Internal Medicine
1 questionsA 50 year old male presents with fever and malaise for 4 months and pain in the knees and ankles. Blood tests are normal apart from a raised ESR. Chest x-ray shows bilateral hilar adenopathy and pulmonary infiltrates most severe in the upper and mid zones. Mantoux test is negative. What is the most likely diagnosis?
Pharmacology
1 questionsWhich of the following is the only clinically available depolarizing muscle relaxant?
Psychiatry
3 questionsA 25-year-old male believes that his penis is decreasing in size every day and that it will eventually disappear, leading to his death. What is the most likely diagnosis?
What is the primary cause of death in Neuroleptic Malignant Syndrome?
The site of lesion in Korsakoff's psychosis is
Radiology
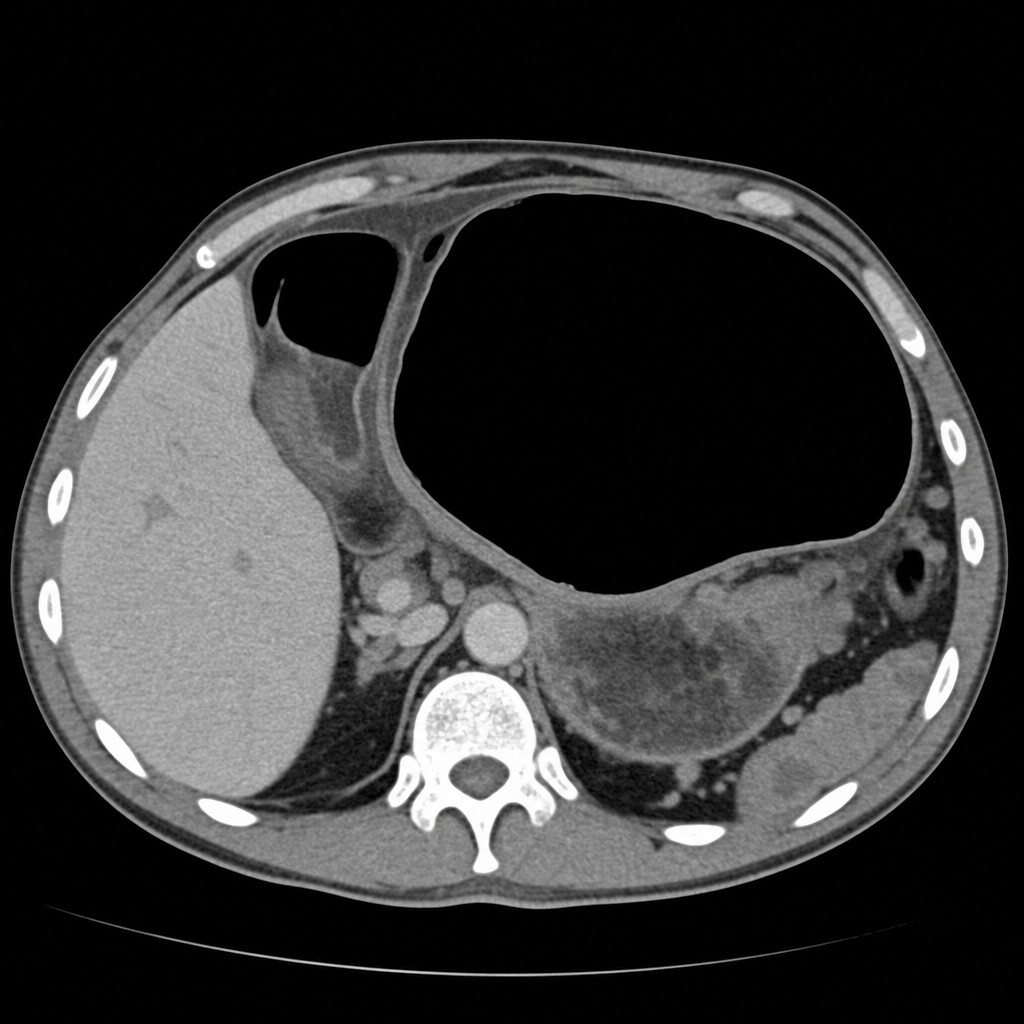
4 questionsOn CT scan, gastric volvulus typically shows which of the following findings?
Cobra head appearance on excretory urography is suggestive of?
Which of the following is NOT a typical ultrasonographic finding in autosomal recessive polycystic kidney disease (ARPKD)?
Which of the following statements about lipoma is radiologically true?
Surgery
1 questionsA patient presents with abdominal pain. On physical examination there was abdominal guarding and tenderness. A plain erect chest X-ray reveals air under diaphragm. Probable diagnosis is
