
Gastroenterology — MCQs

On this page
A 53-year-old woman presents to the office complaining of an extreme, nonradiating stabbing pain in the epigastric region after having a meal. She states that it has happened several times in the past week approximately 30 minutes after eating and spontaneously resolves. A day before, the patient went to urgent care with the same complaint, but the abdominal X-ray was normal. Surgical history is remarkable for a total knee arthroplasty procedure 6 months ago. She has lost 34 kg (75 lb) since the operation because of lifestyle changes. The vital signs are normal. Laparoscopic surgical scars are well healed. Endoscopy shows benign mucosa to the proximal duodenum. A barium swallow study reveals an extremely narrowed duodenum. Which of the following structures is most likely responsible for this patient’s current symptoms?
A 55-year-old man comes to the physician because of heartburn for the past 2 years. He has no chest pain, dysphagia, weight loss, or fever. He has no history of any serious illnesses. He takes omeprazole daily. Vital signs are within normal limits. Body mass index (BMI) is 34 kg/m2. Physical exam shows no abnormalities. An endoscopic image of the lower esophageal sphincter is shown. Which of the following is the most important next step in management?
A 48-year-old man presents to an urgent care center with epigastric discomfort following meals and an occasional dry cough worse in the morning, both of which have increased in frequency over the past several months. He is otherwise healthy and has no additional complaints. Past medical history is significant for major depressive disorder, anxiety, and hypothyroidism. Physical examination is unremarkable. His vital signs include temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 74/min, and respiratory rate 14/min. Given the following options, what is the most appropriate next step in patient management?
A 56-year-old man comes to the clinic complaining of intermittent abdominal pain for the past 2 months. He reports that the pain improves with oral intake and is concentrated at the epigastric area. The pain is described as gnawing in quality and improves when he takes his wife’s ranitidine. He denies weight changes, fever, chest pain, or recent travel but endorses “brain fog” and decreased libido. An upper endoscopy reveals ulcerations at the duodenum and jejunum. Physical examination demonstrates bilateral hemianopsia, gynecomastia, and diffuse pain upon palpation at the epigastric area. Laboratory findings are demonstrated below: Serum: Na+: 137 mEq/dL Cl-: 96 mEq/L K+: 3.9 mEq/dL HCO3-: 25 mEq/L Glucose: 110 mg/dL Creatinine: .7 mg/dL Ca2+: 13.5 mg/dL What is the best explanation for this patient’s findings?
A 41-year-old man presents to the office with pain in his right big toe. The pain started yesterday and has been progressively getting worse to the point that it is difficult to walk. He describes his right big toe as being swollen and hot to the touch. He has never had symptoms like this before. He drinks 3 beers per night. Medical history is otherwise significant for chronic kidney disease. Physical examination is notable for an overweight gentleman in moderate pain, with an erythematous, swollen and tender right toe. He is afebrile. A joint fluid analysis in this patient is most likely to show what?
A 24-year-old man comes to the physician for a routine health maintenance examination. He feels well. He has type 1 diabetes mellitus. His only medication is insulin. He immigrated from Nepal 2 weeks ago . He lives in a shelter. He has smoked one pack of cigarettes daily for the past 5 years. He has not received any routine childhood vaccinations. The patient appears healthy and well nourished. He is 172 cm (5 ft 8 in) tall and weighs 68 kg (150 lb); BMI is 23 kg/m2. His temperature is 36.8°C (98.2°F), pulse is 72/min, and blood pressure is 123/82 mm Hg. Examination shows a healed scar over his right femur. The remainder of the examination shows no abnormalities. A purified protein derivative (PPD) skin test is performed. Three days later, an induration of 13 mm is noted. Which of the following is the most appropriate initial step in the management of this patient?
A 42-year-old man is brought to the emergency department by his wife because of a 1-day history of progressive confusion. He recently lost his job. He has a history of chronic alcoholism and has been drinking 14 beers daily for the past week. Before this time, he drank 6 beers daily. He appears lethargic. His vital signs are within normal limits. Serum studies show a sodium level of 111 mEq/L and a potassium level of 3.7 mEq/L. Urgent treatment for this patient's current condition increases his risk for which of the following adverse events?
