
Gastroenterology — MCQs

On this page
A 52-year-old man comes to the physician because of a 5-month history of progressive lethargy, shortness of breath, and difficulty concentrating. His friends have told him that he appears pale. He has smoked half a pack of cigarettes daily for the past 20 years. Neurological examination shows reduced sensation to light touch and pinprick in the toes bilaterally. Laboratory studies show: Hemoglobin 8.2 g/dL Mean corpuscular volume 108 μm3 Serum Vitamin B12 (cyanocobalamin) 51 ng/L (N = 170–900) Folic acid 13 ng/mL (N = 5.4–18) An oral dose of radiolabeled vitamin B12 is administered, followed by an intramuscular injection of nonradioactive vitamin B12. A 24-hour urine sample is collected and urine vitamin B12 levels are unchanged. The procedure is repeated with the addition of oral intrinsic factor, and 24-hour urine vitamin B12 levels increase. This patient's findings indicate an increased risk for which of the following conditions?
A 70-year-old man comes to the physician for the evaluation of an 8-week history of blood in his stool. Two months ago, he had an episode of bronchitis and was treated with amoxicillin. Since then, he has noticed blood in his stool and on the toilet paper occasionally. The patient has had intermittent constipation for the past 5 years. Six months ago, he had severe left lower quadrant pain and fever that resolved with antibiotic therapy. He underwent a colonoscopy 3 years ago, which did not show any evidence of malignancy. He takes levothyroxine for hypothyroidism. He had smoked one pack of cigarettes daily for 45 years, but quit smoking 10 years ago. He drinks one glass of red wine every night. He appears pale. He is 180 cm (5 ft 11 in) tall and weighs 98 kg (216 lb); BMI is 32 kg/m2. His temperature is 36°C (96.8°F), pulse is 85/min, and blood pressure is 135/80 mm Hg. Physical examination shows pale conjunctivae. Cardiopulmonary examination shows no abnormalities. The abdomen is soft and nontender with no organomegaly. Digital rectal examination shows no masses. Test of the stool for occult blood is positive. Laboratory studies show: Hemoglobin 11 g/dL Mean corpuscular volume 76 μm3 Red cell distribution width 17% (N = 13–15) Leukocyte count 5,000/mm3 Which of the following is the most likely diagnosis?
A 58-year-old woman with a history of nephrolithiasis presents with fever and acute-onset right flank pain. The patient says that 2 days ago she developed sudden-onset right flank pain and nausea which has progressively worsened. She describes the pain as severe, colicky, localized to the right flank, and radiating to the groin. This morning she woke with a fever and foul-smelling urine. She has no significant past medical history. Vital signs are temperature 40.0°C (104.0°F), blood pressure 110/70 mm Hg, pulse 92/min, and respiratory rate 21/min. Physical examination shows severe right costovertebral angle tenderness. Her laboratory findings are significant for the following: WBC 12,500/mm3 RBC 4.20 x 106/mm3 Hematocrit 41.5% Hemoglobin 14.0 g/dL Platelet count 225,000/mm3 Urinalysis: Color Dark yellow Clarity Turbid pH 5.9 Specific gravity 1.026 Glucose None Ketones None Nitrites Positive Leukocyte esterase Positive Bilirubin Negative Urobilirubin 0.6 mg/dL Protein Trace RBC 325/hpf WBC 8,200/hpf Bacteria Many A non-contrast CT of the abdomen and pelvis shows an obstructing 7-mm diameter stone lodged at the ureteropelvic junction. There is also evidence of hydronephrosis of the right kidney. Which of the following is the best course of treatment for this patient?
A 49-year-old sexually active woman presents with dysuria and urinary frequency. She denies any previous urinary tract infections (UTIs), but she says that her mother has had frequent UTIs. Her medical history includes type 2 diabetes mellitus, hypertension, cervical cancer, and hypercholesterolemia. She currently smokes 1 pack of cigarettes per day, drinks a glass of wine per day, and denies any illicit drug use. Her vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 87/min, and respiratory rate 17/min. On physical examination, her lung sounds are clear. She has a grade 2/6 holosystolic murmur heard best over the left upper sternal border. She also has tenderness in the suprapubic area. A urinalysis shows the presence of numerous leukocytes, leukocyte esterase, and nitrites. Which of the following factors would not classify a UTI as complicated?
