
Trauma/Emergencies — MCQs

On this page
A 24-year-old man is brought to the emergency department 30 minutes after being involved in a high-speed motor vehicle collision in which he was a restrained driver. On arrival, he is alert and oriented. His pulse is 112/min, respirations are 29/min, and blood pressure is 100/60 mm Hg. The pupils are equal and reactive to light. There is a 3-cm laceration over the forehead and multiple bruises over the trunk. The lungs are clear to auscultation. Cardiac examination shows no abnormalities. The abdomen is soft and nontender. The right knee is swollen and tender; range of motion is limited by pain. Infusion of 0.9% saline is begun and intravenous acetaminophen is administered. Two hours later, blood-tinged fluid spontaneously drains from both nostrils, and is made worse by leaning forward. On a piece of gauze, it shows up as a rapidly-expanding clear ring of fluid surrounding blood. Further evaluation of this patient is most likely to show which of the following?
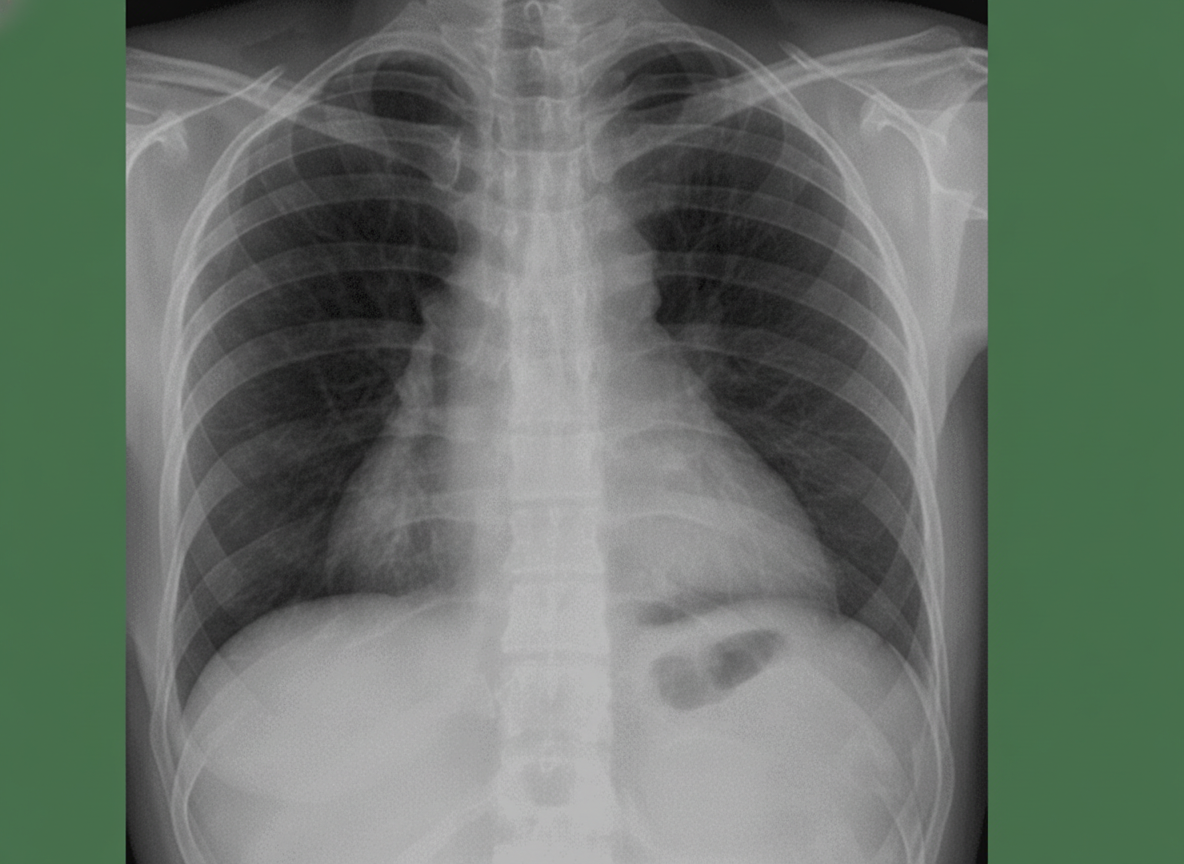
A 50-year-old man presents with severe chest pain for a week. His pain increases with breathing and is localized to the right. He has tried over-the-counter medications at home, but they did not help. The patient has a 20-pack-year smoking history and currently smokes 2 packs of cigarettes daily, and he drinks 3 to 4 cans of beer daily before dinner. His temperature is 39.1°C (102.3°F), blood pressure is 127/85 mm Hg, pulse is 109/min, and respirations are 20/min. Respiratory examination shows dullness to percussion from the 7th rib inferiorly at the right midaxillary line, decreased vocal tactile fremitus, and diminished breath sounds in the same area. Chest radiograph is shown in the image. The patient is prepared for thoracocentesis. Which of the following locations would be the most appropriate for insertion of a chest tube?
