
Antimicrobials — MCQs

On this page
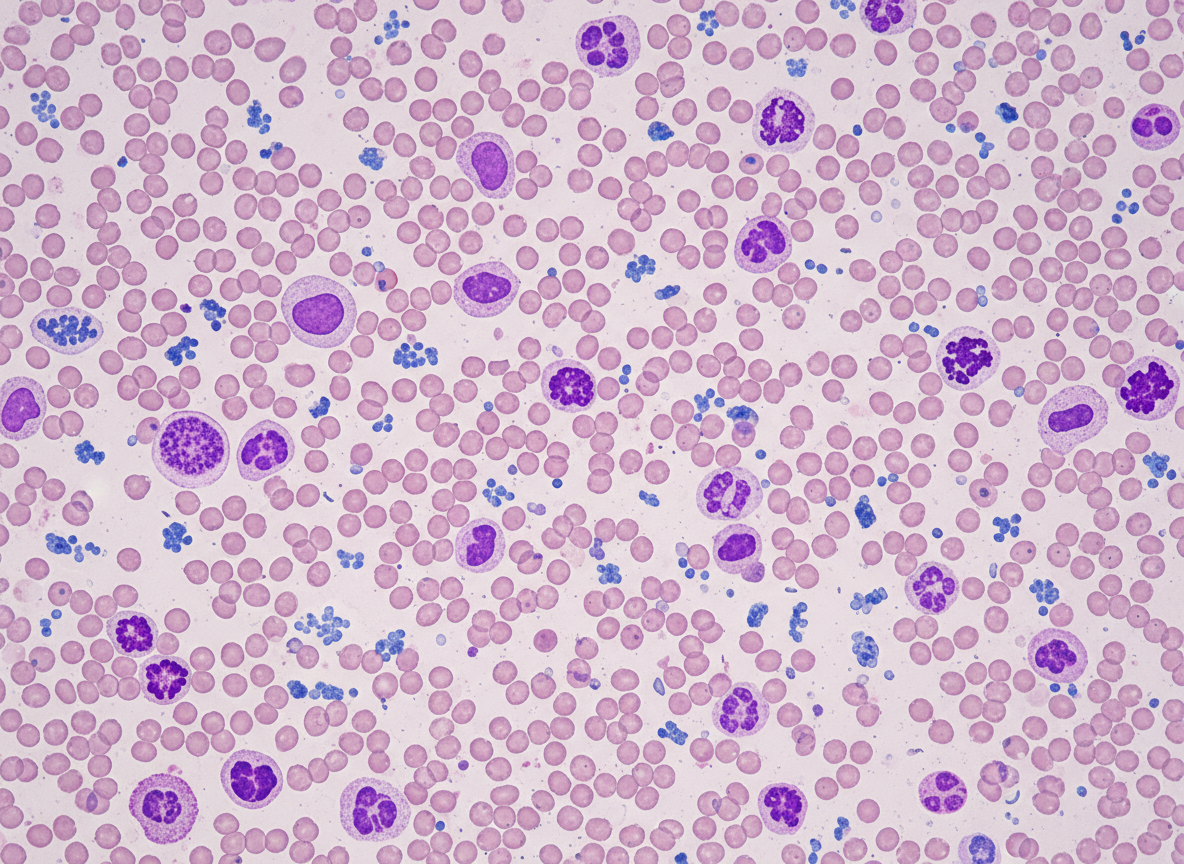
A 64-year-old woman comes to the physician for her routine health maintenance examination. She feels well. She had cervical cancer and received radiotherapy 8 years ago. Her vital signs are within normal limits. On percussion, the spleen size is 15 cm. Otherwise, the physical examination shows no abnormalities. The laboratory test results are as follows: Hemoglobin 10 g/dL Mean corpuscular volume 88 μm3 Leukocyte count 65,000/mm3 Platelet count 500,000/mm3 Two images of the peripheral blood smear are shown on the image. Which of the following is the most appropriate next step in management?
A 65-year-old female patient with a past medical history of diabetes mellitus and an allergy to penicillin develops an infected abscess positive for MRSA on the third day of her hospital stay. She is started on an IV infusion of vancomycin at a dose of 1000 mg every 12 hours. Vancomycin is eliminated by first-order kinetics and has a half life of 6 hours. The volume of distribution of vancomycin is 0.5 L/kg. Assuming no loading dose is given, how long will it take for the drug to reach 94% of its plasma steady state concentration?
A 55-year-old man presents to the urgent clinic complaining of pain in his right foot. He reported that the pain is intense that he had to remove his shoe and sock, and rates the pain level as 6 out of 10. He does not report trauma or recent infection. The past medical history includes hypertension. The medications include hydrochlorothiazide, enalapril, and a daily multivitamin. The family history is noncontributory. He consumes alcohol in moderation. His diet mostly consists of red meat and white rice. The blood pressure is 137/85 mm Hg, heart rate is 74/min, respiratory rate is 12/min, and the temperature is 36.9°C (98.4°F). The physical examination demonstrates swelling, redness, and tenderness to palpation in the first metatarsophalangeal joint of his right foot. There are no skin lesions. The rest of the patient’s examination is normal. An arthrocentesis procedure is scheduled. Which of the following is the most likely pharmacological treatment for the presented patient?
