All SubjectsAnatomy (167)Anesthesiology (9)Biochemistry (108)Community Medicine (87)Dental (8)Dermatology (19)ENT (30)Forensic Medicine (62)General Medicine (3)Internal Medicine (136)Microbiology (101)Obstetrics and Gynecology (65)Ophthalmology (60)Orthopaedics (33)Pathology (107)Pediatrics (37)Pharmacology (123)Physiology (116)Psychiatry (2)Psychiatry (38)Radiology (25)Surgery (81)
Q11
Which subtype of Acute Myeloid Leukemia (AML) is associated with the best prognosis?
Q12
In which non-neoplastic condition is CEA commonly elevated?
Q13
Which of the following is not a feature of Poststreptococcal Glomerulonephritis (PSGN)?
Q14
In which condition is Tau protein primarily implicated?
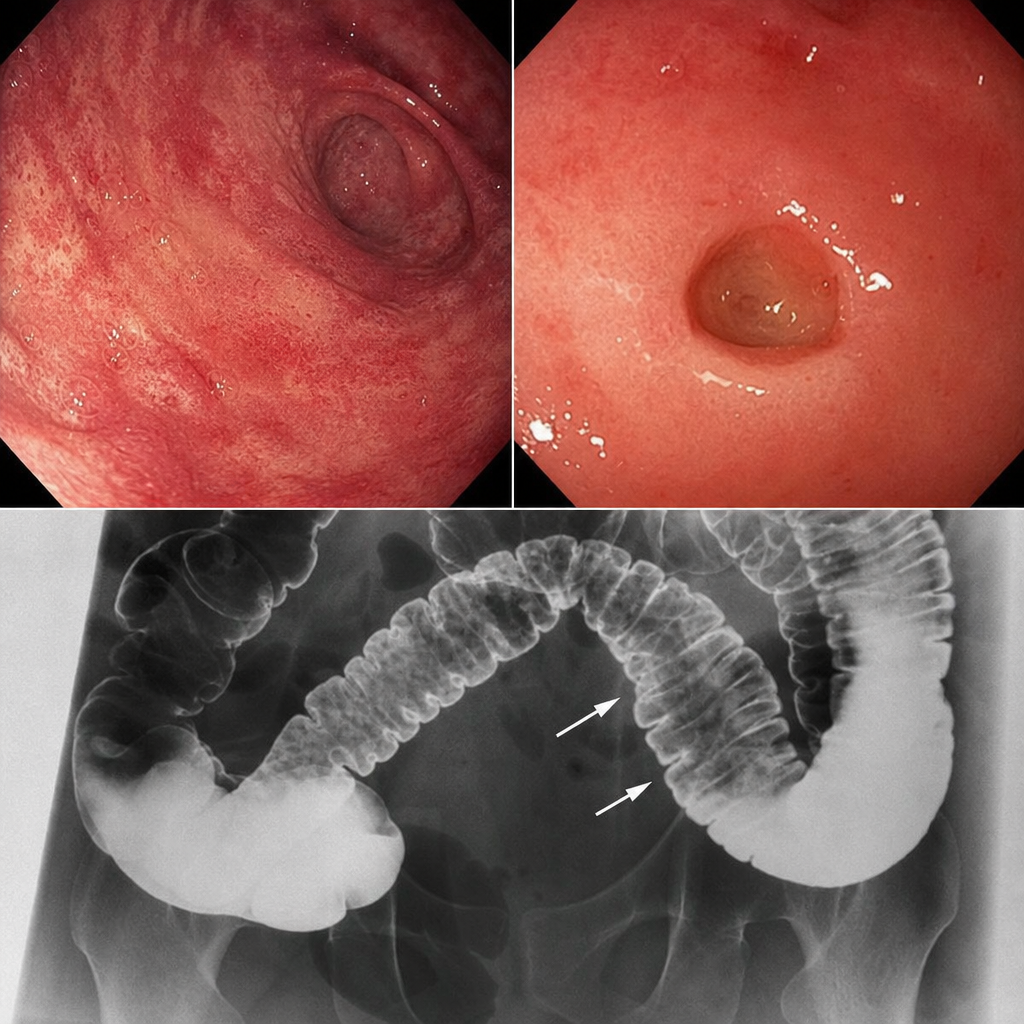
Q15
A patient presents with skin involvement and collar stud ulceration in the intestine observed on radiography. What is the most likely diagnosis?
Q16
Which of the following is true regarding carcinoid tumor?
Q17
Which type of thyroid cancer is associated with primary hyperparathyroidism and phaeochromocytoma?
Q18
What is the primary effect of beta blockers in the management of thyroid storm?
Q19
Which of the following is a cause of post-transplantation hypertension? I. Rejection II. Cyclosporine nephrotoxicity III. Renal transplant artery stenosis (RTAS) IV. Recurrent disease in the allograft. Select the correct option.
Q20
Shrinking Lung Syndrome is seen in: