A 62-year-old man is brought to the emergency department with a 2-day history of cough productive of yellowish sputum. He has had fever, chills, and worsening shortness of breath over this time. He has a 10-year history of hypertension and hyperlipidemia. He does not drink alcohol or smoke cigarettes. His current medications include atorvastatin, amlodipine, and metoprolol. His temperature is 38.9°C (102.0°F), pulse is 105/min, respirations are 27/min, and blood pressure is 110/70 mm Hg. He appears in mild distress. He has rales over the left lower lung field. The remainder of the examination shows no abnormalities. Leukocyte count is 15,000/mm3 (87% segmented neutrophils). Arterial blood gas analysis on room air shows:
pH 7.44
pO2 68 mm Hg
pCO2 28 mm Hg
HCO3- 24 mEq/L
O2 saturation 91%
An x-ray of the chest shows a consolidation in the left lower lobe. Asking the patient to lie down in the left lateral decubitus position would most likely result in which of the following?
Q2
A 52-year-old woman presents to the emergency department with breathlessness for the past 6 hours. She denies cough, nasal congestion or discharge, sneezing, blood in sputum, or palpitation. There is no past history of chronic respiratory or cardiovascular medical conditions, but she mentions that she has been experiencing frequent cramps in her left leg for the past 5 days. She is post-menopausal and has been on hormone replacement therapy for a year now. Her temperature is 38.3°C (100.9°F), the pulse is 116/min, the blood pressure is 136/84 mm Hg, and the respiratory rate is 24/min. Edema and tenderness are present in her left calf region. Auscultation of the chest reveals rales over the left infrascapular and scapular region. The heart sounds are normal and there are no murmurs. Which of the following mechanisms most likely contributed to the pathophysiology of this patient’s condition?
Q3
A 22-year-old man volunteers for a research study on lung function. He has no history of lung disease or allergies and does not smoke. His pulmonary blood flow is measured in the various labeled segments of the lungs while standing. Then the volunteer, still standing, is given very low continuous positive airway pressure and the blood flow measured again. Which of the following sets of findings are most likely to be present in the second measurements relative to the first?
Q4
A 19-year-old man comes to the emergency department with sharp, left-sided chest pain and shortness of breath. He has no history of recent trauma. He does not smoke or use illicit drugs. He is 196 cm (6 feet 5 in) tall and weighs 70 kg (154 lb); BMI is 18 kg/m2. Examination shows reduced breath sounds over the left lung field. An x-ray of the chest is shown. Which of the following changes is most likely to immediately result from this patient's current condition?
Q5
A 17-year-old boy is brought to the physician by his father because of fever, congestion, and malaise for the past 2 days. He reports a sensation of pressure over his nose and cheeks. Over the past year, he has had an intermittent cough productive of green sputum and lately has noticed some streaks of blood in the sputum. He has had over 10 episodes of sinusitis, all of which were successfully treated with antibiotics. There is no family history of serious illness. The patient's vaccinations are up-to-date. His temperature is 38°C (100.4°F), pulse is 90/min, and blood pressure is 120/80 mm Hg. Physical examination shows tenderness to palpation over both cheeks. Crackles and rhonchi are heard on auscultation of the chest. Cardiac examination shows an absence of heart sounds along the left lower chest. Which of the following additional findings is most likely in this patient?
V/Q mismatch US Medical PG Practice Questions and MCQs
Question 1: A 62-year-old man is brought to the emergency department with a 2-day history of cough productive of yellowish sputum. He has had fever, chills, and worsening shortness of breath over this time. He has a 10-year history of hypertension and hyperlipidemia. He does not drink alcohol or smoke cigarettes. His current medications include atorvastatin, amlodipine, and metoprolol. His temperature is 38.9°C (102.0°F), pulse is 105/min, respirations are 27/min, and blood pressure is 110/70 mm Hg. He appears in mild distress. He has rales over the left lower lung field. The remainder of the examination shows no abnormalities. Leukocyte count is 15,000/mm3 (87% segmented neutrophils). Arterial blood gas analysis on room air shows:
pH 7.44
pO2 68 mm Hg
pCO2 28 mm Hg
HCO3- 24 mEq/L
O2 saturation 91%
An x-ray of the chest shows a consolidation in the left lower lobe. Asking the patient to lie down in the left lateral decubitus position would most likely result in which of the following?
