"String of beads" appearance on horizontal abdominal view X-ray is suggestive of:
What condition is indicated by the double bubble sign on an abdominal X-ray?
Investigation with least radiation dose in the diagnosis of Meckel's diverticulum is -
What is the echogenic lesion size criterion for chronic pancreatitis?
What is the CT scan finding in a carotid cavernous sinus fistula?
On imaging, diffuse axonal injury is characterized by -
What is the investigation of choice for whole body imaging in metastatic breast cancer?
What is the maximum radiation dose (in Gray) that bone tissue can tolerate?
Which imaging modality is most effective in differentiating between epidermoid cyst and arachnoid cyst?
In which condition is the 'Picture frame vertebra' seen?
NEET-PG 2013 - Radiology NEET-PG Practice Questions and MCQs
Question 31: "String of beads" appearance on horizontal abdominal view X-ray is suggestive of:
- A. Intussusception
- B. Sigmoid volvulus
- C. Small bowel obstruction (Correct Answer)
- D. Large bowel obstruction
Explanation: ***Small bowel obstruction*** - A "string of beads" appearance on a horizontal abdominal view X-ray refers to small gas bubbles trapped between the valvulae conniventes in a dilated small bowel loop. - This finding is highly suggestive of **complete small bowel obstruction**, particularly when accompanied by multiple air-fluid levels and dilated bowel loops. *Intussusception* - While it causes obstruction, intussusception usually appears as a **target sign** (doughnut sign) on ultrasound or a **meniscus sign** on barium enema, not a string of beads on plain X-ray. - Plain X-rays may show signs of **bowel obstruction**, but the string of beads is not characteristic. *Sigmoid volvulus* - Sigmoid volvulus is characterized by a **dilated loop of colon** forming an inverted U-shape, often described as a **coffee bean sign** or **omega sign**, on plain X-ray. - This involves the large bowel, and the "string of beads" specifically relates to gas in the small bowel. *Large bowel obstruction* - Large bowel obstruction typically presents with a **dilated colon** proximal to the obstruction and a collapsed distal colon, often with absent or minimal gas in the rectum and sigmoid. - While air-fluid levels can be present, the "string of beads" is a specific sign of gas within dilated small bowel loops, distinguishing it from most large bowel obstructions.
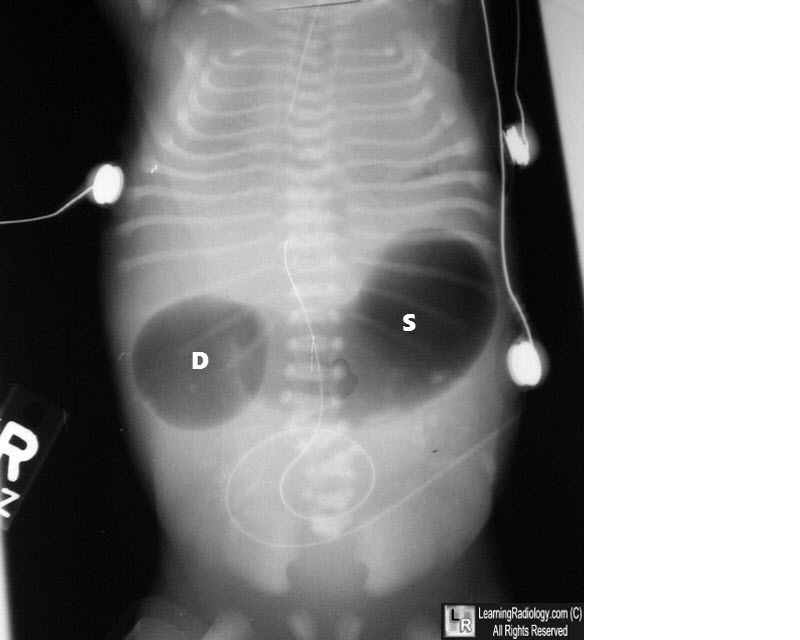
Question 32: What condition is indicated by the double bubble sign on an abdominal X-ray?