A 34-year-old woman visits the physician with complaints of difficulty swallowing and recurrent vomiting for the past 6 months. She even noticed food particles in her vomit a few hours after eating her meals. She has lost about 3.0 kg (6.6 lb) over the past 4 months. Her history is significant for a trip to Argentina last year. Her past medical history is insignificant. She is a non-smoker. On examination, her blood pressure is 118/75 mm Hg, respirations are 17/min, pulse is 78/min, temperature is 36.7°C (98.1°F), and her BMI is 24 kg/m². There is no abdominal tenderness, distension, or evidence of jaundice. Which of the following is the most appropriate next step in the management of this patient?
A 40-year-old man comes to the physician because of a 5-month history of watery diarrhea and episodic crampy abdominal pain. He has no fever, nausea, or vomiting. Over the past 6 months, he has had a 1.8-kg (4-lb) weight loss, despite experiencing no decrease in appetite. His wife has noticed that sometimes his face and neck become red after meals or when he is in distress. A year ago, he was diagnosed with asthma. He has hypertension. Current medications include an albuterol inhaler and enalapril. He drinks one beer daily. His temperature is 36.7°C (98°F), pulse is 85/min, and blood pressure is 130/85 mm Hg. The lungs are clear to auscultation. A grade 2/6 systolic murmur is heard best at the left sternal border and fourth intercostal space. The abdomen is soft, and there is mild tenderness to palpation with no guarding or rebound. The remainder of the physical examination shows no abnormalities. A complete blood count is within the reference range. Without treatment, this patient is at greatest risk for which of the following conditions?
A 52-year-old-woman presents to an urgent care clinic with right upper quadrant pain for the past few hours. She admits to having similar episodes of pain in the past but milder than today. Past medical history is insignificant. She took an antacid, but it did not help. Her temperature is 37°C (98.6°F ), respirations are 16/min, pulse is 78/min, and blood pressure is 122/98 mm Hg. Physical examination is normal, and she says that her pain has subsided. The urgent care provider suspects she has cholecystitis, so she undergoes a limited abdominal ultrasound to confirm it. However, no evidence of cholecystitis is seen with ultrasound, but adenomyomatosis of the gallbladder is incidentally noted. The patient has no clinical features suspicious for malignancy. What is the next best step in the management of this patient?
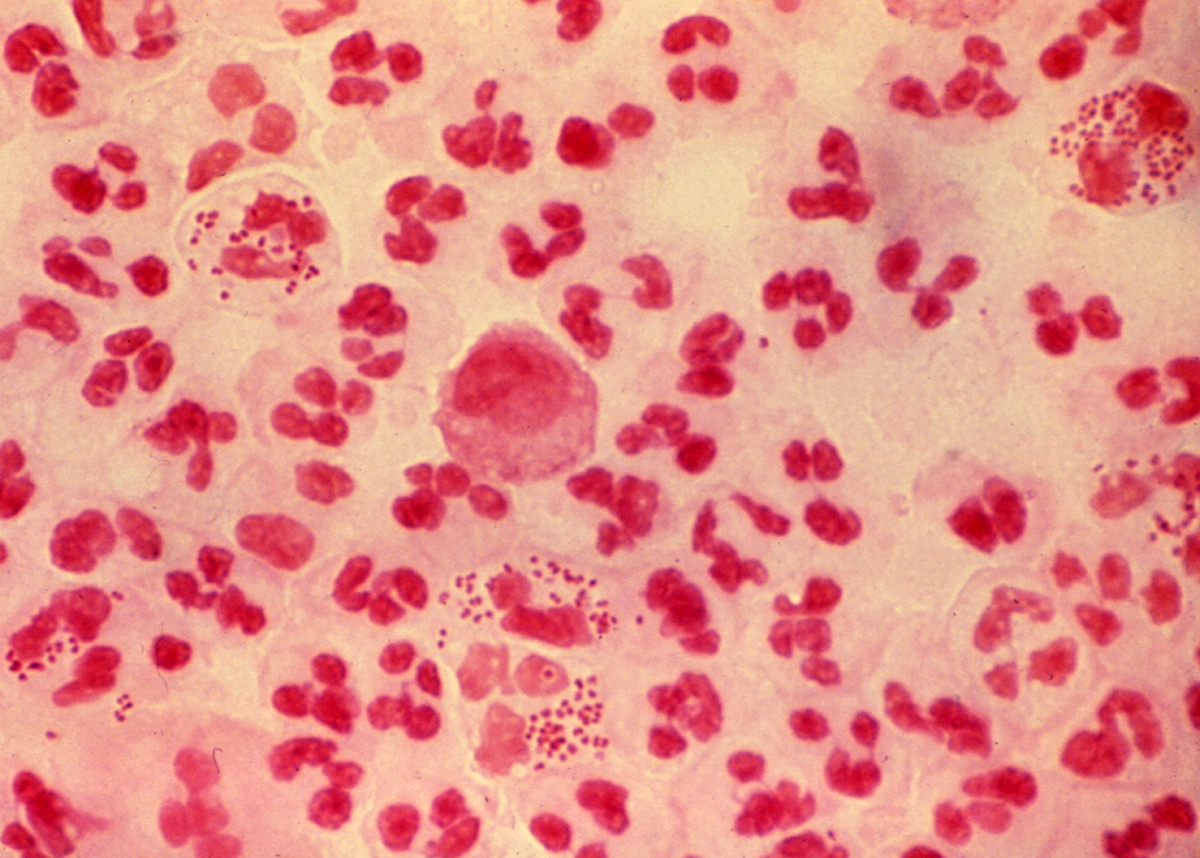