A. Decreased ventilation of the left lung
B. Worsen the hypocapnia
C. Increase in A-a gradient (Correct Answer)
D. Increased perfusion of right lung
E. Improve the hypoxemia
Explanation: ***Increase in A-a gradient***
- Placing the patient in the **left lateral decubitus position** would worsen V/Q mismatch because the **diseased left lung** (with consolidation) would receive increased perfusion due to gravity.
- This increased perfusion to a poorly ventilated area would further impair gas exchange, leading to a larger **alveolar-arterial (A-a) gradient**.
*Decreased ventilation of the left lung*
- While lying on the left side might slightly restrict the expansion of the left lung, the primary issue is the **consolidation** itself, which already severely impairs ventilation.
- The main problem with positioning is not a further decrease in ventilation but rather the **redistribution of blood flow** to an already compromised lung.
*Worsen the hypocapnia*
- The patient has **hypocapnia (pCO2 28 mm Hg)** due to tachypnea as compensation for hypoxemia, indicating increased minute ventilation.
- While worsening the V/Q mismatch will worsen hypoxemia, it's unlikely to directly worsen hypocapnia further; the body would still try to compensate through increased respiratory drive unless the respiratory muscles become fatigued.
*Increased perfusion of right lung*
- In the left lateral decubitus position, **perfusion due to gravity** would increase in the dependent (left) lung, not the non-dependent (right) lung.
- The right lung would experience relatively decreased perfusion compared to the left lung in this position.
*Improve the hypoxemia*
- Lying on the side of the **diseased lung** (left) typically **worsens hypoxemia** because gravity directs more blood flow to the poorly ventilated, consolidated lung.
- To improve hypoxemia, the patient should be positioned with the **healthy lung dependent** (e.g., right lateral decubitus or semi-Fowler's with the right lung lower) to optimize V/Q matching.
Question 2: A 52-year-old woman presents to the emergency department with breathlessness for the past 6 hours. She denies cough, nasal congestion or discharge, sneezing, blood in sputum, or palpitation. There is no past history of chronic respiratory or cardiovascular medical conditions, but she mentions that she has been experiencing frequent cramps in her left leg for the past 5 days. She is post-menopausal and has been on hormone replacement therapy for a year now. Her temperature is 38.3°C (100.9°F), the pulse is 116/min, the blood pressure is 136/84 mm Hg, and the respiratory rate is 24/min. Edema and tenderness are present in her left calf region. Auscultation of the chest reveals rales over the left infrascapular and scapular region. The heart sounds are normal and there are no murmurs. Which of the following mechanisms most likely contributed to the pathophysiology of this patient’s condition?
A. Secretion of vasodilating neurohumoral substances in pulmonary vascular bed
B. Increased right ventricular preload (Correct Answer)
C. Decreased physiologic dead space
D. Alveolar hyperventilation
E. Decreased alveolar-arterial oxygen tension gradient
Explanation: ***Increased right ventricular preload***
- The patient's presentation (acute breathlessness, unilateral leg cramps, calf tenderness and edema, rales) combined with risk factors (post-menopausal, hormone replacement therapy) strongly suggests **pulmonary embolism (PE)** from deep vein thrombosis (DVT).
- In PE, thrombus occludes pulmonary vasculature causing **increased pulmonary vascular resistance**, which increases **right ventricular afterload** (the resistance the RV must overcome to eject blood).
- **Note:** While this option states "preload," the primary mechanism is actually increased RV **afterload**. However, this is the most appropriate answer among the given options, as the increased resistance does lead to RV strain and potential backup of blood that can secondarily affect preload.
*Secretion of vasodilating neurohumoral substances in pulmonary vascular bed*
- The primary vascular response in PE is **vasoconstriction**, not vasodilation.
- Hypoxia and mediator release cause **pulmonary vasoconstriction** distal to the embolus, further increasing pulmonary vascular resistance.
