
Pulmonology — MCQs

On this page
A 24-year-old woman presents with increasing shortness of breath following treatment for right lower lobe pneumonia. She denies fever, cough, or sputum production. Examination reveals decreased tactile fremitus, dullness to percussion, and absent breath sounds over the right lower lung. Additionally, the trachea is deviated to the left. What is the most likely diagnosis for this patient's abnormal pulmonary physical findings?
100% oxygen is not effective in which of the following conditions?
Diagnostic criteria for ARDS include all except?
What is the invasive modality for diagnosing pulmonary embolism?
What is the probable diagnosis in the patient with the provided flow volume loop (FVL)?
Pulmonology Indian Medical PG Practice Questions and MCQs
Question 1: A 24-year-old woman presents with increasing shortness of breath following treatment for right lower lobe pneumonia. She denies fever, cough, or sputum production. Examination reveals decreased tactile fremitus, dullness to percussion, and absent breath sounds over the right lower lung. Additionally, the trachea is deviated to the left. What is the most likely diagnosis for this patient's abnormal pulmonary physical findings?
- A. Acute asthmatic attack
- B. Complete pneumothorax
- C. Large pleural effusion (Correct Answer)
- D. Atelectasis
Explanation: ### Explanation The patient presents with classic signs of a **large pleural effusion**, likely a parapneumonic effusion following her recent pneumonia [1]. **1. Why "Large Pleural Effusion" is correct:** The diagnosis is based on the triad of physical findings: * **Dullness to percussion:** Fluid in the pleural space replaces air-filled lung tissue [1]. * **Decreased tactile fremitus and absent breath sounds:** Fluid acts as an insulator, preventing the transmission of vocal vibrations and breath sounds from the lung to the chest wall [1]. * **Tracheal deviation to the opposite side:** A large volume of fluid creates a "mass effect," increasing intrapleural pressure and pushing the mediastinal structures (including the trachea) **away** from the affected side [1]. **2. Why other options are incorrect:** * **A. Acute asthmatic attack:** Characterized by hyper-resonance on percussion and diffuse wheezing, not localized dullness or tracheal deviation. * **B. Complete pneumothorax:** While it causes absent breath sounds and can deviate the trachea to the opposite side (if under tension), it presents with **hyper-resonance** (due to air), not dullness. * **C. Atelectasis:** This involves lung collapse. While it causes dullness and decreased breath sounds, it creates negative pressure that pulls the trachea **toward** the side of the lesion. ### NEET-PG High-Yield Pearls * **Tracheal Deviation Rule:** * **Pushes AWAY:** Large Pleural Effusion, Tension Pneumothorax. * **Pulls TOWARD:** Atelectasis (Collapse), Lung Fibrosis, Agenesis. * **Percussion Note:** Dullness = Fluid/Solid (Effusion, Consolidation); Hyper-resonance = Air (Pneumothorax, Emphysema). * **Tactile Fremitus:** Increased only in **Consolidation** (with a patent bronchus); decreased in almost all other pathologies (Effusion, Pneumothorax, Collapse).
Question 2: 100% oxygen is not effective in which of the following conditions?
- A. Pulmonary edema
- B. Myocardial infarction
- C. Tetralogy of Fallot (Correct Answer)
- D. COPD
Explanation: ### Explanation The correct answer is **Tetralogy of Fallot (TOF)**. #### 1. Why Tetralogy of Fallot is the Correct Answer The underlying mechanism is a **Right-to-Left (R-L) Shunt**. In TOF, deoxygenated blood from the right ventricle bypasses the lungs entirely and enters the systemic circulation through a large Ventricular Septal Defect (VSD) and an overriding aorta [3]. Since this shunted blood never comes into contact with the alveoli, increasing the Fraction of Inspired Oxygen ($FiO_2$) to 100% cannot oxygenate it [1]. This is known as a **refractory hypoxemia**. While 100% oxygen may slightly increase the dissolved oxygen in the blood that *does* pass through the lungs, it cannot correct the significant desaturations caused by the anatomical shunt [2]. #### 2. Why Other Options are Incorrect * **Pulmonary Edema:** This causes a **diffusion defect** and **V/Q mismatch**. Increasing the $FiO_2$ increases the pressure gradient for oxygen to cross the fluid-filled alveolar-capillary membrane, effectively improving $PaO_2$. * **Myocardial Infarction:** Oxygen is standard therapy (if $SaO_2 < 90\%$) to maximize oxygen delivery to the ischemic myocardium. There is no anatomical shunt preventing oxygenation. * **COPD:** Hypoxemia in COPD is primarily due to **V/Q mismatch**. While high-flow oxygen must be used cautiously (due to the risk of hypercapnia/loss of hypoxic drive), it is highly effective at raising $PaO_2$ [2]. #### 3. NEET-PG High-Yield Pearls * **The Hyperoxic Test:** This is used to differentiate cardiac from pulmonary causes of cyanosis in neonates. If $PaO_2$ fails to rise above **100 mmHg** after giving 100% oxygen for 10–15 minutes, a cyanotic congenital heart disease (R-L shunt) is highly likely. * **Refractory Hypoxemia:** Always think of **Shunts** (Anatomic like TOF, or Physiologic like ARDS) when hypoxemia does not respond to oxygen therapy [1]. * **V/Q Mismatch vs. Shunt:** V/Q mismatch responds well to low doses of supplemental oxygen; Shunts do not [1].
