
Abdominal emergencies — MCQs

On this page
A 16-year-old boy comes to the physician because of painless enlargement of his left testis for the past 2 weeks. The patient reports that the enlargement is worse in the evenings, especially after playing soccer. He has not had any trauma to the testes. There is no personal or family history of serious illness. Vital signs are within normal limits. Examination shows multiple cord-like structures above the left testes. The findings are more prominent while standing. The cord-like structures disappear in the supine position. The testes are normal on palpation. The patient is at greatest risk of developing which of the following complications?
A 42-year-old man presents to the emergency department with abdominal pain. The patient was at home watching television when he experienced sudden and severe abdominal pain that prompted him to instantly call emergency medical services. The patient has a past medical history of obesity, smoking, alcoholism, hypertension, and osteoarthritis. His current medications include lisinopril and ibuprofen. His temperature is 98.5°F (36.9°C), blood pressure is 120/97 mmHg, pulse is 130/min, respirations are 22/min, and oxygen saturation is 97% on room air. The patient is in an antalgic position on the stretcher. His abdomen is rigid and demonstrates rebound tenderness and hypoactive bowel sounds. What is the next best step in management?
A 35-year-old man is admitted with an acute onset of dysphagia, odynophagia, slight retrosternal chest pain, hypersalivation, and bloody sputum. These symptoms appeared 3 hours ago during a meal when the patient ate fish. The patient’s past medical history is significant for repair of a traumatic esophageal rupture 5 years ago. The patient’s vital signs are as follows: blood pressure 140/90 mm Hg, heart rate 87/min, respiratory rate 16/min, and temperature 36.8℃ (98.2℉). On exam, the patient is pale and breathing deeply. The oral cavity appears normal. The pharynx is erythematous but with no visible lesions. Lungs are clear to auscultation. Cardiovascular examination shows no abnormalities. The abdomen is nondistended and nontender. Which of the following interventions are indicated in this patient?
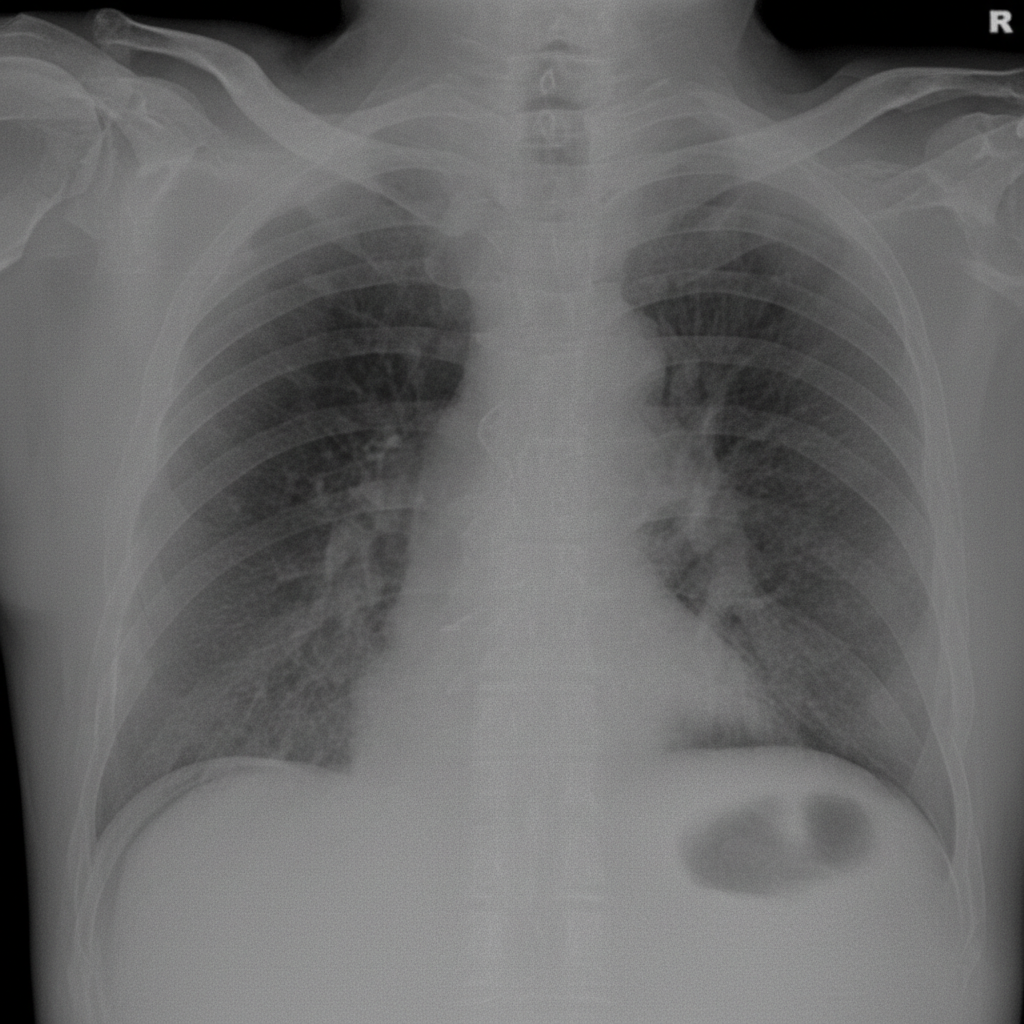
A 56-year-old man is brought to the emergency department after 4 hours of severe abdominal pain with an increase in its intensity over the last hour. His personal history is relevant for peptic ulcer disease and H. pylori infection that is being treated with clarithromycin triple therapy. Upon admission his vital signs are as follows: pulse of 120/min, a respiratory rate of 20/min, body temperature of 39°C (102.2°F), and blood pressure of 90/50 mm Hg. Physical examination reveals significant tenderness over the abdomen. A chest radiograph taken when the patient was standing erect is shown. Which of the following is the next best step in the management of this patient?