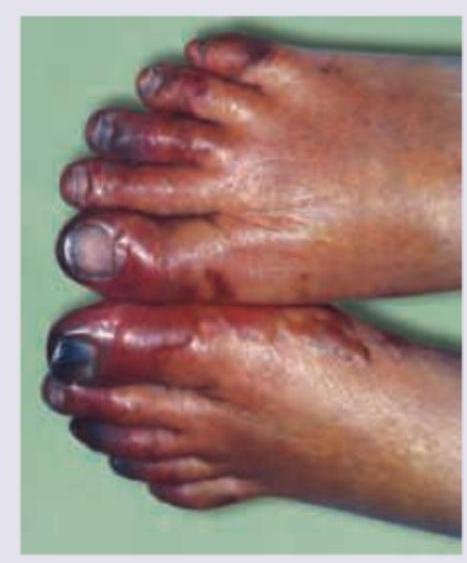
A 75-year-old man presents to the emergency department because of pain in his left thigh and left calf for the past 3 months. The pain occurs at rest, increases with walking, and is mildly improved by hanging the foot off the bed. He has had hypertension for 25 years and type 2 diabetes mellitus for 30 years. He has smoked 30–40 cigarettes per day for the past 45 years. On examination, femoral, popliteal, and dorsalis pedis pulses are faint on both sides. The patient’s foot is shown in the image. Resting ankle-brachial index (ABI) is found to be 0.30. Antiplatelet therapy and aggressive risk factors modifications are initiated. Which of the following is the best next step for this patient?
A 27-year-old man presents to the emergency department after being hit by a car while riding his bike. The patient was brought in with his airway intact, vitals stable, and with a C-collar on. Physical exam is notable for bruising over the patient’s head and a confused man with a Glasgow coma scale of 11. It is noticed that the patient has a very irregular pattern of breathing. Repeat vitals demonstrate his temperature is 97.5°F (36.4°C), blood pressure is 172/102 mmHg, pulse is 55/min, respirations are 22/min and irregular, and oxygen saturation is 94% on room air. Which of the following interventions are most likely to improve this patient's vital signs?
A 23-year-old woman comes to the office because of a 2-day history of right knee pain. She says, "I can't run anymore because my knee hurts." The pain is localized "somewhere under the kneecap" and is achy, rated 5/10, but increases to 8/10 with prolonged sitting. She reports an occasional "popping" sound and sensation when she rises from a seated position. She has no history of trauma to the knee. She had a right clavicular fracture 2 years ago that was treated with a shoulder sling. She takes a daily multivitamin and has no known drug allergies. She does not smoke and drinks up to three glasses of wine weekly. Vital signs: Temperature 37°C (98.6°F), pulse 65/min, respirations 15/min, blood pressure 108/62 mm Hg. Height 173 cm (5 ft 8 in), weight 54 kg (119 lb), BMI 18 kg/m². Physical examination shows no acute distress. Pulmonary examination shows lungs clear to auscultation. Cardiac examination shows regular rate and rhythm with normal S1 and S2; no murmurs, rubs, or gallops. The abdomen is thin with no tenderness, guarding, masses, bruits, or hepatosplenomegaly. Extremities show no joint erythema, edema, or warmth; dorsalis pedis, radial, and femoral pulses are intact. Musculoskeletal examination shows diffuse tenderness to palpation over the right anterior knee, worse with full extension of the knee; no associated effusion or erythema; full, symmetric strength of quadriceps, hip abductors, and hip external rotators; crepitus with knee range of motion; and antalgic gait. Neurologic examination shows the patient is alert and oriented with cranial nerves grossly intact and no focal neurologic deficits. Which of the following is the most appropriate next step in management?