*Decreased physiologic dead space*
- In PE, there is **ventilation-perfusion (V/Q) mismatch** where lung regions are ventilated but not perfused due to embolic obstruction.
- This actually **increases physiologic dead space** because these areas are ventilated but cannot participate in gas exchange.
*Alveolar hyperventilation*
- Patients with PE often develop **tachypnea and hyperventilation** due to hypoxia, anxiety, and chest discomfort.
- However, this is a **compensatory response** to hypoxemia, not the primary pathophysiological mechanism causing the condition.
*Decreased alveolar-arterial oxygen tension gradient*
- The **A-a gradient is increased in PE** due to V/Q mismatch and shunting, reflecting impaired gas exchange.
- A decreased A-a gradient would indicate efficient gas exchange, which contradicts the hypoxia and breathlessness seen in PE.
Question 3: A 22-year-old man volunteers for a research study on lung function. He has no history of lung disease or allergies and does not smoke. His pulmonary blood flow is measured in the various labeled segments of the lungs while standing. Then the volunteer, still standing, is given very low continuous positive airway pressure and the blood flow measured again. Which of the following sets of findings are most likely to be present in the second measurements relative to the first?
A. Increased blood flow in zone 2
B. Reduced blood flow in zone 3
C. Reduced blood flow in zone 1
D. Increased blood flow in zone 3
E. Increased blood flow in zone 1 (Correct Answer)
Explanation: ***Increased blood flow in zone 1***
- In healthy standing subjects, **Zone 1** may not exist or is minimal at the apex where alveolar pressure (PA) can exceed arterial pressure (Pa).
- **Very low CPAP** increases alveolar pressure, but when applied at very low levels, it may **recruit collapsed or under-perfused alveoli** by preventing alveolar collapse and improving the pressure gradient.
- The net effect with **very low CPAP** can paradoxically **improve perfusion** in Zone 1 by optimizing alveolar mechanics and reducing vascular resistance through **alveolar recruitment**, particularly in previously under-ventilated apical regions.
*Increased blood flow in zone 2*
- In Zone 2, arterial pressure exceeds alveolar pressure, which exceeds venous pressure (**Pa > PA > Pv**), creating a waterfall effect.
- While CPAP increases alveolar pressure (PA), this would increase the downstream resistance and typically **reduce** the arterial-alveolar pressure gradient (Pa - PA), decreasing flow rather than increasing it.
*Increased blood flow in zone 3*
- **Zone 3** (lung base) normally has the **highest blood flow** where both arterial and venous pressures exceed alveolar pressure (**Pa > Pv > PA**).
- CPAP increases alveolar pressure (PA), which would compress capillaries and **reduce** the pressure gradient, typically decreasing rather than increasing blood flow in this zone.
*Reduced blood flow in zone 1*
- While increasing alveolar pressure with CPAP might be expected to **reduce** Zone 1 perfusion by compressing capillaries, **very low levels of CPAP** can have the opposite effect through **alveolar recruitment** and optimization of lung mechanics.
- The question specifies **very low** CPAP, which is the key—this level improves alveolar patency without significantly compressing capillaries.
*Reduced blood flow in zone 3*
- Zone 3 typically has the highest blood flow due to favorable pressure gradients from gravity.
- CPAP increases PA, which could compress capillaries and reduce the (Pa - PA) gradient, but the **very low level** specified means this effect is minimal and Zone 3 generally maintains adequate perfusion.
