A 27-year-old male who works on an organic farm is diagnosed with infection by N. americanus, a helminthic parasite. Eosinophils require which antibody isotype to destroy these parasites via antibody-dependent cellular cytotoxicity?
Q2
A 29-year-old man presents to the clinic with several days of flatulence and greasy, foul-smelling diarrhea. He says that he was on a camping trip last week after which his symptoms started. When asked further about his camping activities, he reports collecting water from a stream but did not boil or chemically treat the water. The patient also reports nausea, weight loss, and abdominal cramps followed by sudden diarrhea. He denies tenesmus, urgency, and bloody diarrhea. His temperature is 37°C (98.6° F), respiratory rate is 15/min, pulse is 107/min, and blood pressure is 89/58 mm Hg. A physical examination is performed where nothing significant was found except for dry mucous membranes. Intravenous fluids are started and a stool sample is sent to the lab, which reveals motile protozoa on microscopy, negative for any ova, no blood cells, and pus cells. What is the most likely diagnosis?
Q3
A 34-year-old woman with HIV comes to the emergency department because of a 2-week history of diarrhea and abdominal cramping. She has had up to 10 watery stools per day. She also has anorexia and nausea. She returned from a trip to Mexico 4 weeks ago where she went on two hiking trips and often drank from spring water. She was diagnosed with HIV 12 years ago. She says that she has been noncompliant with her therapy. Her last CD4+ T-lymphocyte count was 85/mm3. She appears thin. She is 175 cm (5 ft 9 in) tall and weighs 50 kg (110 lb); BMI is 16.3 kg/m2. Her temperature is 38.3°C (100.9°F), pulse is 115/min, and blood pressure is 85/65 mm Hg. Examination shows dry mucous membranes. The abdomen is soft, and there is diffuse tenderness to palpation with no guarding or rebound. Bowel sounds are hyperactive. Microscopy of a modified acid-fast stain on a stool sample reveals oocysts. Which of the following is the most likely causal organism?
Q4
A 31-year-old man comes to the physician because of a 2-day history of abdominal pain and diarrhea. He reports that his stools are streaked with blood and mucus. He returned from a vacation in the Philippines 3 weeks ago. His vital signs are within normal limits. Abdominal examination shows hyperactive bowel sounds. A photomicrograph of a trichrome-stained wet mount of a stool specimen is shown. Which of the following organisms is the most likely cause of this patient's symptoms?
Q5
A 62-year-old man is referred to a gastroenterologist because of difficulty swallowing for the past 5 months. He has difficulty swallowing both solid and liquid foods, but there is no associated pain. He denies any shortness of breath or swelling in his legs. He immigrated from South America 10 years ago. He is a non-smoker and does not drink alcohol. His physical examination is unremarkable. A barium swallow study was ordered and the result is given below. Esophageal manometry confirms the diagnosis. What is the most likely underlying cause of this patient’s condition?
Protozoa/Helminths US Medical PG Practice Questions and MCQs
Question 1: A 27-year-old male who works on an organic farm is diagnosed with infection by N. americanus, a helminthic parasite. Eosinophils require which antibody isotype to destroy these parasites via antibody-dependent cellular cytotoxicity?
A. IgE (Correct Answer)
B. IgA
C. IgG
D. IgM
E. IgD
Explanation: ***IgE***
- **IgE** antibodies are crucial in the immune response against helminthic parasites, including *N. americanus*, by sensitizing **mast cells** and **eosinophils**.
- When **IgE** binds to the surface of parasites, the **Fc receptor** on eosinophils recognizes the Fc portion of IgE, leading to the release of cytotoxic granules that destroy the parasite (antibody-dependent cellular cytotoxicity).
*IgA*
- **IgA** is primarily found in **mucosal secretions** and plays a role in defending against pathogens at mucosal surfaces, but it is not the primary isotype involved in eosinophil-mediated **ADCC** against helminths.
- While IgA can bind to some immune cells, its main function is to **neutralize toxins** and prevent microbial adhesion at mucosal sites.
*IgG*
- **IgG** is the most abundant antibody in serum and is involved in various immune functions, including **opsonization**, **neutralization**, and **complement activation**.
- Although IgG can mediate ADCC by **NK cells** and **macrophages**, it is not the primary isotype for eosinophil-mediated killing of helminths, which is dominated by IgE.
*IgM*
- **IgM** is typically the first antibody produced during a primary immune response and is very effective at **activating the complement system**.