A 33-year-old man is brought to the emergency department by his partner for 24 hours of fever, severe headache, and neck stiffness. His companion also comments that he has been vomiting several times in the past 8 hours and looks confused. His personal medical history is unremarkable. Upon examination, his blood pressure is 125/82 mm Hg, heart rate 110/min, and temperature is 38.9 C (102F). There is no rash or any other skin lesions, his lung sounds are clear and symmetrical. There is nuchal rigidity, jolt accentuation of a headache, and photophobia. A lumbar puncture is taken, and cerebrospinal fluid is sent for analysis and a Gram stain (shown in the picture). The patient is put on empirical antimicrobial therapy with ceftriaxone and vancomycin. According to the clinical manifestations and Gram stain, which of the following should be considered in the management of this case?
A 48-year-old woman presents to the physician because of facial flushing and weakness for 3 months, abdominal discomfort and bloating for 6 months, and profuse watery diarrhea for 1 year. She reports that her diarrhea was episodic initially, but it has been continuous for the past 3 months. The frequency ranges from 10 to 12 bowel movements per day, and the diarrhea persists even if she is fasting. She describes the stools as odorless, watery in consistency, and tea-colored, without blood or mucus. She has not been diagnosed with any specific medical conditions, and there is no history of substance use. Her temperature is 36.9°C (98.4°F), heart rate is 88/min, respiratory rate is 18/min, and blood pressure is 110/74 mm Hg. Her physical exam shows decreased skin turgor, and the abdominal exam does not reveal any significant abnormality. Laboratory studies show: Serum glucose 216 mg/dL (12.0 mmol/L) Serum sodium 142 mEq/L (142 mmol/L) Serum potassium 3.1 mEq/L (3.1 mmol/L) Serum chloride 100 mEq/L (100 mmol/L) Serum calcium 11.1 mg/dL (2.77 mmol/L) Her 24-hour stool volume is 4 liters. Which of the following tests is most likely to yield an accurate diagnosis?
A 67-year-old man comes to the physician because of worsening lower back pain for 6 weeks. He reports that the pain is most intense with movement and that it sometimes occurs at night. Over the past 3 months, he has noticed a weakened urinary stream. He has not seen any blood in his urine. His only daily medication is ibuprofen. Examination shows no spinal deformities. Palpation of the lumbar spinal process elicits tenderness. Muscle strength is normal. Which of the following is the most likely cause of this patient’s back pain?
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app