A 60-year-old man comes to the physician because of a 2-day history of blood in his urine, lower abdominal pain, and a burning sensation while micturating. Five months ago, he was diagnosed with high-grade non-Hodgkin lymphoma and a deep vein thrombosis of his right popliteal vein. His medications include polychemotherapy every 3 weeks and a daily subcutaneous dose of low molecular weight heparin. The last cycle of chemotherapy was 2 weeks ago. His temperature is 37°C (98.6°F), pulse is 94/min, and blood pressure is 110/76 mm Hg. Examination shows bilateral axillary and inguinal lymphadenopathy, hepatosplenomegaly, and mild suprapubic tenderness. Laboratory studies show: Hemoglobin 10.2 g/dL Leukocytes 4,300/mm3 Platelet count 145,000/mm3 Partial thromboplastin time 55 seconds Prothrombin time 11 seconds (INR=1) Urine RBCs 50–55/hpf RBC casts negative WBCs 7/hpf Epithelial cells 5/hpf Bacteria occasional Administration of which of the following is most likely to have prevented this patient's current condition?
A 45-year-old woman presents to the office complaining of fatigue and unintentional weight loss. On examination, there is a palpable firm lymph node in the cervical area. Biopsy of the lymph node reveals Hodgkin’s lymphoma. The patient agrees to start the standard chemotherapy regimen. A few months later, after the completion of 3 successful courses, the patient presents with a dry cough and progressively worsening shortness of breath. Her temperature is 37°C (98.6°F), the blood pressure is 110/70 mm Hg, the pulse is 72/min, and the respirations are 16/min. Pulse oximetry shows an O2 saturation of 94% on room air. On spirometry, the patient's FEV1/FVC ratio is normal. Chest CT reveals bilateral diffuse cystic airspaces in middle and lower lung fields. Which of the following is the most likely cause of this patient’s current symptoms?
A 65-year-old man comes to the physician for a routine health maintenance examination. He feels well. His most recent examination 2 years ago included purified protein derivative (PPD) skin testing and showed no abnormalities. He is a retired physician and recently came back from rural China where he completed a voluntary service at a local healthcare center. A PPD skin test is performed. Three days later, an induration of 12 mm is noted. An x-ray of the chest shows no abnormalities. He is started on a drug that inhibits the synthesis of mycolic acid. This patient is at greatest risk of developing which of the following adverse effects?
A 25-year-old woman is brought to the emergency department because of a 1-day history of lower abdominal pain and vaginal bleeding. Her last menstrual period was 7 weeks ago. A urine pregnancy test is positive. A pelvic ultrasound shows a normal appearing uterus with an empty intrauterine cavity and a minimal amount of free pelvic fluid. Treatment with a drug is begun. Which of the following is the most likely effect of this drug?
A 34-year-old male comes to his family physician with complaints of joint pain that has been present for over 7 weeks. Prior to the onset of his arthritis, he recalls having a gastrointestinal infection which caused mild diarrhea and abdominal cramps. He recovered well and had no issues until his joint pain started. A prescription for naproxen was previously prescribed but he still does not feel well. He has no significant past medical or family history. On physical examination, his blood pressure is 120/78 mm Hg, respirations are 17/min, pulse is 64/min, and temperature is 36.7°C (98.0°F). Which of the following therapies is likely to be most beneficial in treating this patient’s condition?
A 35-year-old man comes to the physician because of a 4-month history of intermittent headaches. They have been getting progressively worse and no longer respond to ibuprofen. He also complains of weight gain and excessive sweating. Physical examination shows prominent supraorbital ridges, prognathism, macroglossia with thick lips, and disproportionately broad hands and feet. There is decreased peripheral vision bilaterally on visual field testing. An MRI of the brain shows a mass in the sella turcica. Genetic analysis of a biopsy specimen from the mass shows cells that overexpress adenylyl cyclase. Which of the following is the most appropriate pharmacotherapy for this condition?
A 32-year-old man presents to the clinic for follow up for treatment of latent tuberculosis. He is a healthcare worker and began isoniazid 3 months ago after a routine PPD yielded a 12-mm induration. He feels otherwise well and attributes this to his vegetarian diet that he has been following for the past 4 years. His past medical history is unremarkable, but his family history is significant for a "liver disease," the specifics of which are unknown. Physical exam shows mildly reduced sensation to pinprick over the distal lower extremities. The abdomen is soft, nontender, and without hepatosplenomegaly. Laboratory studies demonstrate the following: Serum: Hemoglobin: 9.6 g/dL Hematocrit: 34% Leukocyte count: 9,200/mm^3 with normal differential Platelets: 270,000/mm^3 Mean corpuscular volume: 77 µm^3 AST: 92 U/L ALT: 84 U/L Ferritin: 302 ng/mL (normal 15-200 ng/mL) Total iron: 273 µg/dL (normal 50-170 µg/dL) TIBC: 150 µg/dL (normal 250–370 µg/dL) Which of the following is the most appropriate next step in management?
Practice by Chapter
Antiparasitic drugs (antiprotozoals)
Practice Questions
Antimalarial medications
Practice Questions
Anthelmintics
Practice Questions
Antiseptics and disinfectants
Practice Questions
Antimicrobial stewardship principles
Practice Questions
Empiric antimicrobial selection
Practice Questions
Antimicrobial dosing in special populations
Practice Questions
Antimicrobial pharmacokinetics/pharmacodynamics
Practice Questions
Antimicrobial toxicities
Practice Questions
Antimicrobial allergies and cross-reactivity
Practice Questions
Combination antimicrobial therapy
Practice Questions
Cost-effective antimicrobial strategies
Practice Questions
New antimicrobial development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app