
Cardiology — MCQs

On this page
A 42-year-old woman comes to the physician because of a 12 month history of progressive fatigue and shortness of breath with exertion. Five years ago, she emigrated from Eastern Europe. She has smoked one pack of cigarettes daily for 20 years. She has a history of using methamphetamines and cocaine but quit 5 years ago. Vital signs are within normal limits. Physical examination shows jugular venous pulsations 9 cm above the sternal angle. The lungs are clear to auscultation. There is a normal S1 and a loud, split S2. An impulse can be felt with the fingers left of the sternum. The abdomen is soft and nontender. The fingertips are enlarged and the nails are curved. There is pitting edema around the ankles bilaterally. An x-ray of the chest shows pronounced central pulmonary arteries and a prominent right heart border. Which of the following is most likely to confirm the diagnosis?
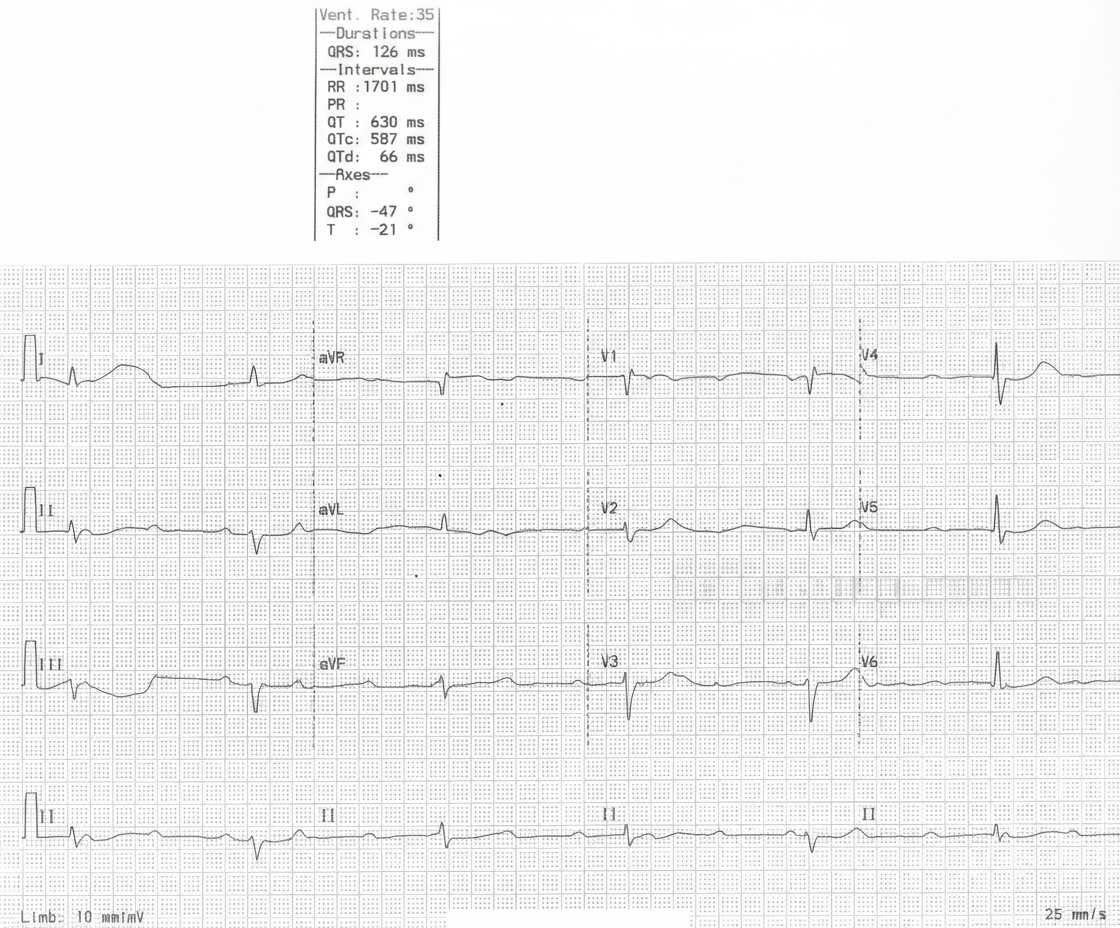
A 29-year-old woman is brought to the emergency department after an episode of syncope. For the past 10 days, she has had dyspnea and palpitations occurring with mild exertion. The patient returned from a hiking trip in Upstate New York 5 weeks ago. Except for an episode of flu with fever and chills a month ago, she has no history of serious illness. Her temperature is 37.3°C (99.1°F), pulse is 45/min, respirations are 21/min, and blood pressure is 148/72 mm Hg. A resting ECG is shown. Two-step serological testing confirms the diagnosis. Which of the following is the most appropriate treatment?
