
Labor Complications — MCQs

On this page
A 17-year-old woman presents to an OBGYN clinic for evaluation of primary amenorrhea. She is a well-developed well-nourished woman who looks at her stated age. She has reached Tanner stage IV breast and pubic hair development. The external genitalia is normal in appearance. She has an older sister who underwent menarche at 12 years of age. A limited pelvic exam reveals a shortened vaginal canal with no cervix. No uterus is visualized during an ultrasound exam, but both ovaries are noted. What is the likely pathophysiology underlying this condition?
A 22-year-old woman comes to the physician for a routine health maintenance examination. She has no history of serious illness. Pelvic examination shows a pink, 2 x 2-cm, fluctuant swelling at the right posterior vaginal introitus. The swelling is most likely derived from which of the following structures?
A 27-year-old woman G2P1 at 34 weeks estimated gestational age presents with bouts of sweating, weakness, and dizziness lasting a few minutes after lying down on the bed. She says symptoms resolve if she rolls on her side. She reports that these episodes have occurred several times over the last 3 weeks. On lying down, her blood pressure is 90/50 mm Hg and her pulse is 50/min. When she rolls on her side, her blood pressure slowly increases to 120/65 mm Hg, and her pulse increases to 72/min. Which of the following best describes the mechanism which underlies this patient’s most likely condition?
A 40-year-old woman visits your office with her pathology report after being subjected to total abdominal hysterectomy a month ago. She explains that she went through this procedure after a long history of lower abdominal pain that worsened during menses and heavy menstrual bleeding. She is a mother of 5 children, and they are all delivered by cesarean section. The pathology gross examination report and microscopic examination report from the specimen from surgery describes an enlarged, globular uterus with invading clusters of endometrial tissue within the myometrium. What is the most likely diagnosis for this patient?
A 25-year-old G2P1001 at 32 weeks gestation presents to the hospital with painless vaginal bleeding. The patient states that she was taking care of laundry at home when she experienced a sudden sensation of her water breaking and saw that her groin was covered in blood. Her prenatal history is unremarkable according to the clinic records, but she has not seen an obstetrician for the past 14 weeks. Her previous delivery was by urgent cesarean section for placenta previa. Her temperature is 95°F (35°C), blood pressure is 125/75 mmHg, pulse is 79/min, respirations are 18/min, and oxygen saturation is 98% on room air. Cervical exam shows gross blood in the vaginal os. The fetal head is not palpable. Fetal heart rate monitoring demonstrates decelerations and bradycardia. Labs are pending. IV fluids are started. What is the best next step in management?
A 35-year-old female presents to your office with complaints of painful bleeding between regular menstrual cycles, pain during sexual intercourse, and postcoital bleeding for the past 6 months. She also gives a long history of mild, crampy, vague, lower abdominal pain, but has never sought medical attention. She underwent surgical sterilization after her first and only child 7 years ago with no other significant events in her medical history. The last Pap smear, 1 year ago, was reported as reactive inflammation and negative for malignancy. Upon pelvic examination, you note a mucopurulent discharge, cervical motion tenderness, and endocervical bleeding when passing a cotton swab through the cervical os. Which of the following is the most likely diagnosis?
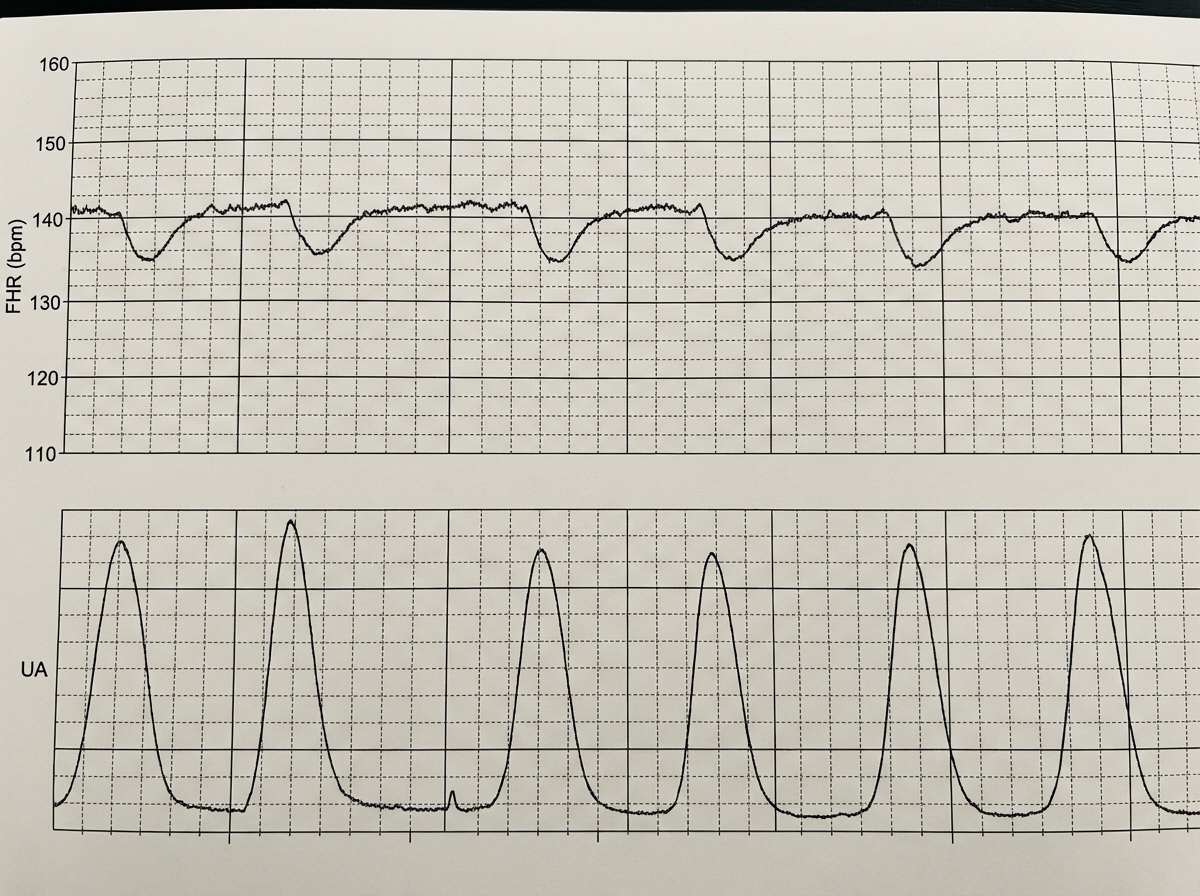
A 39-year-old woman, gravida 5, para 4, at 41 weeks' gestation is brought to the hospital because of regular uterine contractions that started 2 hours ago. Pregnancy has been complicated by iron deficiency anemia treated with iron supplements. Pelvic examination shows the cervix is 90% effaced and 7-cm dilated; the vertex is at -1 station. Fetal heart tracing is shown. The patient is repositioned, O2 therapy is initiated, and amnioinfusion is done. A repeat assessment after 20 minutes shows a similar cervical status, and no changes in the fetal heart tracing, and less than 5 contractions in a period of 10 minutes.What is the most appropriate next step in management?
A 31-year-old G3P0 is admitted to the hospital with profuse vaginal bleeding and abdominal pain at 34 weeks gestation. She reports passing bright blood with clots and no water in the discharge. She denies recent trauma or medical illnesses. She had no prenatal care. Her previous pregnancies culminated in spontaneous abortions in the second trimester. She has a 6-year history of drug abuse and cocaine smoking 2 hours prior to the onset of her symptoms. Her blood pressure is 160/90 mm Hg, the heart rate is 93/min, the respiratory rate is 19/min, and the temperature is 36.9℃ (98.4℉). The fetal heart rate is 110/min. On examination, the patient is lethargic. Her pupils are constricted, but reactive to light bilaterally. There are no signs of trauma. Abdominal palpation identifies lower abdominal tenderness and strong uterine contractions. The fundus of the uterus is between the xiphoid process and umbilicus. The patient’s perineum is grossly bloody. On pelvic examination, the vaginal canal is without lesions. The cervix is almost completely effaced and 2 cm dilated. Which of the following options is the most likely cause of the patient’s pregnancy-related condition?
A 24-year-old woman comes to the emergency department because of lower abdominal pain for 4 hours. She has had vaginal spotting for 2 days. Menses occur at irregular 20- to 45-day intervals and last for 3 to 7 days. Her last menstrual period was 8 weeks ago. She was treated for pelvic inflammatory disease at the age of 20 years with ceftriaxone and azithromycin. She is sexually active with one male partner and uses condoms inconsistently. Her pulse is 118/min, respirations are 20/min, and blood pressure is 118/66 mm Hg. Examination shows lower abdominal tenderness. Pelvic examination shows a closed cervix and a uterus of normal size with right adnexal tenderness. Her serum β-human chorionic gonadotropin concentration is 16,000 mIU/mL (N < 5). Transvaginal ultrasonography shows a 5-cm hypoechoic lesion at the junction of the fallopian tube and uterine cavity with a 3-mm layer of myometrium surrounding it. Which of the following is the most likely diagnosis?
A 24-year-old primigravid woman at 38 weeks' gestation comes to the physician for a prenatal visit. At the last two prenatal visits, transabdominal ultrasound showed the fetus in breech presentation. She has no medical conditions and only takes prenatal vitamins. Her pulse is 95/min, respirations are 16/min, and blood pressure is 130/76 mm Hg. The abdomen is soft and nontender; no contractions are felt. Pelvic examination shows a closed cervical os and a uterus consistent with 38 weeks' gestation. The fetal rate tracing shows a baseline heart rate of 152/min and 2 accelerations over 10 minutes. Repeat ultrasound today shows a persistent breech presentation. The patient states that she would like to attempt a vaginal delivery. Which of the following is the most appropriate next step in management?
Practice by Chapter
Preterm labor management
Practice Questions
Premature rupture of membranes
Practice Questions
Chorioamnionitis
Practice Questions
Abnormal labor patterns
Practice Questions
Shoulder dystocia management
Practice Questions
Umbilical cord prolapse
Practice Questions
Malpresentations (breech, face, brow)
Practice Questions
Trial of labor after cesarean
Practice Questions
Uterine rupture
Practice Questions
Placental abruption
Practice Questions
Placenta previa
Practice Questions
Amniotic fluid embolism
Practice Questions
Fetal heart rate abnormalities
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app