Question 3: Diagnostic criteria for ARDS include all except?
- A. Bilateral alveolar infiltrates
- B. PaO2 / FiO2 < 300 mm Hg (Correct Answer)
- C. Acute onset
- D. Pulmonary capillary wedge pressure <= 18 mm Hg
Explanation: This question focuses on the **Berlin Definition (2012)**, which is the current gold standard for diagnosing Acute Respiratory Distress Syndrome (ARDS) [1]. ### **Why Option B is the Correct Answer (The Exception)** The question asks for the "except" regarding diagnostic criteria. While a $PaO_2/FiO_2$ ratio of $< 300$ mmHg is indeed part of the Berlin criteria, it defines **Mild ARDS** [1]. However, in the context of many standardized exams (including NEET-PG), this question often refers to the older **AECC (American-European Consensus Conference) definition**. Under the older AECC criteria, ARDS was specifically defined by a $PaO_2/FiO_2 \leq 200$ mmHg, while a ratio between 201–300 mmHg was termed "Acute Lung Injury" (ALI). Therefore, in a comparative MCQ setting, $< 300$ is considered the "least correct" or the differentiator between ALI and ARDS. ### **Analysis of Other Options** * **A. Bilateral alveolar infiltrates:** Required by both AECC and Berlin criteria [1]. These must be present on frontal chest radiograph or CT and not fully explained by effusions or collapse. * **C. Acute onset:** Symptoms must develop within **one week** of a known clinical insult or new/worsening respiratory symptoms [1]. * **D. PCWP $\leq$ 18 mmHg:** This was a hallmark of the AECC definition to exclude hydrostatic (cardiogenic) pulmonary edema. While the Berlin criteria replaced this with "respiratory failure not fully explained by heart failure or fluid overload," a PCWP $\leq$ 18 remains a classic diagnostic threshold in exams [1]. ### **High-Yield Clinical Pearls for NEET-PG** * **Berlin Severity Grading:** * **Mild:** $PaO_2/FiO_2$ 201–300 mmHg (with PEEP/CPAP $\geq$ 5 $cmH_2O$) * **Moderate:** $PaO_2/FiO_2$ 101–200 mmHg * **Severe:** $PaO_2/FiO_2 \leq 100$ mmHg * **Management:** The mainstay is **Low Tidal Volume Ventilation (6 mL/kg)** to prevent volutrauma and **Prone Positioning** (if $PaO_2/FiO_2 < 150$). * **Pathology:** The characteristic histological finding is **Diffuse Alveolar Damage (DAD)** with hyaline membrane formation.
Question 4: What is the invasive modality for diagnosing pulmonary embolism?
- A. Venous ultrasonography
- B. Pulmonary angiography (Correct Answer)
- C. CT scan
- D. MRI scan
Explanation: **Explanation:** **Pulmonary angiography** is traditionally considered the **gold standard** and the definitive invasive modality for diagnosing pulmonary embolism (PE). It involves the percutaneous insertion of a catheter (usually via the femoral vein) into the pulmonary artery, followed by the injection of radiopaque contrast. A positive diagnosis is confirmed by the direct visualization of an intraluminal filling defect or the abrupt "cutoff" of a pulmonary vessel. While highly accurate, its use has declined due to its invasive nature and the high diagnostic yield of modern non-invasive imaging. **Analysis of Incorrect Options:** * **A. Venous Ultrasonography:** This is a non-invasive bedside tool used to detect Deep Vein Thrombosis (DVT). While a positive DVT scan in a symptomatic patient is highly suggestive of PE, it does not directly visualize the pulmonary vasculature [1]. * **C. CT Scan (CTPA):** Computed Tomographic Pulmonary Angiography is currently the **investigation of choice** and the clinical standard for diagnosing PE due to its high sensitivity and non-invasive nature [1]. However, it is not classified as an "invasive" modality. * **D. MRI Scan:** Magnetic Resonance Angiography (MRA) is a non-invasive alternative, typically reserved for patients with contraindications to CT contrast or radiation (e.g., pregnancy or renal failure), but it is less sensitive than CTPA. **High-Yield Clinical Pearls for NEET-PG:** * **Investigation of Choice:** CT Pulmonary Angiography (CTPA) [1]. * **Gold Standard (Invasive):** Conventional Pulmonary Angiography. * **Best Initial Test:** Chest X-ray (to rule out other causes), though often normal or showing non-specific signs like **Westermark sign** (oligemia) or **Hampton’s hump** (wedge-shaped opacity). * **ECG Finding:** Most common is sinus tachycardia; most specific is the **S1Q3T3 pattern**. * **Gold Standard for DVT:** Contrast Venography.