- Its large pentameric structure also limits its diffusion into tissues, and it does not play a direct role in eosinophil-mediated ADCC against helminthic parasites.
*IgD*
- **IgD** primarily functions as a **B cell receptor** on naive B lymphocytes, signaling for their activation and differentiation.
- It is present in very low concentrations in serum and its role in host defense against parasites or in ADCC is negligible.
Question 2: A 29-year-old man presents to the clinic with several days of flatulence and greasy, foul-smelling diarrhea. He says that he was on a camping trip last week after which his symptoms started. When asked further about his camping activities, he reports collecting water from a stream but did not boil or chemically treat the water. The patient also reports nausea, weight loss, and abdominal cramps followed by sudden diarrhea. He denies tenesmus, urgency, and bloody diarrhea. His temperature is 37°C (98.6° F), respiratory rate is 15/min, pulse is 107/min, and blood pressure is 89/58 mm Hg. A physical examination is performed where nothing significant was found except for dry mucous membranes. Intravenous fluids are started and a stool sample is sent to the lab, which reveals motile protozoa on microscopy, negative for any ova, no blood cells, and pus cells. What is the most likely diagnosis?
A. Traveler’s diarrhea due to ETEC
B. Irritable bowel syndrome
C. C. difficile colitis
D. Giardiasis (Correct Answer)
E. Traveler’s diarrhea due to Norovirus
Explanation: ***Giardiasis***
- The patient's history of drinking untreated stream water after a camping trip, followed by **greasy, foul-smelling diarrhea**, flatulence, nausea, and weight loss, is highly characteristic of **giardiasis**.
- The stool microscopy finding of **motile protozoa** without blood cells or pus cells confirms the presence of *Giardia lamblia* infection, which is a common cause of such symptoms in campers.
*Traveler’s diarrhea due to ETEC*
- **ETEC (Enterotoxigenic *Escherichia coli*)** typically causes watery diarrhea, often without the prominent greasy, foul-smelling, and chronic nature seen in this case.
- While ETEC is a common cause of traveler's diarrhea, the **microscopic finding of motile protozoa** in the stool definitively rules out a bacterial cause like ETEC.
*Irritable bowel syndrome*
- **Irritable bowel syndrome (IBS)** is a chronic functional disorder of the bowel, characterized by abdominal pain, bloating, and altered bowel habits (diarrhea, constipation, or both), but it does not have an acute onset directly linked to water consumption or involve **motile protozoa** in the stool.
- IBS is a diagnosis of exclusion and would not be considered in the presence of a clear infectious etiology identified by stool examination.
*C. difficile colitis*
- **Clostridioides difficile colitis** typically presents with watery to bloody diarrhea, abdominal pain, and fever, usually following **antibiotic use** or in hospitalized patients, none of which are reported here.
- The stool microscopy would show evidence of *C. difficile* toxins, not **motile protozoa**, and would often reveal pus cells or inflammatory markers.
*Traveler’s diarrhea due to Norovirus*
- **Norovirus** typically causes acute onset of vomiting, watery diarrhea, and abdominal cramps, often resolving within a few days, but it is a **viral infection**.
- The detection of **motile protozoa** on stool microscopy rules out a viral etiology like Norovirus.
Question 3: A 34-year-old woman with HIV comes to the emergency department because of a 2-week history of diarrhea and abdominal cramping. She has had up to 10 watery stools per day. She also has anorexia and nausea. She returned from a trip to Mexico 4 weeks ago where she went on two hiking trips and often drank from spring water. She was diagnosed with HIV 12 years ago. She says that she has been noncompliant with her therapy. Her last CD4+ T-lymphocyte count was 85/mm3. She appears thin. She is 175 cm (5 ft 9 in) tall and weighs 50 kg (110 lb); BMI is 16.3 kg/m2. Her temperature is 38.3°C (100.9°F), pulse is 115/min, and blood pressure is 85/65 mm Hg. Examination shows dry mucous membranes. The abdomen is soft, and there is diffuse tenderness to palpation with no guarding or rebound. Bowel sounds are hyperactive. Microscopy of a modified acid-fast stain on a stool sample reveals oocysts. Which of the following is the most likely causal organism?
A. Entamoeba histolytica
B. Cytomegalovirus
C. Cryptosporidium parvum (Correct Answer)
D. Giardia lamblia
E. Rotavirus
Explanation: ***Cryptosporidium parvum***
- This patient's **immunosuppressed state** (HIV with CD4 count of 85/mm3), severe **watery diarrhea**, and history of drinking **spring water** are highly suggestive of cryptosporidiosis.
