
Gastroenterology — MCQs

On this page
A 32-year-old woman complains of fatigue and pallor. She says symptoms that started several months ago and have been becoming more serious with time. She reports that she has been exercising regularly and has been adhering to a strict vegan diet. The patient has no significant past medical history and takes no current medications. She denies any smoking history, alcohol use, or recreational drug use. She is tachycardic, but otherwise, her physical examination is unremarkable. A complete blood count (CBC) shows anemia with a low MCV (mean corpuscular volume), and a peripheral blood smear shows small erythrocytes. Which of the following is the most likely diagnosis in this patient?
A 31-year-old man comes to the physician because of a 9-month history of increasing fatigue and recurrent nausea. During this period, he has had a 3.8 kg (8.3 lb) weight loss. He also reports feeling lightheaded when he stands up suddenly. He was diagnosed with alopecia areata 1 year ago and was treated with monthly intralesional triamcinolone injections for 3 months. He does not smoke or drink alcohol. His temperature is 37.4°C (99.3°F), pulse is 86/min, and blood pressure is 102/68 mm Hg. Examination of the scalp shows a few well-defined patches of hair loss without scarring. The creases of the palm are darkened. Serum studies show: Na+ 125 mEq/L Cl- 98 mEq/L K+ 5.6 mEq/L Glucose 72 mg/dL Creatinine 0.8 mg/dL Thyroid-stimulating hormone 4.1 μU/mL Cortisol (AM) 2.5 μg/dL Cortisol (30 min after 250 μg corticotropin) 2.6 μg/dL Which of the following is the most likely underlying mechanism of this patient's symptoms?
A 35-year-old woman comes to the physician with right-sided flank pain and blood in her urine for 1 day. She does not have fever or dysuria. She had similar symptoms several weeks ago but did not seek medical care at the time. Physical examination shows right costovertebral angle tenderness. Her serum uric acid level is 6.9 mg/dL. Urine dipstick shows 3+ blood. Analysis of a 24-hour urine collection specimen shows wedge-shaped prisms. This patient is most likely to benefit from which of the following to prevent recurrence of her condition?
A 70-year-old man with a history of chronic constipation presents to the emergency department with a two-day history of left lower quadrant abdominal pain. He is found to have a temperature of 100.8F, BP 140/90, HR 85, and RR 16. On physical examination, he is tender to light palpation in the left lower quadrant and exhibits voluntary guarding. Rectal examination reveals heme-positive stool. Laboratory values are unremarkable except for a WBC count of 12,500 with a left shift. Which of the following tests would be most useful in the diagnosis of this patient's disease?
A 56-year-old woman presents to the emergency department following a seizure episode. She has a remote history of tonic-clonic seizures; however, her seizures have been well-controlled on valproate, with no seizure episodes occurring over the past 12 years. She was weaned off of the valproate 4 months ago. Her temperature is 97.6°F (36.4°C), blood pressure is 122/80 mmHg, pulse is 85/min, respirations are 15/min, and oxygen saturation is 99% on room air. Examination reveals her to be lethargic and somewhat confused. She is moving all extremities spontaneously. Her mucous membranes appear moist and she does not demonstrate any skin tenting. Laboratory values are ordered as seen below. Arterial blood gas pH: 7.21 PO2: 99 mmHg PCO2: 20 mmHg HCO3-: 10 meq/L The patient's initial serum chemistries and CBC are otherwise unremarkable except for the bicarbonate as indicated above. An ECG demonstrates normal sinus rhythm. Which of the following is the best next step in management for this patient's acid-base status?
A 65-year-old man presents to the emergency department with vague, constant abdominal pain, and worsening shortness of breath for the past several hours. He has baseline shortness of breath and requires 2–3 pillows to sleep at night. He often wakes up because of shortness of breath. Past medical history includes congestive heart failure, diabetes, hypertension, and hyperlipidemia. He regularly takes lisinopril, metoprolol, atorvastatin, and metformin. His temperature is 37.0°C (98.6°F), respiratory rate 25/min, pulse 67/min, and blood pressure 98/82 mm Hg. On physical examination, he has bilateral crackles over both lung bases and a diffusely tender abdomen. His subjective complaint of abdominal pain is more severe than the observed tenderness on examination. Which of the following vessels is involved in the disease affecting this patient?
A patient presents with right upper quadrant pain, fever, and nonbloody vomiting. Which of the following risk factors is most likely associated with the patient's condition?
A 42-year-old man comes to his primary care physician complaining of abdominal pain. He describes intermittent, burning, epigastric pain over the past 4 months. He reports that the pain worsens following meals. He had an upper gastrointestinal endoscopy done 2 months ago that showed a gastric ulcer without evidence of malignancy. The patient was prescribed pantoprazole with minimal improvement in symptoms. He denies nausea, vomiting, diarrhea, or melena. The patient has no other medical problems. He had a total knee replacement 3 years ago following a motor vehicle accident for which he took naproxen for 2 months for pain management. He has smoked 1 pack per day since the age of 22 and drinks 1-2 beers several nights a week with dinner. He works as a truck driver, and his diet consists mostly of fast food. His family history is notable for hypertension in his paternal grandfather and coronary artery disease in his mother. On physical examination, the abdomen is soft, nondistended, and mildly tender in the mid-epigastric region. A stool test is positive for Helicobacter pylori antigen. In addition to antibiotic therapy, which of the following is the most likely to decrease the recurrence of the patient's symptoms?