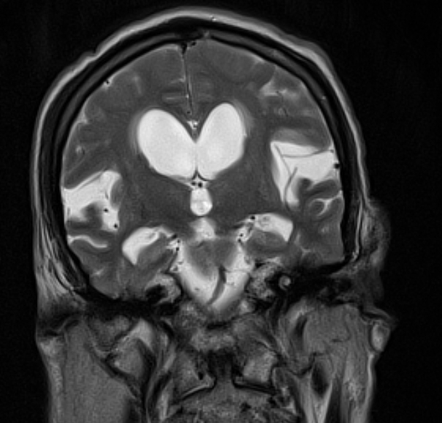
A 73-year-old man is brought in by his wife with a history of progressive personality changes. The patient’s wife says that, over the past 3 years, he has become increasingly aggressive and easily agitated, which is extremely out of character for him. His wife also says that he has had several episodes of urinary incontinence in the past month. He has no significant past medical history. The patient denies any history of smoking, alcohol use, or recreational drug use. The patient is afebrile, and his vital signs are within normal limits. A physical examination is unremarkable. The patient takes the mini-mental status examination (MMSE) and scores 28/30. A T2 magnetic resonance image (MRI) of the head is performed and the results are shown in the exhibit (see image). Which of the following is the next best diagnostic step in the management of this patient?
A 57-year-old man presents to his physician with dyspnea on exertion and rapid heartbeat. He denies any pain during these episodes. He works as a machine operator at a solar panels manufacturer. He has a 21-pack-year history of smoking. The medical history is significant for a perforated ulcer, in which he had to undergo gastric resection and bypass. He also has a history of depression, and he is currently taking escitalopram. The family history is unremarkable. The patient weighs 69 kg (152 lb). His height is 169 cm (5 ft 7 in). The vital signs include: blood pressure 140/90 mm Hg, heart rate 95/min, respiratory rate 12/min, and temperature 36.6℃ (97.9℉). Lung auscultation reveals widespread wheezes. Cardiac auscultation shows decreased S1 and grade 1/6 midsystolic murmur best heard at the apex. Abdominal and neurological examinations show no abnormalities. A subsequent echocardiogram shows increased left ventricular mass and an ejection fraction of 50%. Which of the options is a risk factor for the condition detected in the patient?
A 71-year-old male presents to the emergency department after having a generalized tonic-clonic seizure. His son reports that he does not have a history of seizures but has had increasing confusion and weakness over the last several weeks. An electrolyte panel reveals a sodium level of 120 mEq/L and a serum osmolality of 248 mOsm/kg. His urine is found to have a high urine osmolality. His temperature is 37° C (98.6° F), respirations are 15/min, pulse is 67/min, and blood pressure is 122/88 mm Hg. On examination he is disoriented, his pupils are round and reactive to light and accommodation and his mucous membranes are moist. His heart has a regular rhythm without murmurs, his lungs are clear to auscultation bilaterally, the abdomen is soft, and his extremities have no edema but his muscular strength is 3/5 bilaterally. There is hyporeflexia of all four extremities. What is the most likely cause of his symptoms?
A 71-year-old African American man is brought to the emergency department with sudden onset lower limb paralysis and back pain. He has had generalized bone pain for 2 months. He has no history of severe illnesses. He takes ibuprofen for pain. On examination, he is pale. The vital signs include: temperature 37.1°C (98.8°F), pulse 68/min, respiratory rate 16/min, and blood pressure 155/90 mm Hg. The neurologic examination shows paraparesis. The 8th thoracic vertebra is tender to palpation. X-ray of the thoracic vertebrae confirms a compression fracture at the same level. The laboratory studies show the following: Laboratory test Hemoglobin 9 g/dL Mean corpuscular volume 95 μm3 Leukocyte count 5,000/mm3 Platelet count 240,000/mm3 ESR 85 mm/hr Serum Na+ 135 mEq/L K+ 4.2 mEq/L Cl− 113 mEq/L HCO3− 20 mEq/L Ca+ 11.8 mg/dL Albumin 4 g/dL Urea nitrogen 38 mg/dL Creatinine 2.2 mg/dL Which of the following is the most likely mechanism underlying this patient’s vertebral fracture?