- The finding of **oocysts** on modified acid-fast stain is the definitive diagnostic test for *Cryptosporidium*.
*Entamoeba histolytica*
- While *Entamoeba histolytica* can cause diarrhea, it typically presents with **bloody stools (dysentery)** and may cause **liver abscesses**, which are not described here.
- Diagnosis involves identifying trophozoites or cysts in stool, not acid-fast oocysts.
*Cytomegalovirus*
- **CMV colitis** can cause diarrhea in immunocompromised patients, but it is typically diagnosed by **biopsy showing inclusions** and is not characterized by acid-fast oocysts in stool.
- CMV often presents with systemic symptoms, and while abdominal pain is common, the specific stool findings point elsewhere.
*Giardia lamblia*
- *Giardia lamblia* causes **greasy, foul-smelling stools** and **malabsorption**, often without fever, and is diagnosed by finding **cysts or trophozoites** in stool, which are not acid-fast oocysts.
- While acquired from contaminated water, the clinical picture and diagnostic test differ markedly.
*Rotavirus*
- **Rotavirus** is a common cause of severe watery diarrhea, especially in **infants and young children**, but it is less common in adults without specific risk factors and is not diagnosed by acid-fast oocysts.
- It does not specifically target immunocompromised individuals like *Cryptosporidium* does in this context.
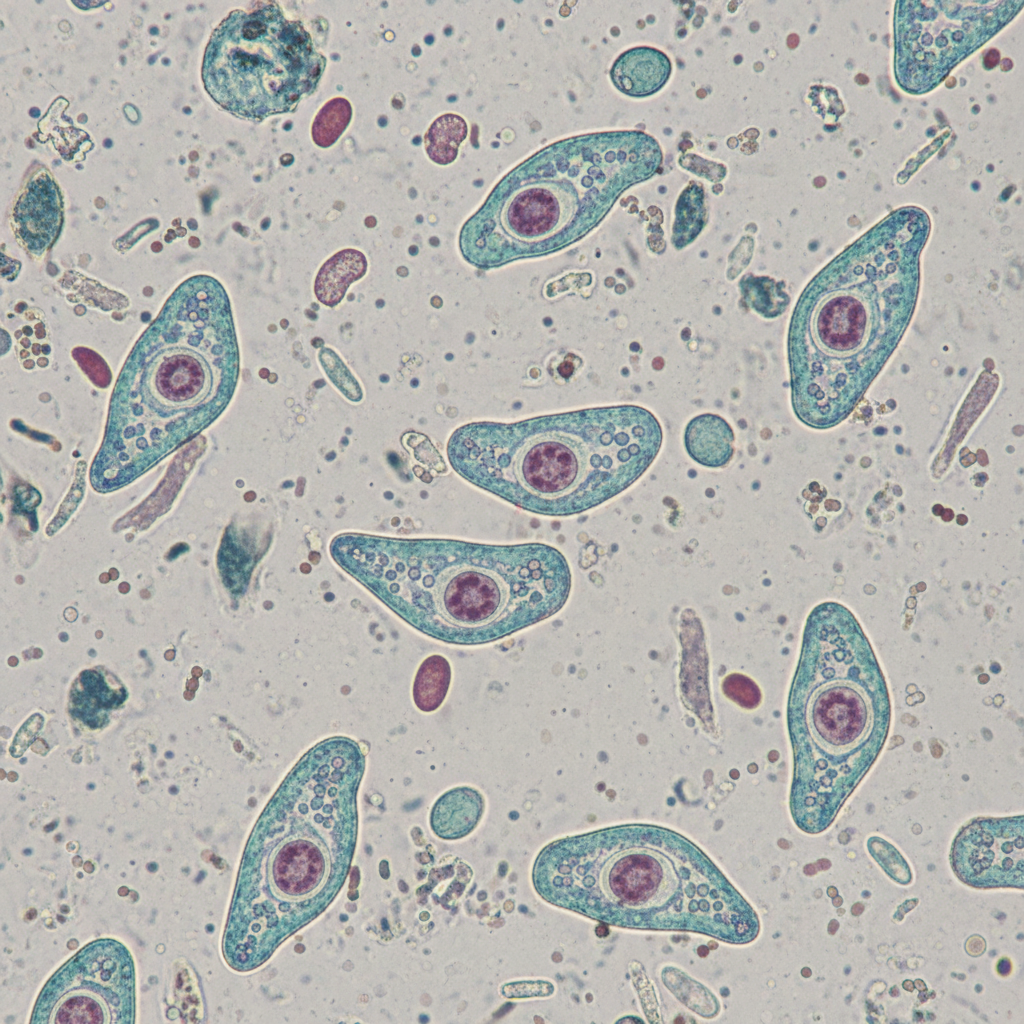
Question 4: A 31-year-old man comes to the physician because of a 2-day history of abdominal pain and diarrhea. He reports that his stools are streaked with blood and mucus. He returned from a vacation in the Philippines 3 weeks ago. His vital signs are within normal limits. Abdominal examination shows hyperactive bowel sounds. A photomicrograph of a trichrome-stained wet mount of a stool specimen is shown. Which of the following organisms is the most likely cause of this patient's symptoms?