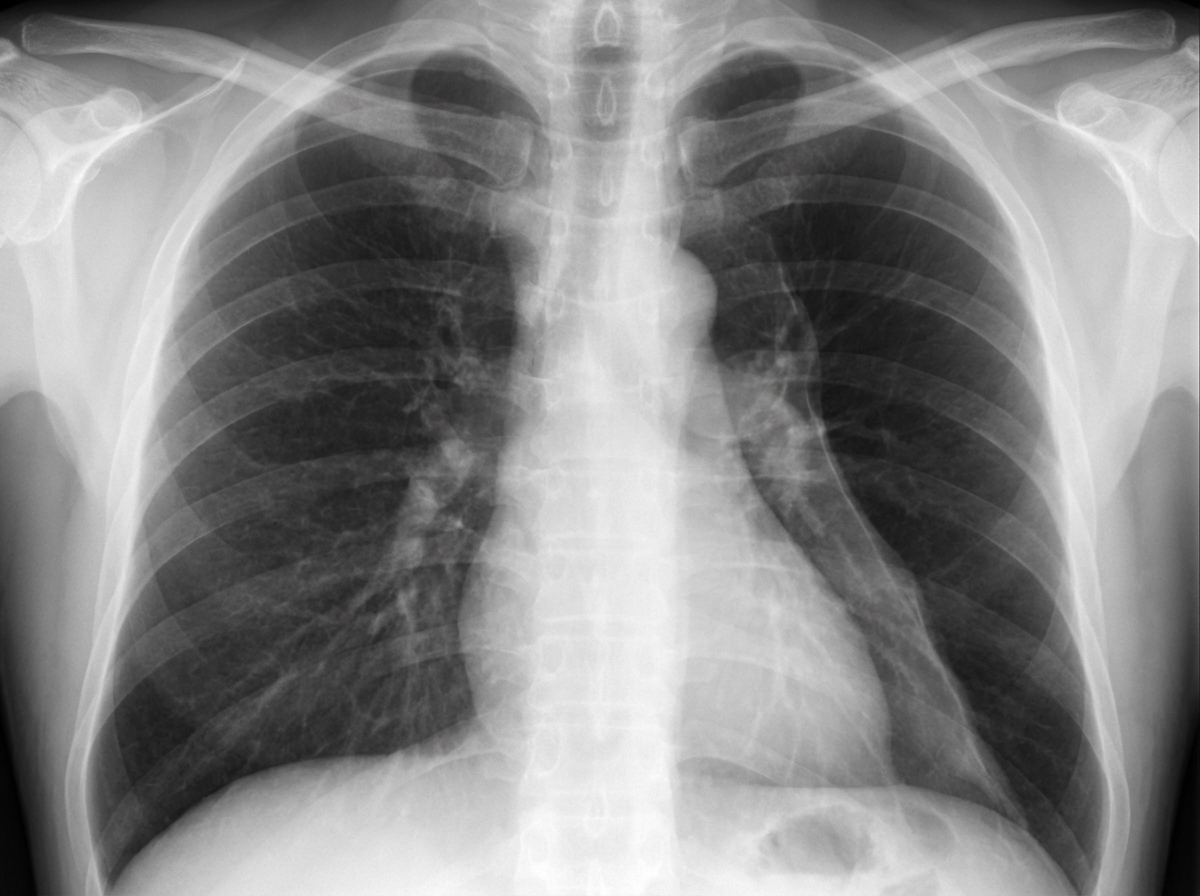
Question 4: A 19-year-old man comes to the emergency department with sharp, left-sided chest pain and shortness of breath. He has no history of recent trauma. He does not smoke or use illicit drugs. He is 196 cm (6 feet 5 in) tall and weighs 70 kg (154 lb); BMI is 18 kg/m2. Examination shows reduced breath sounds over the left lung field. An x-ray of the chest is shown. Which of the following changes is most likely to immediately result from this patient's current condition?
A. Increased intra-alveolar pressure
B. Increased right-to-left shunting (Correct Answer)
C. Increased lung compliance
D. Increased transpulmonary pressure
E. Increased physiological dead space
Explanation: ***Increased right-to-left shunting***
- The patient has a **spontaneous pneumothorax** (common in tall, thin young males) causing **left lung collapse**.
- In the collapsed lung, alveoli are **not ventilated but continue to be perfused** (at least initially, before hypoxic pulmonary vasoconstriction fully develops), creating **perfusion without ventilation**.
- This represents a **low V/Q ratio approaching zero (true shunt)**, where deoxygenated blood bypasses functional gas exchange units, resulting in **increased right-to-left shunting** and immediate hypoxemia.
- This is the **immediate pathophysiologic change** that causes the patient's shortness of breath and hypoxemia.
*Increased intra-alveolar pressure*
- In a **pneumothorax**, air enters the pleural space, increasing **pleural pressure** and causing lung collapse.
