
Gastroenterology — MCQs

On this page
A 74-year-old woman with a past medical history of hypertension, peripheral artery disease, and migraine headaches presents to the emergency department with a two hour history of severe abdominal pain. The patient cannot recall any similar episodes, although she notes occasional abdominal discomfort after eating. She describes the pain as sharp periumbilical pain. She denies recent illness, fever, chills, nausea, vomiting, or diarrhea. Her last normal bowel movement was yesterday evening. Her temperature is 37.1°C (98.8°F), pulse is 110/min, blood pressure is 140/80 mmHg, and respirations are 20/min. On exam, the patient is grimacing and appears to be in significant discomfort. Heart and lung exams are within normal limits. The patient's abdomen is soft and non-distended with diffuse periumbilical pain on palpation. There is no rebound tenderness or guarding, and bowel sounds are present. The rest of the exam is unremarkable. Labs in the emergency room show: Serum: Na+: 144 mEq/L Cl-: 105 mEq/L K+: 3.7 mEq/L HCO3-: 20 mEq/L BUN: 15 mg/dL Glucose: 99 mg/dL Creatinine: 1.2 mg/dL Ca2+: 10.7 mg/dL Phosphorus: 5.2 mg/dL Lactate: 7.0 mmol/L Amylase: 240 U/L Hemoglobin: 13.4 g/dL Hematocrit: 35% Leukocyte count: 12,100 cells/mm^3 with normal differential Platelet count: 405,000/mm^3 What is the next best step in diagnosis?
A 25-year-old man comes to the physician for a 2-month history of abdominal discomfort, fatigue, and increased urinary frequency, especially at night. He has also noticed that despite eating more often he has lost 14-lbs (6-kg). He has a congenital solitary kidney and a history of Hashimoto thyroiditis, for which he takes levothyroxine. He has smoked two packs of cigarettes daily for 10 years. BMI is 18 kg/m2. His temperature is 36.7°C (98.1°F), pulse is 80/min, and blood pressure is 110/60 mm Hg. Physical examination is unremarkable. Serum studies show an osmolality of 305 mOsm/L and bicarbonate of 17 mEq/L. Urinalysis shows clear-colored urine with no organisms. Which of the following is most likely to be helpful in establishing the diagnosis?
A 52-year-old male presents with several months of fatigue, malaise, dry cough, and occasional episodes of painless hematuria. He recalls having had a sore throat several days prior to the onset of these symptoms that resolved without antibiotics. Physical exam is remarkable for diffusely coarse breath sounds bilaterally. Urinalysis reveals 2+ protein, 2+ blood, and numerous red blood cell casts are visible under light microscopy. Which is the most likely diagnosis?