- A. Duodenal stenosis
- B. Volvulus
- C. All of the options
- D. Duodenal atresia (Correct Answer)
Explanation: ***Duodenal atresia*** - The **double bubble sign** on an abdominal X-ray is pathognomonic for **duodenal atresia**, characterized by two air-filled bubbles: one in the stomach and one in the proximal duodenum, separated by the pylorus. - This congenital anomaly results from a complete obstruction of the duodenum, preventing the passage of air and fluid past this point. *Duodenal stenosis* - While also an obstruction of the duodenum, **duodenal stenosis** is an incomplete obstruction, meaning some gas will pass beyond the duodenum. - This would result in gas being present in the distal bowel, which is not seen with a classic "double bubble" where the bowel distal to the duodenum is gasless. *Volvulus* - **Volvulus** involves the twisting of a loop of intestine, leading to obstruction and potentially ischemia. - While it can cause obstruction, it typically presents with a "corkscrew" appearance on an upper GI series or signs of diffuse bowel distension, not the isolated double bubble. *All of the options* - The double bubble sign is highly specific to **duodenal atresia** due to the complete obstruction it signifies. - Other conditions like duodenal stenosis and volvulus cause different radiological patterns, making this option incorrect.
Question 33: Investigation with least radiation dose in the diagnosis of Meckel's diverticulum is -
- A. MRI
- B. CT
- C. Contrast radiography
- D. Technetium -99m scanning (Correct Answer)
Explanation: ***Technetium-99m scanning*** - **Technetium-99m pertechnetate scan** (Meckel's scan) is the **gold standard investigation** for diagnosing Meckel's diverticulum with ectopic gastric mucosa - Among the investigations that can actually **diagnose Meckel's diverticulum**, it has the **lowest radiation dose** (approximately 1-2 mSv) - The radioisotope is specifically taken up by ectopic gastric mucosa, providing both diagnostic utility and relatively low radiation exposure - **Sensitivity: 85-95%** for detecting ectopic gastric mucosa in Meckel's diverticulum - The radiation dose is comparable to a few months of natural background radiation and significantly lower than CT or contrast studies *MRI* - While **MRI uses no ionizing radiation**, it is **not a standard or practical investigation** for diagnosing Meckel's diverticulum - MRI cannot identify ectopic gastric mucosa specifically - It is rarely used in clinical practice for this indication - The question asks about investigation "in the diagnosis" of Meckel's diverticulum, implying a test that is actually used diagnostically *CT* - **Computed Tomography (CT)** delivers a **high radiation dose** (typically 5-10 mSv or more) - While it can identify structural abnormalities, it is not specific for Meckel's diverticulum - Not the first-line investigation for this condition *Contrast radiography* - **Contrast studies** (barium studies) use **moderate ionizing radiation** (3-5 mSv) - Limited utility in diagnosing Meckel's diverticulum as it primarily assesses luminal patency - Cannot identify ectopic gastric mucosa - Lower sensitivity compared to Tc-99m scanning
Question 34: What is the echogenic lesion size criterion for chronic pancreatitis?
- A. > 2 mm
- B. > 3 mm (Correct Answer)
- C. > 1 mm
- D. > 4 mm
Explanation: ***> 3 mm*** - An echogenic lesion **greater than 3 mm** in size is a diagnostic criterion for **chronic pancreatitis** when observed on ultrasound imaging. - This represents one of the **major features** in ultrasound diagnosis of chronic pancreatitis, particularly when echogenic foci demonstrate acoustic shadowing (suggesting calcifications). - This criterion is part of established diagnostic frameworks and helps differentiate pathological calcifications from minor, non-specific findings. *> 4 mm* - While a **4 mm threshold** would indicate significant findings, the established diagnostic criterion for chronic pancreatitis uses **> 3 mm** as the cutoff. - Using a higher threshold would reduce sensitivity for detecting chronic pancreatitis. *> 2 mm* - A lesion larger than **2 mm** is generally considered below the established diagnostic threshold for **chronic pancreatitis**. - This size may represent early changes or incidental findings that are not yet definitive for diagnosis. *> 1 mm* - A lesion **greater than 1 mm** is too small to be a definitive criterion for **chronic pancreatitis** and could represent minor, non-pathological findings. - Such small echogenic foci lack sufficient specificity for diagnosing chronic pancreatic disease.
Question 35: What is the CT scan finding in a carotid cavernous sinus fistula?