A 72-year-old woman comes to the physician for follow-up care. One year ago, she was diagnosed with a 3.8-cm infrarenal aortic aneurysm found incidentally on abdominal ultrasound. She has no complaints. She has hypertension, type 2 diabetes mellitus, and COPD. Current medications include hydrochlorothiazide, lisinopril, glyburide, and an albuterol inhaler. She has smoked a pack of cigarettes daily for 45 years. Her temperature is 37°C (98.6°F), pulse is 90/min, respirations are 12/min, and blood pressure is 145/85 mm Hg. Examination shows a faint abdominal bruit on auscultation. Ultrasonography of the abdomen shows a 4.9-cm saccular dilation of the infrarenal aorta. Which of the following is the most appropriate next step in management?
A 62-year-old man presents to his primary care physician. He was brought in by his daughter as he has refused to see a physician for the past 10 years. The patient has been having worsening abdominal pain. He claims that it was mild initially but has gotten worse over the past week. The patient has been eating lots of vegetables recently to help with his pain. The patient has a past medical history of constipation and a 50 pack-year smoking history. He is not currently taking any medications. On review of systems, the patient endorses trouble defecating and blood that coats his stool. His temperature is 99.5°F (37.5°C), blood pressure is 197/128 mmHg, pulse is 100/min, respirations are 17/min, and oxygen saturation is 98% on room air. On abdominal exam, the patient complains of right upper quadrant tenderness and a palpable liver edge that extends 4 cm beneath the costal margin. Murphy's sign is positive. HEENT exam is notable for poor dentition, normal sclera, and normal extraocular movements. There are no palpable lymph nodes. Laboratory studies are ordered as seen below. Hemoglobin: 9 g/dL Hematocrit: 30% Leukocyte count: 7,500/mm^3 with normal differential Platelet count: 199,000/mm^3 Serum: Na+: 140 mEq/L Cl-: 101 mEq/L K+: 4.0 mEq/L HCO3-: 23 mEq/L BUN: 29 mg/dL Glucose: 197 mg/dL Creatinine: 1.4 mg/dL Ca2+: 10.2 mg/dL Total bilirubin: 1.1 mg/dL AST: 150 U/L ALT: 112 U/L Which of the following is the most likely diagnosis?
A 63-year-old man presents to the ambulatory medical clinic with symptoms of dysphagia and ‘heartburn’, which he states have become more troublesome over the past year. Past medical history is significant for primary hypertension. On physical exam, he is somewhat tender to palpation over his upper abdomen. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 74/min, and respiratory rate 14/min. Barium swallow fluoroscopy demonstrates a subdiaphragmatic gastroesophageal junction, with herniation of the gastric fundus into the left hemithorax. Given the following options, what is the most appropriate next step in the management of this patient’s underlying condition?
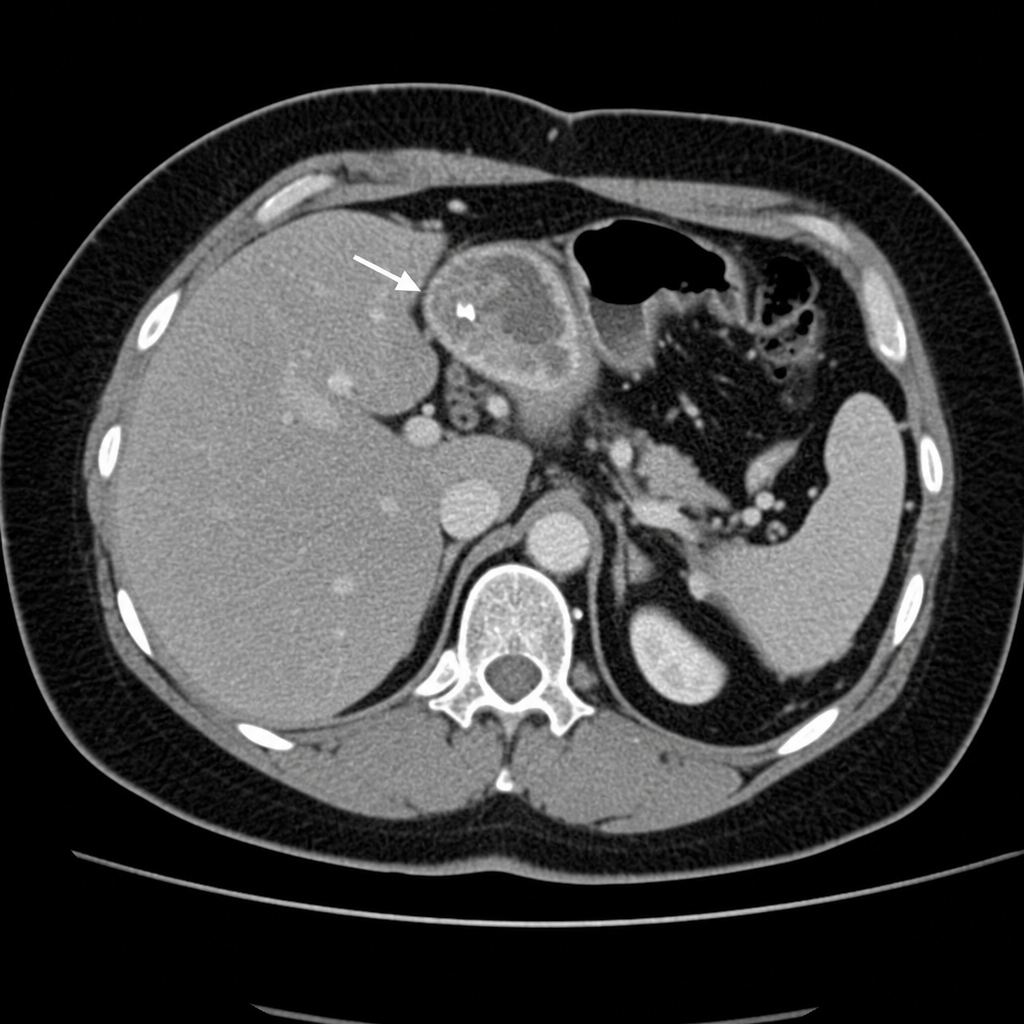