A. Campylobacter jejuni
B. Giardia lamblia
C. Cryptosporidium parvum
D. Shigella dysenteriae
E. Entamoeba histolytica (Correct Answer)
Explanation: ***Entamoeba histolytica***
- The patient's symptoms of **bloody, mucoid diarrhea** (dysentery) after travel to the **Philippines** are highly suggestive of **amebic dysentery** caused by *Entamoeba histolytica*.
- A **trichrome-stained wet mount** of stool revealing trophozoites or cysts of *Entamoeba histolytica* in this clinical context would confirm the diagnosis.
*Campylobacter jejuni*
- While *Campylobacter jejuni* can cause **bloody diarrhea** and is a common cause of **traveler's diarrhea**, it is a **bacterial infection**, and the question implies a parasitic etiology with the mention of a trichrome-stained wet mount.
- Infection is typically associated with consumption of undercooked poultry or contaminated water.
*Giardia lamblia*
- *Giardia lamblia* causes **giardiasis**, which typically presents with **non-bloody, watery diarrhea**, **steatorrhea**, abdominal cramps, and bloating.
- It does not usually cause **dysentery** or bloody stools.
*Cryptosporidium parvum*
- *Cryptosporidium parvum* causes **cryptosporidiosis**, characterized by **profuse, watery diarrhea** and abdominal cramps.
- While it can be severe in immunocompromised individuals, it typically does not cause **bloody or mucoid stools** (dysentery).
*Shigella dysenteriae*
- *Shigella dysenteriae* causes **shigellosis**, a severe form of dysentery with **bloody, mucoid stools**, fever, and tenesmus.
- While it fits the clinical picture of dysentery, the diagnostic method mentioned (trichrome-stained wet mount) is primarily used for identifying **parasitic organisms**, not bacteria like *Shigella*.
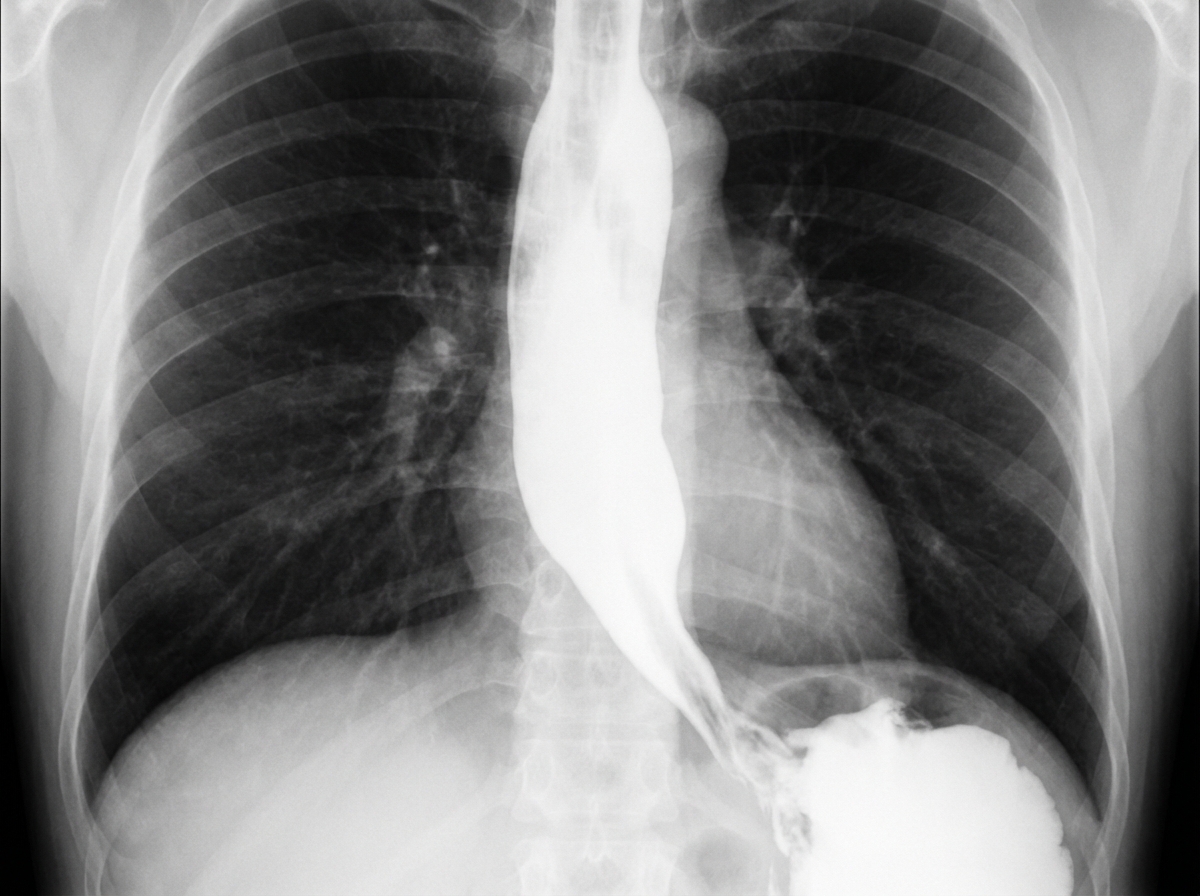
Question 5: A 62-year-old man is referred to a gastroenterologist because of difficulty swallowing for the past 5 months. He has difficulty swallowing both solid and liquid foods, but there is no associated pain. He denies any shortness of breath or swelling in his legs. He immigrated from South America 10 years ago. He is a non-smoker and does not drink alcohol. His physical examination is unremarkable. A barium swallow study was ordered and the result is given below. Esophageal manometry confirms the diagnosis. What is the most likely underlying cause of this patient’s condition?