- A. Enlarged superior ophthalmic vein (Correct Answer)
- B. Enlarged inferior ophthalmic vein
- C. Enlarged superior ophthalmic artery
- D. Enlarged inferior ophthalmic artery
Explanation: ***Enlarged superior ophthalmic vein*** * A carotid cavernous sinus fistula (CCSF) causes **high-pressure arterial blood** to shunt into the **venous system** of the cavernous sinus. * This increased pressure leads to retrograde flow and congestion in the draining veins, most notably the **superior ophthalmic vein**, causing its dilation. *Enlarged inferior ophthalmic vein* * While the inferior ophthalmic vein can also be involved in some cases of CCSF, the **superior ophthalmic vein** is typically more prominent and consistently affected due to its primary drainage pathway. * The inferior ophthalmic vein is less frequently the primary or most notable imaging finding compared to the superior ophthalmic vein. *Enlarged superior ophthalmic artery* * A CCSF involves an abnormal connection between the **carotid artery** (an artery) and the **cavernous sinus** (a venous structure), leading to venous, not arterial, dilation. * Arteries in the orbital region, like the superior ophthalmic artery, would not typically enlarge as a direct result of increased venous pressure in the cavernous sinus. *Enlarged inferior ophthalmic artery* * Similar to the superior ophthalmic artery, the inferior ophthalmic artery is an **arterial structure** and would not enlarge due to a high-flow arteriovenous shunt within the cavernous sinus. * The pathological changes in CCSF are primarily observed in the **venous drainage pathways**.
Question 36: On imaging, diffuse axonal injury is characterized by -
- A. Patchy ill-defined low density lesion mixed with small hyperdensities of petechial hemorrhage
- B. Crescentic extra-axial hematoma
- C. White matter lucencies
- D. Multiple small petechial hemorrhages (Correct Answer)
Explanation: ***Multiple small petechial hemorrhages*** - Diffuse axonal injury (DAI) is characterized on imaging by numerous **small petechial hemorrhages** at the **gray-white matter junction**, **corpus callosum**, and **brainstem**. - These microhemorrhages are the **hallmark imaging finding** and are best visualized on MRI (GRE/SWI sequences), though they can be seen on CT as small hyperdensities. - This is the **most specific** and characteristic finding that defines DAI. *Patchy ill-defined low density lesion mixed with small hyperdensities of petechial hemorrhage* - While this description can be seen in DAI (combining edema with microhemorrhages), it is **less specific** and could represent other entities. - This mixed pattern is more commonly associated with **contusions** where there is more prominent parenchymal injury with larger areas of edema and hemorrhage. - DAI classically shows predominantly **small punctate hemorrhages** rather than larger patchy low-density lesions. *Crescentic extra-axial hematoma* - A crescentic extra-axial collection describes a **subdural hematoma**, which is an entirely separate entity from DAI. - Subdural hematomas are located between the dura and arachnoid membranes, whereas DAI involves direct **axonal shearing injury** within brain parenchyma. *White matter lucencies* - This is a **non-specific finding** that can occur in many conditions including ischemia, demyelination, and chronic small vessel disease. - While DAI can cause white matter edema leading to lucencies, this does not capture the **characteristic petechial hemorrhages** that define the condition on imaging.
Question 37: What is the investigation of choice for whole body imaging in metastatic breast cancer?
- A. Angiography
- B. Venography
- C. Magnetic Resonance Imaging
- D. CT Scan (Correct Answer)
Explanation: ***CT Scan (Correct answer for NEET 2013)*** - **Contrast-enhanced CT scan** was the standard imaging modality for **whole-body staging** in metastatic breast cancer at the time of this exam (2013). - CT offers **excellent spatial resolution** for detecting metastases in **bone, lung, liver, and lymph nodes**. - It is widely available, relatively quick, and provides comprehensive anatomical information. - **Modern Update:** While CT was the standard in 2013, **PET-CT (FDG-PET/CT) is now considered the gold standard** for whole-body staging in metastatic breast cancer due to its combined metabolic and anatomical imaging capabilities. However, PET-CT was not among the options in this historical question. *Magnetic Resonance Imaging* - **MRI** is highly sensitive for specific sites, particularly for **brain metastases** and **bone metastases (especially spine and bone marrow)**. - **Whole-body MRI** protocols are emerging but require longer acquisition times and specialized equipment. - Not ideal as a single first-line modality for comprehensive whole-body staging compared to CT (or modern PET-CT). *Angiography* - **Angiography** is an invasive vascular imaging procedure used to visualize **arterial blood flow**. - It has **no role in routine metastatic screening or staging** of breast cancer. - Reserved for specific indications like preoperative vascular mapping or interventional procedures. *Venography* - **Venography** specifically visualizes **venous structures** and is used to detect venous thrombosis or venous obstructions. - It is **not applicable** for detecting solid organ metastases, bone lesions, or lymph node involvement in cancer staging.
Question 38: What is the maximum radiation dose (in Gray) that bone tissue can tolerate?