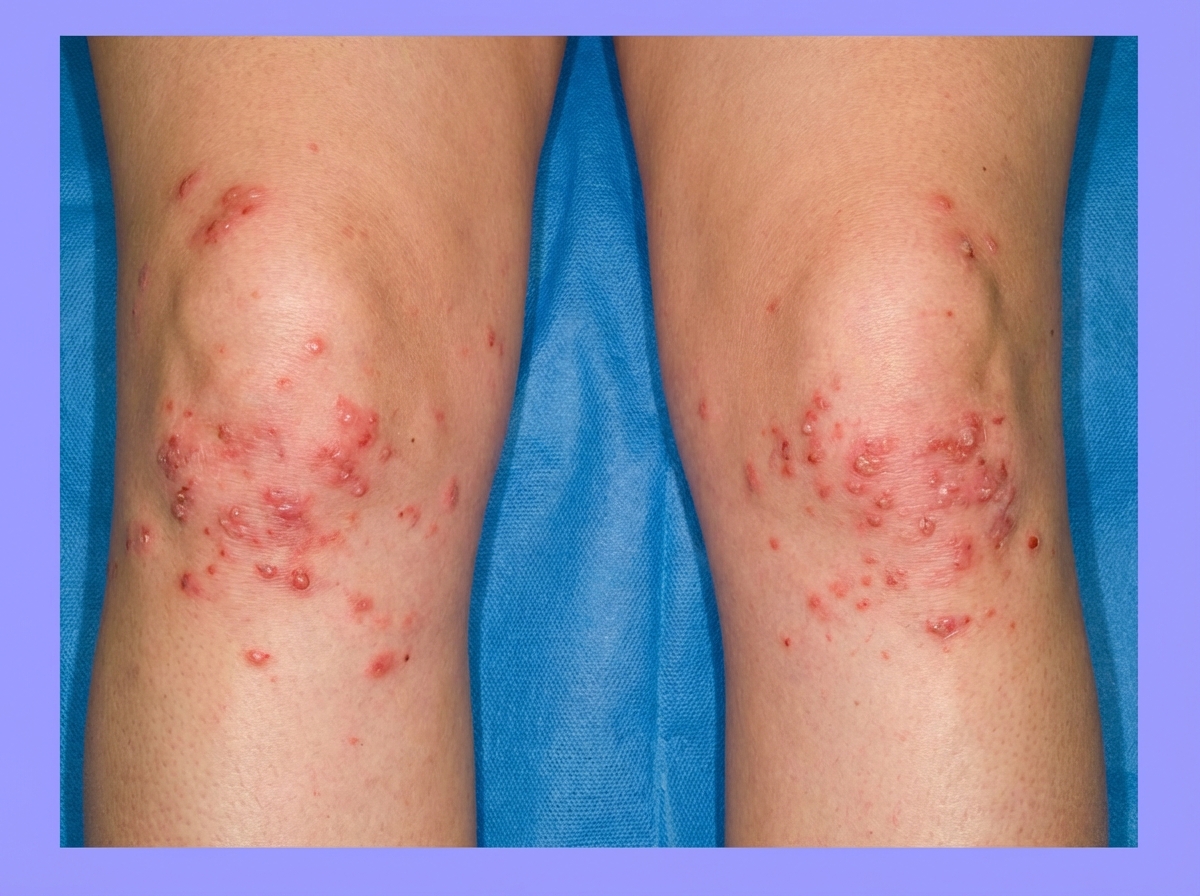
A 42-year-old woman presents with exertional dyspnea and fatigue for the past 3 months. Her past medical history is significant for multiple episodes of mild diarrhea for many years, which was earlier diagnosed as irritable bowel syndrome (IBS). She denies any current significant gastrointestinal symptoms. The patient is afebrile and vital signs are within normal limits. Physical examination reveals oral aphthous ulcers and mild conjunctival pallor. Abdominal examination is unremarkable. There is a rash present on the peripheral extremities bilaterally (see image). Laboratory findings are significant for evidence of microcytic hypochromic anemia. FOBT is negative. Which of the following is the most likely diagnosis in this patient?
A 45-year-old woman with type 2 diabetes mellitus is brought to the physician because of a 3-week history of nausea, abdominal pain, and confusion. She has a history of gastroesophageal reflux disease treated with over-the-counter antacids. She does not smoke or drink alcohol. Her only medication is metformin. Her pulse is 86/min and blood pressure is 142/85 mm Hg. Examination shows a soft abdomen. Arterial blood gas analysis on room air shows: pH 7.46 PCO2 44 mm Hg PO2 94 mm Hg HCO3- 30 mEq/L An ECG shows a QT interval corrected for heart rate (QTc) of 0.36 seconds (N = 0.40–0.44). The serum concentration of which of the following substances is most likely to be increased in this patient?
A previously healthy 31-year-old man comes to the emergency department because of acute onset of left flank pain radiating to his inner groin and scrotum for 3 hours. He also had nausea and one episode of hematuria. His only medication is a multivitamin. He appears uncomfortable. His temperature is 37°C (98.6°F), pulse is 104/min, respirations are 19/min, and blood pressure is 132/85 mm Hg. Physical examination shows marked tenderness in the left costovertebral area. He has normal skin turgor, a capillary refill time of < 1 second, and has been urinating normally. Laboratory studies show: Serum Calcium 9.5 mg/dL Phosphorus 4.3 mg/dL Creatinine 0.8 mg/dL Urea nitrogen 15 mg/dL Urine pH 6.5 RBCs 50–60/hpf A CT scan of the abdomen shows a 4-mm stone in the left distal ureter. Intravenous fluid resuscitation is begun and treatment with tamsulosin and ketorolac is initiated. Five hours later, he passes the stone. Metabolic analysis of the stone is most likely going to show which of the following?