- The collapsed alveoli have **reduced or zero pressure**, not increased pressure.
- Intra-alveolar pressure would only increase in a **tension pneumothorax** with a one-way valve effect, which is not described here.
*Increased lung compliance*
- **Compliance** (ΔV/ΔP) measures how easily the lung expands.
- A **collapsed lung** has **decreased compliance** because it is harder to re-expand due to loss of surfactant function and alveolar collapse.
- The chest wall compliance may increase, but lung parenchymal compliance decreases.
*Increased transpulmonary pressure*
- **Transpulmonary pressure** = alveolar pressure - pleural pressure; this is the pressure that keeps the lung inflated.
- In pneumothorax, air in the pleural space **increases pleural pressure** (makes it less negative or even positive).
- This **reduces the transpulmonary pressure gradient**, causing lung collapse, not an increase.
*Increased physiological dead space*
- **Physiological dead space** occurs when alveoli are **ventilated but not perfused** (high V/Q ratio or wasted ventilation).
- In pneumothorax, the primary immediate problem is the **opposite**: the collapsed lung has **perfusion without ventilation** (shunt, low V/Q ratio).
- While the contralateral lung may develop some dead space from compensatory hyperventilation and redistribution, the **immediate dominant change** is shunt physiology from the collapsed lung, not dead space.
Question 5: A 17-year-old boy is brought to the physician by his father because of fever, congestion, and malaise for the past 2 days. He reports a sensation of pressure over his nose and cheeks. Over the past year, he has had an intermittent cough productive of green sputum and lately has noticed some streaks of blood in the sputum. He has had over 10 episodes of sinusitis, all of which were successfully treated with antibiotics. There is no family history of serious illness. The patient's vaccinations are up-to-date. His temperature is 38°C (100.4°F), pulse is 90/min, and blood pressure is 120/80 mm Hg. Physical examination shows tenderness to palpation over both cheeks. Crackles and rhonchi are heard on auscultation of the chest. Cardiac examination shows an absence of heart sounds along the left lower chest. Which of the following additional findings is most likely in this patient?
A. Immotile sperm (Correct Answer)
B. Absence of B lymphocytes
C. Increased forced expiratory volume
D. Increased sweat chloride levels
E. Defective interleukin-2 receptor gamma chain
Explanation: **Immotile sperm**
- This patient's history of **recurrent sinusitis**, **chronic productive cough**, and **situs inversus** (indicated by absence of heart sounds on the left lower chest) are classic signs of **primary ciliary dyskinesia (PCD)**, also known as Kartagener syndrome.
- In males with PCD, the **ciliary dysfunction** extends to the **sperm flagella**, leading to **immotile sperm** and subsequent **infertility**.
*Absence of B lymphocytes*
- An absence of **B lymphocytes** would suggest a **primary immunodeficiency** affecting humoral immunity, such as **X-linked agammaglobulinemia**.
- While patients would experience recurrent infections, the specific pattern of **situs inversus** and **chronic sino-pulmonary disease** points away from this diagnosis and towards a ciliary defect.
*Increased forced expiratory volume*
- **Increased forced expiratory volume (FEV)** is not typically associated with chronic respiratory conditions like those seen in PCD; in fact, chronic airway obstruction often leads to a **decreased FEV1** due to trapped air and inflammation.
- Patients with chronic lung disease, especially those with **bronchiectasis** as seen in PCD, usually have **obstructive lung disease** characterized by decreased airflow.
*Increased sweat chloride levels*
- **Increased sweat chloride levels** are the hallmark diagnostic finding for **cystic fibrosis (CF)**.
- While CF also presents with **chronic sinopulmonary infections** and **bronchiectasis**, it is typically associated with **pancreatic insufficiency** and **gastrointestinal symptoms** (e.g., malabsorption), which are not described in this patient.
*Defective interleukin-2 receptor gamma chain*
- A defective **interleukin-2 receptor gamma chain** is characteristic of **X-linked severe combined immunodeficiency (SCID)**.
- SCID causes profound immunodeficiency with severe, recurrent infections from infancy, but it does **not explain the situs inversus** or the specific pattern of chronic sinopulmonary disease seen here.