
Psychopharmacology — MCQs

On this page
A 28-year-old woman diagnosed with schizophrenia had been compliant with her prescribed olanzapine for several months. However, she discontinued the treatment. Which of the following is the most likely reason for her discontinuation?
A 38-year-old professor with depression requests you to prescribe an antidepressant that would be least likely to cause sexual dysfunction. Which of the following drugs would you prescribe?
Which among the following psychoactive substances has antidepressant properties?
Which of the following drugs are used in the management of acute mania?
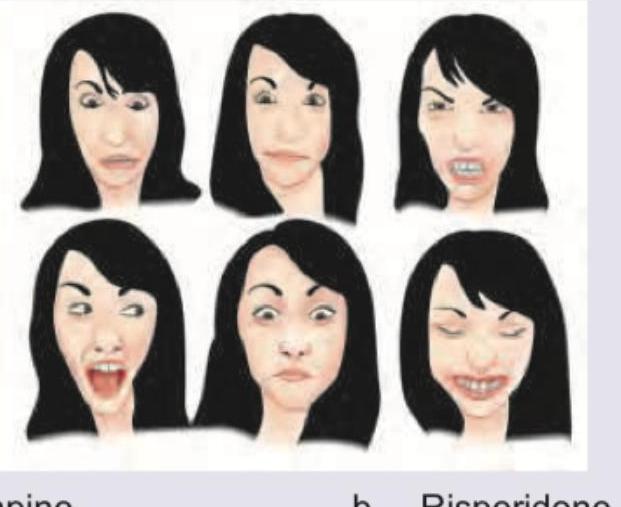
A patient on haloperidol for 2 years presents with orofacial dyskinesia and extrapyramidal symptoms. What is the appropriate treatment?
A patient on long-term antipsychotics develops involuntary mouth and lip movements (perioral dyskinesia). What is the best treatment?
Which of the following psychoactive substances is a new, rapidly acting antidepressant?
Which drug has propensity to cause such involuntary movements?
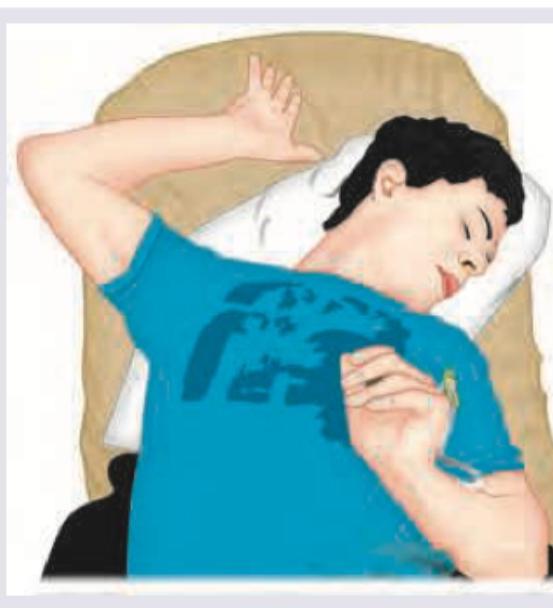
A 25-year-old uncooperative patient of schizophrenia was brought in to the casualty. The Casualty Medical Officer gave an injectable drug to the patient. Two hours later patient develops the following posturing. What is the best treatment?
Which of the following medications may be used in a child diagnosed with Attention Deficit Hyperactivity Disorder? I. Carbamazepine II. Methylphenidate III. Atomoxetine IV. Clonazepam Select the correct answer using the code given below :
Practice by Chapter
Principles of Psychopharmacology
Practice Questions
Antipsychotic Medications
Practice Questions
Antidepressant Medications
Practice Questions
Mood Stabilizers
Practice Questions
Anxiolytics and Hypnotics
Practice Questions
Stimulants and Cognitive Enhancers
Practice Questions
Pharmacokinetics and Pharmacodynamics
Practice Questions
Drug Interactions
Practice Questions
Adverse Effects and Management
Practice Questions
Pharmacogenomics in Psychiatry
Practice Questions
Special Populations Considerations
Practice Questions
Treatment Algorithms and Guidelines
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app