
Abdominal emergencies — MCQs

On this page
A 57-year-old man presents to the emergency department after an episode of syncope. He states that he was at home when he suddenly felt weak and experienced back pain that has been persistent. He states that he vomited forcefully several times after the episode. The patient has a past medical history of diabetes, hypertension, dyslipidemia, and depression. He smokes 1.5 packs of cigarettes per day and drinks 10 alcoholic beverages each night. His temperature is 97.5°F (36.4°C), blood pressure is 107/48 mmHg, pulse is 130/min, respirations are 19/min, and oxygen saturation is 99% on room air. A chest radiograph is within normal limits. Physical exam is notable for abdominal tenderness and a man resting in an antalgic position. Urinalysis is currently pending but reveals a concentrated urine sample. Which of the following is the most likely diagnosis?
A 12-year-old boy is brought to the emergency room by his mother with complaints of abdominal pain and fever that started 24 hours ago. On further questioning, the mother says that her son vomited twice and has constipation that started approximately 1 and one-half days ago. The medical history is benign. The vital signs are as follows: heart rate 103/min, respiratory rate of 20/min, temperature 38.7°C (101.66°F), and blood pressure 109/69 mm Hg. On physical examination, there is severe right lower quadrant abdominal tenderness on palpation. Which of the following is the most likely cause for this patient’s symptoms?
A 68-year-old man presents to the emergency department with left lower quadrant abdominal pain and fever for 1 day. He states during this time frame he has had weight loss and a decreased appetite. The patient had surgery for a ruptured Achilles tendon 1 month ago and is still recovering but is otherwise generally healthy. His temperature is 102°F (38.9°C), blood pressure is 154/94 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 98% on room air. Physical exam is remarkable for an uncomfortable and thin man with left lower quadrant abdominal tenderness without rebound findings. Fecal occult test for blood is positive. Laboratory studies are ordered as seen below. Hemoglobin: 10 g/dL Hematocrit: 30% Leukocyte count: 3,500/mm^3 with normal differential Platelet count: 157,000/mm^3 Which of the following is the most appropriate next step in management?
A 54-year-old man with lymphoma presents to his oncologist with severe abdominal pain and flank pain. He says that the pain started 2 days ago and has gotten worse over time. He has also not been able to urinate over the same time period. On presentation, his temperature is 99°F (37.2°C), blood pressure is 110/72 mmHg, pulse is 105/min, and respirations are 12/min. Physical exam reveals bilateral flank tenderness. Labs results are shown below: Blood urea nitrogen: 34 mg/dL Creatinine: 3.7 mg/dl Urine osmolality: 228 mOsm/kg Renal ultrasonography shows dilation of the kidneys bilaterally with a normal-sized bladder. Which of the following would most likely be beneficial in treating this patient's condition?
A 19-year-old man comes to the emergency department because of abdominal pain, nausea, and vomiting for 4 hours. Initially, the pain was dull and located diffusely around his umbilicus, but it has now become sharper and moved towards his lower right side. He has no history of serious illness and takes no medications. His temperature is 38.2°C (100.7°F) and blood pressure is 123/80 mm Hg. Physical examination shows severe right lower quadrant tenderness without rebound or guarding; bowel sounds are decreased. His hemoglobin concentration is 14.2 g/dL, leukocyte count is 12,000/mm3, and platelet count is 280,000/mm3. Abdominal ultrasonography shows a dilated noncompressible appendix with distinct wall layers and echogenic periappendiceal fat. Intravenous fluid resuscitation is begun. Which of the following is the most appropriate next step in management?