A. Pharyngoesophageal diverticulum
B. Chagas disease (Correct Answer)
C. Esophageal rupture
D. Gastroesophageal reflux disease
E. Squamous cell carcinoma of the esophagus
Explanation: ***Chagas disease***
- The patient's history of living in **South America** and presenting with **dysphagia for both solids and liquids** (suggesting a motility disorder), along with the **barium swallow image showing esophageal dilation and a 'bird's beak' appearance** at the gastroesophageal junction, are highly characteristic of achalasia caused by Chagas disease.
- Chagas disease, caused by *Trypanosoma cruzi*, leads to the destruction of **myenteric plexus neurons** in the esophagus, resulting in achalasia (failure of the lower esophageal sphincter to relax) and megaesophagus.
*Pharyngoesophageal diverticulum*
- This typically presents as **Zenker's diverticulum**, causing **difficulty initiating a swallow**, regurgitation of undigested food, and sometimes halitosis, which is different from the described dysphagia for both solids and liquids.
- A Zenker's diverticulum would appear as a **pouch-like protrusion** in the posterior pharynx, not the diffuse esophageal dilation seen in the image.
*Esophageal rupture*
- Esophageal rupture (Boerhaave syndrome) is an acute, life-threatening condition associated with **severe chest pain, vomiting, and crepitus**, not a chronic, progressive dysphagia without pain.
- Imaging would reveal **extravasation of contrast** into the mediastinum or pleural space, not the smooth dilation and distal narrowing observed.
*Gastroesophageal reflux disease*
- While chronic GERD can lead to **strictures** and dysphagia, it typically causes **heartburn**, regurgitation, and sometimes odynophagia, and the dysphagia is usually progressive for solids first.
- The barium swallow would show reflux or a stricture, not the **classic achalasia findings** of a dilated esophagus tapering to a narrow distal segment.
*Squamous cell carcinoma of the esophagus*
- Squamous cell carcinoma usually presents with **progressive dysphagia, initially for solids**, and is often associated with weight loss, smoking, and alcohol use, none of which are present in this patient.
- A tumor would typically appear as an **irregular, focal narrowing or mass** on barium swallow, not the smooth, diffuse dilation seen in this image.