- A. 50 Gray (Correct Answer)
- B. 30 Gray
- C. 20 Gray
- D. 40 Gray
Explanation: ***Correct Option: 50 Gray*** - The **maximum radiation tolerance dose** for bone tissue is approximately **50-60 Gray (Gy)** based on radiobiology literature and clinical practice. - Among the given options, **50 Gy** represents the most appropriate threshold for bone tolerance. - According to **Emami et al. tolerance doses** and **QUANTEC guidelines**, bone can typically tolerate up to 60 Gy without significant risk of complications. - Doses approaching or exceeding **60 Gy** carry increased risk of **osteoradionecrosis**, particularly in the **mandible and weight-bearing bones**. - **Clinical significance**: In radiation therapy planning, doses of 50-60 Gy to bone are commonly used therapeutically for tumors involving or adjacent to bone. *Incorrect Option: 40 Gray* - 40 Gy is **below the accepted tolerance threshold** for bone tissue. - This dose is generally **well-tolerated** by bone without significant risk of necrosis or fracture. - Commonly used in palliative and definitive radiation protocols without major bone complications. *Incorrect Option: 30 Gray* - 30 Gy is **considerably below** the tolerance limit for bone. - This dose level is **safe for bone tissue** and carries minimal risk of radiation-induced bone damage. - Often used in palliative treatments with excellent bone tolerance. *Incorrect Option: 20 Gray* - 20 Gy is a **low radiation dose** from the perspective of bone tolerance. - This dose is **highly unlikely** to cause any significant bone damage or complications. - Represents a conservative therapeutic dose well within safety margins.
Question 39: Which imaging modality is most effective in differentiating between epidermoid cyst and arachnoid cyst?
- A. Magnetic Resonance Imaging (MRI) (Correct Answer)
- B. Ultrasound (USG)
- C. Computed Tomography (CT) scan
- D. Positron Emission Tomography (PET) scan
Explanation: ***Magnetic Resonance Imaging (MRI)*** - **MRI** is superior for differentiating epidermoid and arachnoid cysts due to its excellent **soft tissue contrast** and ability to detect fluid signal characteristics. - **Diffusion-weighted imaging (DWI)**, a specific MRI sequence, is crucial; **epidermoid cysts** show high signal on DWI (diffusion restriction) due to their keratin content, while **arachnoid cysts** follow CSF signal on all sequences and do not restrict diffusion. *Ultrasound (USG)* - **Ultrasound** has limited utility for intracranial lesions in adults due to the bony skull, which prevents sound wave penetration. - It may be used in infants through the fontanelles but lacks the resolution and specific sequences needed to characterize these cysts. *Computed Tomography (CT) scan* - While a **CT scan** can identify these cysts as hypodense lesions, it lacks the detailed **tissue characterization** and signal patterns provided by MRI. - Both cysts would appear as **hypodense lesions**, making differentiation difficult based on density alone, especially after contrast administration. *Positron Emission Tomography (PET) scan* - A **PET scan** primarily assesses metabolic activity and would not effectively differentiate between benign **non-metabolic cysts** like epidermoid and arachnoid cysts. - It is more commonly used for detecting **malignancies** or assessing brain activity patterns, not for structural differentiation of fluid-filled lesions.
Question 40: In which condition is the 'Picture frame vertebra' seen?
- A. Paget disease (Correct Answer)
- B. Osteopetrosis (marble bone disease)
- C. Ankylosing spondylitis (AS)
- D. Osteoporosis
Explanation: ***Paget disease*** - The "picture frame vertebra" sign is a classic radiographic finding in **Paget disease**, characterized by **cortical thickening** and sclerosis around the vertebral body circumference, resembling a picture frame. - This appearance is due to the disordered bone remodeling processes (increased osteoclastic bone resorption followed by disorganized osteoblastic new bone formation) characteristic of Paget disease. *Osteopetrosis (marble bone disease)* - Osteopetrosis is characterized by **increased bone density** due to defective osteoclast function, leading to bones that are dense but brittle. - It does not typically present with the specific "picture frame" appearance of individual vertebrae, but rather with diffuse sclerosis of bones. *Ankylosing spondylitis (AS)* - Ankylosing spondylitis primarily affects the **axial skeleton**, causing inflammation and eventual fusion of the vertebrae (leading to a "bamboo spine" appearance). - While it involves the spine, it does not produce the "picture frame" vertebral sign seen in Paget disease. *Osteoporosis* - Osteoporosis is characterized by **reduced bone mass** and microstructural deterioration of bone tissue, leading to increased bone fragility and fracture risk. - Radiographically, it shows **decreased bone density** and possible vertebral compression fractures, which is the opposite of the increased bone density and cortical thickening seen in the "picture frame" sign.