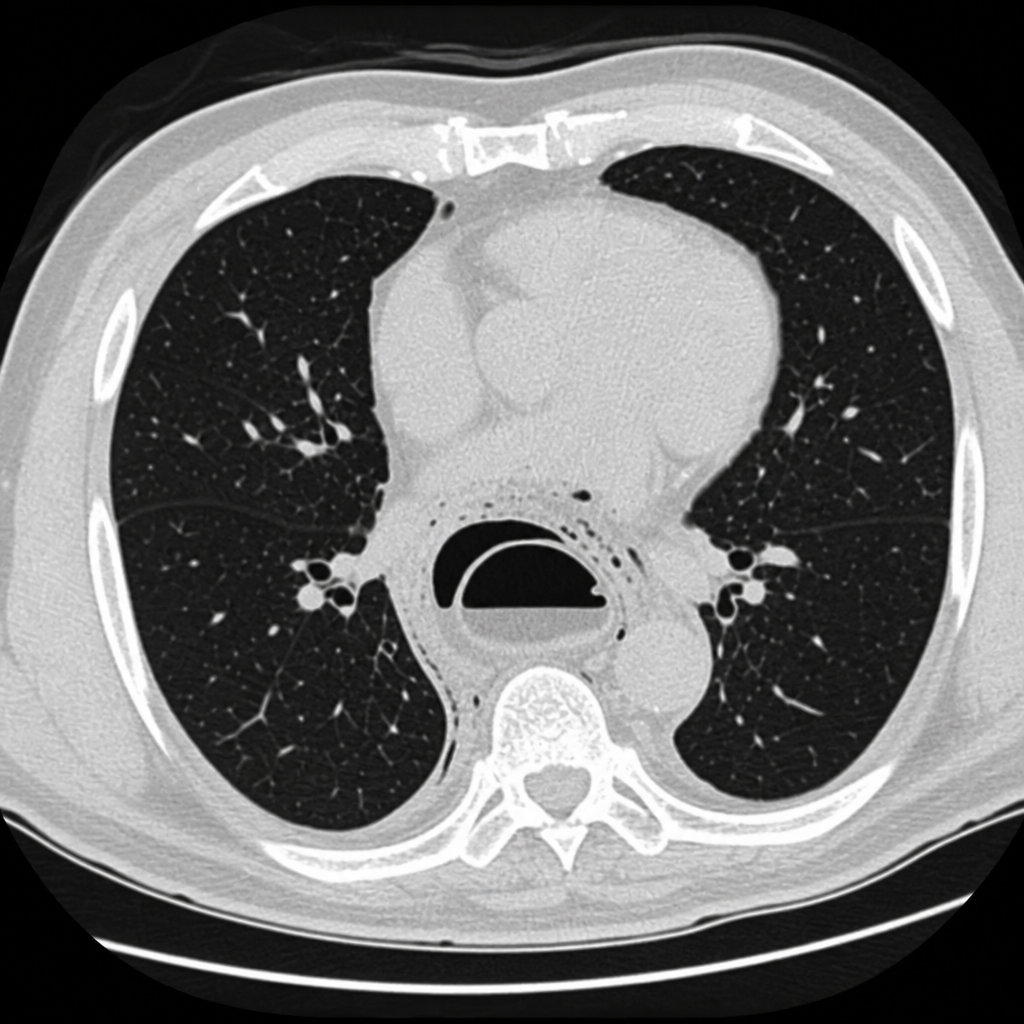
A 64-year-old man is brought to the emergency department because of a 2-hour history of nausea, vomiting, and retrosternal pain that radiates to the back. Abdominal examination shows tenderness to palpation in the epigastric area. A CT scan of the patient's chest is shown. Which of the following is the most likely diagnosis?
A 29-year-old woman, gravida 1, para 1, comes to the physician for the evaluation of a painful mass in her left breast for several days. She has no fevers or chills. She has not noticed any changes in the right breast. She has no history of serious illness. Her last menstrual period was 3 weeks ago. She appears anxious. Her temperature is 37°C (98.6°F), pulse is 80/min, respirations are 13/min, and blood pressure is 130/75 mm Hg. Examination shows a palpable, mobile, tender mass in the left upper quadrant of the breast. Ultrasound shows a 1.75-cm, well-circumscribed anechoic mass with posterior acoustic enhancement. The patient says that she is very concerned that she may have breast cancer and wishes further diagnostic testing. Which of the following is the most appropriate next step in the management of this patient?