A 47-year-old woman presents to the clinic for a regular health check-up. She is currently asymptomatic but gives a history of recurrent bouts of right upper abdominal pain for 3 years. She further describes the pain as intermittent and localized. She denies any fever, vomiting, difficulty breathing, abnormal bowel habits, hematemesis, or melena. She currently takes multivitamins only. She used to take combined oral contraceptive pills but stopped 3 years ago. Her temperature is 36.7°C (98.1°F), the blood pressure is 126/88 mm Hg, the pulse rate is 84/min, and the respiratory rate is 12/min. Her blood work is normal. An abdominal X-ray is shown in the picture. Based on the imaging findings, the patient is at risk for developing which of the following?
A 46-year-old woman comes to the emergency department because of intermittent abdominal pain and vomiting for 2 days. The abdominal pain is colicky and diffuse. The patient's last bowel movement was 3 days ago. She has had multiple episodes of upper abdominal pain that radiates to her scapulae and vomiting over the past 3 months; her symptoms subsided after taking ibuprofen. She has coronary artery disease, type 2 diabetes mellitus, gastroesophageal reflux disease, and osteoarthritis of both knees. Current medications include aspirin, atorvastatin, rabeprazole, insulin, and ibuprofen. She appears uncomfortable. Her temperature is 39°C (102.2°F), pulse is 111/min, and blood pressure is 108/68 mm Hg. Examination shows dry mucous membranes. The abdomen is distended and tympanitic with diffuse tenderness; bowel sounds are high-pitched. Rectal examination shows a collapsed rectum. Her hemoglobin concentration is 13.8 g/dL, leukocyte count is 14,400/mm3, and platelet count is 312,000/mm3. An x-ray of the abdomen is shown. Which of the following is the most likely cause of this patient's findings?

A 57-year-old man presents with acute-onset nausea and left flank pain. He says his symptoms suddenly started 10 hours ago and have not improved. He describes the pain as severe, colicky, intermittent, and localized to the left flank. The patient denies any fever, chills, or dysuria. His past medical history is significant for nephrolithiasis, incidentally diagnosed 10 months ago on a routine ultrasound, for which he has not been treated. His family history is unremarkable. The patient is afebrile, and his vital signs are within normal limits. On physical examination, he is writhing in pain and moaning. Severe left costovertebral angle tenderness is noted. Gross hematuria is present on urinalysis. A non-contrast CT of the abdomen and pelvis reveals a 12-mm obstructing calculus at the left ureterovesical junction. Initial management, consisting of IV fluid resuscitation, antiemetics, and analgesia, is administered. Which of the following is the best next step in the management of this patient?
Practice by Chapter
Acute appendicitis
Practice Questions
Acute cholecystitis
Practice Questions
Small bowel obstruction
Practice Questions
Large bowel obstruction
Practice Questions
Mesenteric ischemia
Practice Questions
Gastrointestinal perforation
Practice Questions
Abdominal compartment syndrome
Practice Questions
Acute pancreatitis management
Practice Questions
Diverticulitis
Practice Questions
Incarcerated/strangulated hernias
Practice Questions
Non-operative management principles
Practice Questions
Diagnostic approach to acute abdomen
Practice Questions
Damage control surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app