A 67-year-old man presents to his primary care provider for routine follow-up. He complains of mild fatigue and occasional tingling in both feet. He reports that this numbness and tingling has led to him having 3 falls over the last month. He has had type 2 diabetes mellitus for 23 years and hypertension for 15 years, for which he takes metformin and enalapril. He denies tobacco or alcohol use. His blood pressure is 126/82 mm Hg, the heart rate is 78/min, and the respiratory rate is 15/min. Significant laboratory results are shown: Hemoglobin 10 g/dL Hematocrit 30% Mean corpuscular volume (MCV) 110 fL Serum B12 level 210 picograms/mL Which of the following is the best next step in the management of this patient’s condition?
A 50-year-old man presents to the emergency department with chief complaints of abdominal pain, distension, and bloody diarrhea for a day. Abdominal pain was episodic in nature and limited to the left lower quadrant. It was also associated with nausea and vomiting. He also has a history of postprandial abdominal pain for several months. He had an acute myocardial infarction which was treated with thrombolytics 3 months ago. He is a chronic smoker and has been diagnosed with diabetes mellitus for 10 years. On physical examination, the patient is ill-looking with a blood pressure of 90/60 mm Hg, pulse 100/min, respiratory rate of 22/min, temperature of 38.0°C (100.5°F) with oxygen saturation of 98% in room air. The abdomen is tender on palpation and distended. Rectal examination demonstrates bright red color stool. Leukocyte count is 14,000/mm3. Other biochemical tests were within normal ranges. Abdominal X-ray did not detect pneumoperitoneum or air-fluid level. The recent use of antibiotics was denied by the patient and stool culture was negative for C. difficile. Contrast-enhanced CT scan revealed segmental colitis involving the distal transverse colon. What is the most likely cause of the patient’s symptoms?
A 39-year-old woman comes to the physician because of recurrent episodes of severe pain over her neck, back, and shoulders for the past year. The pain worsens with exercise and lack of sleep. Use of over-the-counter analgesics have not resolved her symptoms. She also has stiffness of the shoulders and knees and tingling in her upper extremities that is worse in the morning. She takes escitalopram for generalized anxiety disorder. She also has tension headaches several times a month. Her maternal uncle has ankylosing spondylitis. Examination shows marked tenderness over the posterior neck, bilateral mid trapezius, and medial aspect of the left knee. Muscle strength is normal. Laboratory studies, including a complete blood count, erythrocyte sedimentation rate, and thyroid-stimulating hormone are within the reference ranges. X-rays of her cervical and lumbar spine show no abnormalities. Which of the following is the most likely diagnosis?
A 68-year-old man presents to his primary care physician for fatigue. He is accompanied by his granddaughter who is worried that the patient is depressed. She states that over the past 2 months he has lost 15 lbs. He has not come to some family events because he complains of being “too tired.” The patient states that he tries to keep up with things he likes to do like biking and bowling with his friends but just tires too easily. He does not feel like he has trouble sleeping. He does agree that he has lost weight due to a decreased appetite. The patient has coronary artery disease and osteoarthritis. He has not been to a doctor in “years” and takes no medications, except acetaminophen as needed. Physical examination is notable for hepatomegaly. Routine labs are obtained, as shown below: Leukocyte count: 11,000/mm^3 Hemoglobin: 9 g/dL Platelet count: 300,000/mm^3 Mean corpuscular volume (MCV): 75 µm^3 Serum iron: 35 mcg/dL An abdominal ultrasound reveals multiple, hypoechoic liver lesions. Computed tomography of the abdomen confirms multiple, centrally-located, hypoattenuated lesions. Which of the following is the next best step in management?
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app