A 61-year-old man comes to the physician because of a 2-month history of severe chest discomfort. The chest discomfort usually occurs after heavy meals or eating in the late evening and lasts several hours. He has nausea sometimes but no vomiting. He has also had an occasional nighttime cough during this period. He has hypertension and type 2 diabetes mellitus. He has smoked one pack of cigarettes daily for the past 41 years and drinks one beer daily. Current medications include metformin, naproxen, enalapril,and sitagliptin. He is 177 cm (5 ft 10 in) tall and weighs 135 kg (297 lb); BMI is 43 kg/m2. Vital signs are within normal limits. Cardiopulmonary examination shows no abnormalities. The abdomen is soft and nontender. Laboratory studies are within the reference ranges. An ECG shows no abnormalities. An upper endoscopy shows that the Z-line is located 4 cm above the diaphragmatic hiatus and reveals the presence of a 1.5-cm esophageal ulcer with an erythematous base and without bleeding. The physician recommends weight loss as well as smoking and alcohol cessation. Treatment with omeprazole is begun. One month later, his symptoms are unchanged. Which of the following is the most appropriate next step in management?
A 69-year-old male presents to the Emergency Department with bilious vomiting that started within the past 24 hours. His medical history is significant for hypertension, hyperlipidemia, and a myocardial infarction six months ago. His past surgical history is significant for a laparotomy 20 years ago for a perforated diverticulum. Most recently he had some dental work done and has been on narcotic pain medicine for the past week. He reports constipation and obstipation. He is afebrile with a blood pressure of 146/92 mm Hg and a heart rate of 116/min. His abdominal exam reveals multiple well-healed scars with distension but no tenderness. An abdominal/pelvic CT scan reveals dilated small bowel with a transition point to normal caliber bowel distally. When did the cause of his pathology commence?
A 32-year-old man comes to the emergency department because of recurrent episodes of vomiting for 1 day. He has had over 15 episodes of bilious vomiting. During this period he has had cramping abdominal pain but has not had a bowel movement or passed flatus. He does not have fever or diarrhea. He was diagnosed with Crohn disease at the age of 28 years which has been well controlled with oral mesalamine. He underwent a partial small bowel resection for midgut volvulus at birth. His other medications include vitamin B12, folic acid, loperamide, ferrous sulfate, and vitamin D3. He appears uncomfortable and his lips are parched. His temperature is 37.1°C (99.3°F), pulse is 103/min, and blood pressure is 104/70 mm Hg. The abdomen is distended, tympanitic, and tender to palpation over the periumbilical area and the right lower quadrant. Rectal examination is unremarkable. A CT scan of the abdomen shows multiple dilated loops of small bowel with a transition zone in the mid to distal ileum. After 24 hours of conservative management with IV fluid resuscitation, nasogastric bowel decompression, promethazine, and analgesia, his condition does not improve and a laparotomy is scheduled. During the laparotomy, two discrete strictures are noted in the mid-ileum, around 20 cm apart. Which of the following is the most appropriate next step in management?
Practice by Chapter
Acute appendicitis
Practice Questions
Acute cholecystitis
Practice Questions
Small bowel obstruction
Practice Questions
Large bowel obstruction
Practice Questions
Mesenteric ischemia
Practice Questions
Gastrointestinal perforation
Practice Questions
Abdominal compartment syndrome
Practice Questions
Acute pancreatitis management
Practice Questions
Diverticulitis
Practice Questions
Incarcerated/strangulated hernias
Practice Questions
Non-operative management principles
Practice Questions
Diagnostic approach to acute abdomen
Practice Questions
Damage control surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app