A 16-year-old man presents to the emergency department with a 2-hour history of sudden-onset abdominal pain. He was playing football when his symptoms started. The patient’s past medical history is notable only for asthma. Social history is notable for unprotected sex with 4 women in the past month. His temperature is 99.3°F (37.4°C), blood pressure is 120/88 mmHg, pulse is 117/min, respirations are 14/min, and oxygen saturation is 99% on room air. Physical exam is noted for a non-tender abdomen. Testicular exam reveals a right testicle which is elevated with a horizontal lie and the scrotum is neither swollen nor discolored. Which of the following is the most likely diagnosis?
A 22-year-old woman in the intensive care unit has had persistent oozing from the margins of wounds for 2 hours that is not controlled by pressure bandages. She was admitted to the hospital 13 hours ago following a high-speed motor vehicle collision. Initial focused assessment with sonography for trauma was negative. An x-ray survey showed opacification of the right lung field and fractures of multiple ribs, the tibia, fibula, calcaneus, right acetabulum, and bilateral pubic rami. Laboratory studies showed a hemoglobin concentration of 14.8 g/dL, leukocyte count of 10,300/mm3, platelet count of 175,000/mm3, and blood glucose concentration of 77 mg/dL. Infusion of 0.9% saline was begun. Multiple lacerations on the forehead and extremities were sutured, and fractures were stabilized. Repeat laboratory studies now show a hemoglobin concentration of 12.4 g/dL, platelet count of 102,000/mm3, prothrombin time of 26 seconds (INR=1.8), and activated partial thromboplastin time of 63 seconds. Which of the following is the next best step in management?
A 27-year-old male arrives in the emergency department with a stab wound over the precordial chest wall. The patient is in distress and is cold, sweaty, and pale. Initial physical examination is significant for muffled heart sounds, distended neck veins, and a 3 cm stab wound near the left sternal border. Breath sounds are present bilaterally without evidence of tracheal deviation. Which of the following additional findings would be expected on further evaluation?
A 34-year-old woman presents to the emergency department with moderate right wrist pain after falling on her outstretched hand. She has numbness in the lateral 3 digits. The patient has no known previous medical conditions. Her family history is not pertinent, and she currently takes no medications. Physical examination shows her blood pressure is 134/82 mm Hg, the respirations are 14/min, the pulse is 87/min, and the temperature is 36.7°C (98.0°F). When asked to make a fist, the patient is unable to flex the lateral 2 digits. Tapping the anterior portion of her wrist elicits tingling in the lateral 3 digits. The patient is taken to get an X-ray. Which of the following is the most likely diagnosis for this patient's injury?
A 66-year-old female with hypertension and a recent history of acute ST-elevation myocardial infarction (STEMI) 6 days previous, treated with percutaneous transluminal angioplasty (PTA), presents with sudden onset chest pain, shortness of breath, diaphoresis, and syncope. Vitals are temperature 37°C (98.6°F), blood pressure 80/50 mm Hg, pulse 125/min, respirations 12/min, and oxygen saturation 92% on room air. On physical examination, the patient is pale and unresponsive. Cardiac exam reveals tachycardia and a pronounced holosystolic murmur loudest at the apex and radiates to the back. Lungs are clear to auscultation. Chest X-ray shows cardiomegaly with clear lung fields. ECG is significant for ST elevations in the precordial leads (V2-V4) and low-voltage QRS complexes. Emergency transthoracic echocardiography shows a left ventricular wall motion abnormality along with a significant pericardial effusion. The patient is intubated, and aggressive fluid resuscitation is initiated. What is the next best step in management?
Practice by Chapter
Chest trauma management
Practice Questions
Head trauma management
Practice Questions
Spinal trauma
Practice Questions
Blunt abdominal trauma
Practice Questions
Penetrating abdominal trauma
Practice Questions
Pelvic fractures and hemorrhage
Practice Questions
Extremity trauma and vascular injuries
Practice Questions
Burns assessment and management
Practice Questions
Traumatic shock management
Practice Questions
Resuscitative thoracotomy
Practice Questions
Focused Assessment with Sonography in Trauma (FAST)
Practice Questions
Trauma in pregnancy
Practice Questions
Pediatric trauma considerations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app