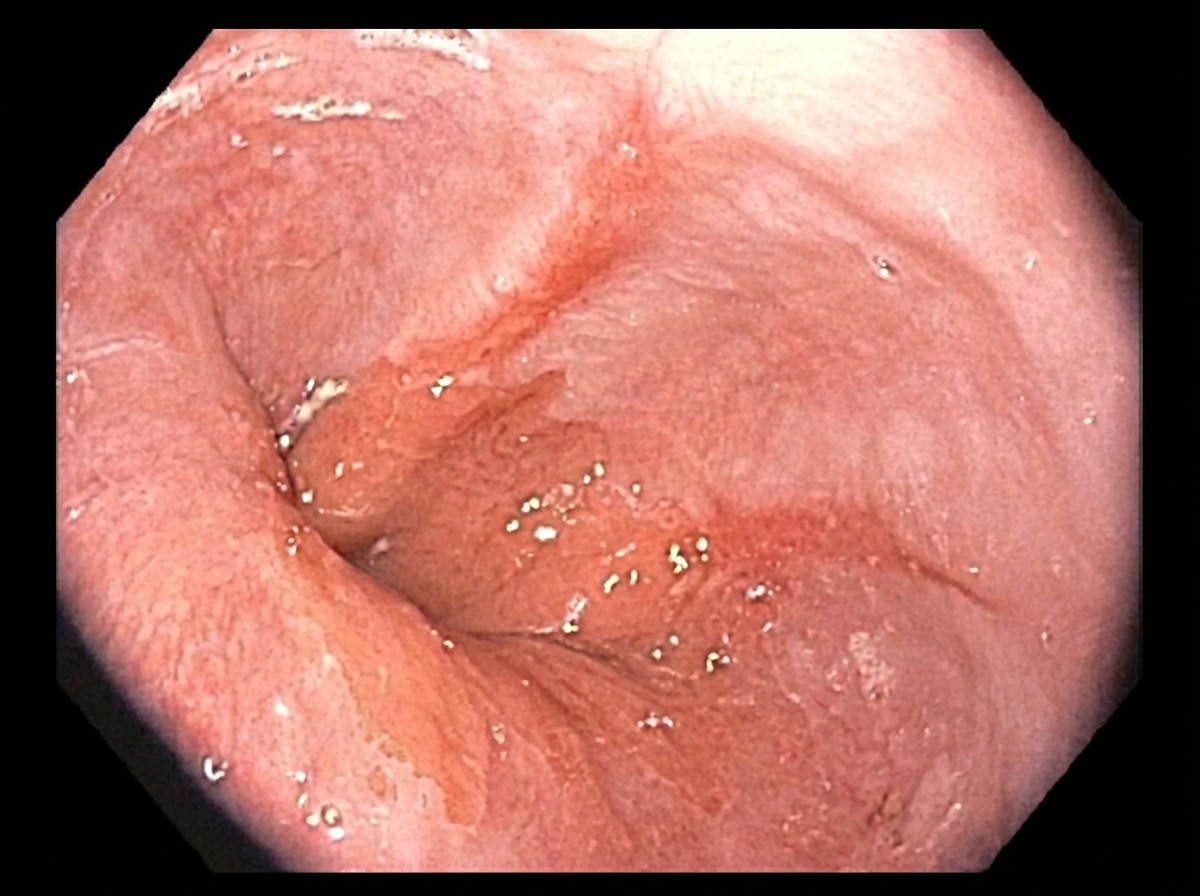
A 47-year-old man presents with upper GI (upper gastrointestinal) bleeding. The patient is known to have a past medical history of peptic ulcer disease and was previously admitted 4 years ago for the same reason. He uses proton-pump inhibitors for his peptic ulcer. Upon admission, the patient is placed on close monitoring, and after 8 hours, his hematocrit is unchanged. The patient has also been hemodynamically stable after initial fluid resuscitation. An upper endoscopy is performed. Which of the following endoscopy findings most likely indicates that this patient will not experience additional GI bleeding in the next few days?
A 76-year-old Japanese man is admitted to the hospital because of a 3-month history of loose stools and worsening peripheral edema. He also reports fatigue, a 10-pound weight loss over the past 6 weeks, and a tingling sensation in his hands and feet over the same time period. Aside from the family dog, he has not had contact with animals for over 1 year and has not traveled outside the country. He has hypertension and benign prostatic hyperplasia. Five years ago, he underwent a partial gastrectomy with jejunal anastomosis for gastric cancer. Current medications include hydrochlorothiazide and tamsulosin. His temperature is 36.8°C (98.2°F), pulse is 103/min, and blood pressure is 132/83 mm Hg. Examination shows a soft and nontender abdomen. There is a well-healed scar on the upper abdomen. Cardiopulmonary examination shows no abnormalities. The conjunctivae appear pale. Sensation to vibration and position is absent over the lower extremities. His hemoglobin concentration is 9.9 g/dL, MCV is 108 μm3, total protein 3.9 g/dL, and albumin 1.9 g/dL. Which of the following is the most likely cause of this patient's condition?
A 25-year-old woman presents to the emergency department with nausea and vomiting. She denies any recent illnesses, sick contacts, or consumption of foods outside of her usual diet. She reports smoking marijuana at least three times a day. Her temperature is 97.7°F (36.5°C), blood pressure is 90/74 mmHg, pulse is 100/min, respirations are 10/min, and SpO2 is 94% on room air. Her conjunctiva are injected. Her basic metabolic panel is obtained below. Serum: Na+: 132 mEq/L Cl-: 89 mEq/L K+: 2.9 mEq/L HCO3-: 30 mEq/L BUN: 35 mg/dL Glucose: 80 mg/dL Creatinine: 1.5 mg/dL Magnesium: 2.0 mEq/L She continues to have multiple bouts of emesis and dry retching. What is the next best step in management?
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app