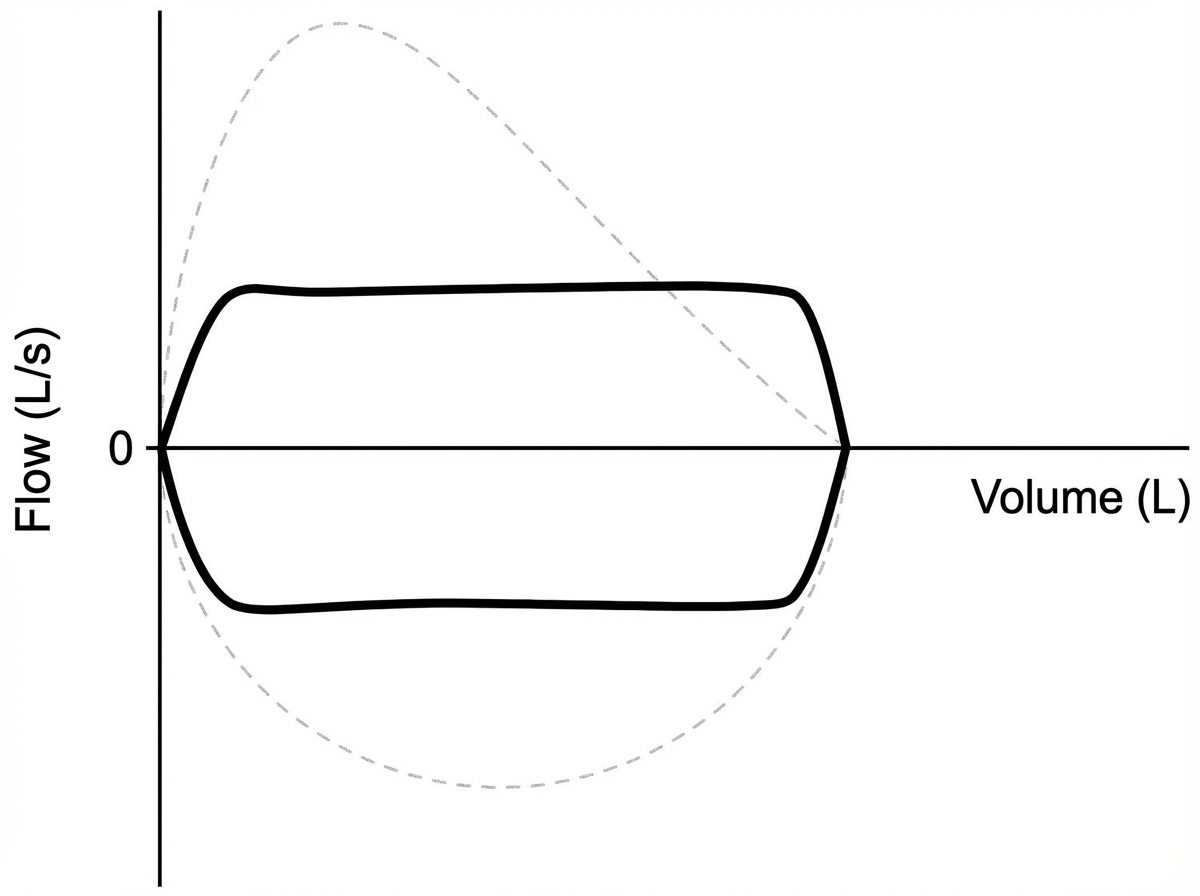
Question 5: What is the probable diagnosis in the patient with the provided flow volume loop (FVL)?
- A. Restrictive airway disease
- B. Tracheal stenosis (Correct Answer)
- C. Obstructive airway disease
- D. None of the above
Explanation: ***Tracheal stenosis*** - The flow-volume loop shows a **plateau/flattening pattern** on both inspiratory and expiratory limbs, characteristic of **fixed upper airway obstruction** like tracheal stenosis. - This creates a **box-shaped** or **truncated** flow-volume loop due to the **fixed anatomical narrowing** limiting maximum airflow regardless of respiratory effort. *Restrictive airway disease* - Flow-volume loop would show a **normal shape but reduced volumes** (FVC, TLC) with preserved flow rates relative to lung volumes. - The **flow-volume curve maintains its normal contour** but appears **smaller and shifted downward**, not flattened or plateau-shaped. *Obstructive airway disease* - Characterized by a **scooped-out or concave** expiratory limb on the flow-volume loop due to **dynamic airway collapse**. - Shows **reduced peak expiratory flow** and **prolonged expiratory phase** with normal or increased lung volumes, contrasting with the plateau pattern. *None of the above* - The flow-volume loop clearly demonstrates pathological findings consistent with **upper airway obstruction**. - The characteristic **flattened plateau pattern** is pathognomonic for **fixed obstruction** like tracheal stenosis, making this option incorrect.
Practice by Chapter
Obstructive Airway Diseases (Asthma, COPD)
Practice Questions
Interstitial Lung Diseases
Practice Questions
Pulmonary Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Pleural Diseases
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Respiratory Failure
Practice Questions
Mediastinal Disorders
Practice Questions
Occupational Lung Diseases
Practice Questions
Pulmonary Function Testing
Practice Questions
Bronchiectasis and Cystic Fibrosis
Practice Questions
Lung Cancer Approach
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Start For Free