A 48-year-old man with a 30-pack-year history comes to the physician for a follow-up examination 6 months after a chest CT showed a solitary 5-mm solid nodule in the upper lobe of the right lung. The follow-up CT shows that the size of the nodule has increased to 2 cm. Ipsilateral mediastinal lymph node involvement is noted. A biopsy of the pulmonary nodule shows small, dark blue tumor cells with hyperchromatic nuclei and scarce cytoplasm. Cranial MRI and skeletal scintigraphy show no evidence of other metastases. Which of the following is the most appropriate next step in management?
A 69-year-old woman presents with pain in her hip and groin. She states that the pain is present in the morning, and by the end of the day it is nearly unbearable. Her past medical history is notable for a treated episode of acute renal failure, diabetes mellitus, obesity, and hypertension. Her current medications include losartan, metformin, insulin, and ibuprofen. The patient recently started taking high doses of vitamin D as she believes that it could help her symptoms. She also states that she recently fell off the treadmill while exercising at the gym. On physical exam you note an obese woman. There is pain, decreased range of motion, and crepitus on physical exam of her right hip. The patient points to the areas that cause her pain stating that it is mostly over the groin. The patient's skin turgor reveals tenting. Radiography is ordered. Which of the following is most likely to be found on radiography?
A 62-year-old woman presents to the emergency department with a 2-hour history of sharp chest pain. She says that the pain is worse when she inhales and is relieved by sitting up and leaning forward. Her past medical history is significant for rheumatoid arthritis, myocardial infarction status post coronary artery bypass graft, and radiation for breast cancer 20 years ago. Physical exam reveals a rubbing sound upon cardiac auscultation as well as increased jugular venous distention on inspiration. Pericardiocentesis is performed revealing grossly bloody fluid. Which of the following is most specifically associated with this patient's presentation?
A previously healthy 44-year-old man is brought by his coworkers to the emergency department 45 minutes after he became light-headed and collapsed while working in the boiler room of a factory. He did not lose consciousness. His coworkers report that 30 minutes prior to collapsing, he told them he was nauseous and had a headache. The patient appears sweaty and lethargic. He is not oriented to time, place, or person. The patient’s vital signs are as follows: temperature 41°C (105.8°F); heart rate 133/min; respiratory rate 22/min; and blood pressure 90/52 mm Hg. Examination shows equal and reactive pupils. Deep tendon reflexes are 2+ bilaterally. His neck is supple. A 0.9% saline infusion is administered. A urinary catheter is inserted and dark brown urine is collected. The patient’s laboratory test results are as follows: Laboratory test Blood Hemoglobin 15 g/dL Leukocyte count 18,000/mm3 Platelet count 51,000/mm3 Serum Na+ 149 mEq/L K+ 5.0 mEq/L Cl- 98 mEq/L Urea nitrogen 42 mg/dL Glucose 88 mg/dL Creatinine 1.8 mg/dL Aspartate aminotransferase (AST, GOT) 210 Alanine aminotransferase (ALT, GPT) 250 Creatine kinase 86,000 U/mL Which of the following is the most appropriate next step in patient management?
Practice by Chapter
Hypertension diagnosis and management
Practice Questions
Stable coronary artery disease
Practice Questions
Peripheral arterial disease
Practice Questions
Aortic diseases
Practice Questions
Valvular heart disease
Practice Questions
Pericardial diseases
Practice Questions
Adult congenital heart disease
Practice Questions
Cardiac tumors
Practice Questions
Cardiac manifestations of systemic diseases
Practice Questions
Pre-operative cardiac risk assessment
Practice Questions
Cardiac imaging modalities
Practice Questions
Preventive cardiology
Practice Questions
Cardiac rehabilitation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app