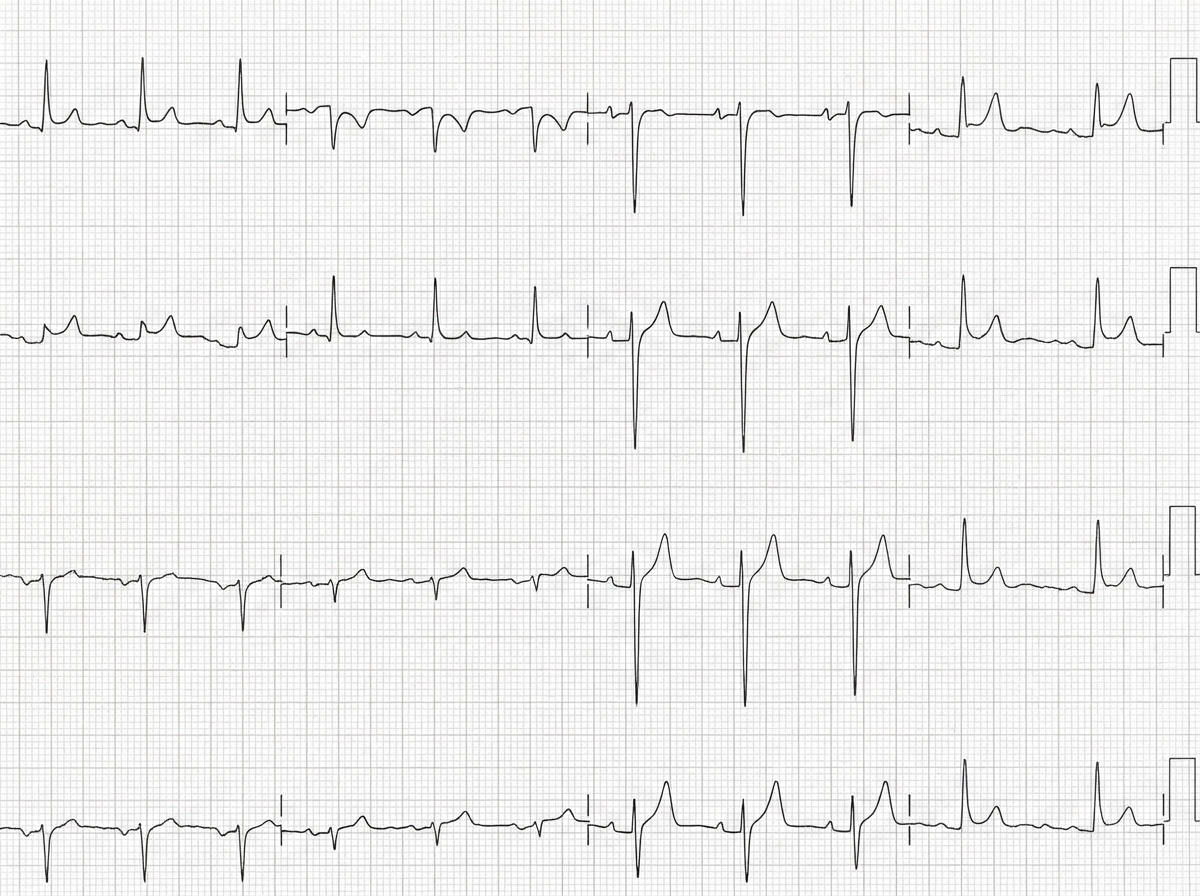
A 50-year-old man with a history of stage 4 kidney disease was admitted to the hospital for an elective hemicolectomy. His past medical history is significant for severe diverticulitis. After the procedure he becomes septic and was placed on broad spectrum antibiotics. On morning rounds, he appear weak and complains of fatigue and nausea. His words are soft and he has difficulty answering questions. His temperature is 38.9°C (102.1°F), heart rate is 110/min, respiratory rate is 15/min, blood pressure 90/65 mm Hg, and saturation is 89% on room air. On physical exam, his mental status appears altered. He has a bruise on his left arm that spontaneously appeared overnight. His cardiac exam is positive for a weak friction rub. Blood specimens are collected and sent for evaluation. An ECG is performed (see image). What therapy will this patient most likely receive next?
A 44-year-old man comes to the physician for a pre-employment evaluation. On questioning, he reports a mild cough, sore throat, and occasional headaches for 1 week. He has not had fever or weight loss. Nine years ago, he was diagnosed with HIV. He has gastroesophageal reflux disease. He has a history of IV drug abuse but quit 8 years ago. He has smoked one pack of cigarettes daily for 27 years and does not drink alcohol. Current medications include tenofovir, emtricitabine, efavirenz, and esomeprazole. He is 180 cm (5 ft 11 in) tall and weighs 89 kg (196 lbs); BMI is 27.5 kg/m2. His temperature is 37.3°C (99.1°F), pulse is 81/min, respirations are 17/min, and blood pressure is 145/75 mm Hg. Pulmonary examination shows no abnormalities. There are a few scattered old scars along the left elbow flexure. Laboratory studies show a leukocyte count of 6200/mm3, hemoglobin of 13.8 g/dL, and CD4+ count of 700/m3 (N = ≥ 500/mm3). A tuberculin skin test (TST) comes back after 50 hours with an induration of 3 mm in diameter. Which of the following is the most appropriate next step in management?
Practice by Chapter
GERD and esophageal disorders
Practice Questions
Peptic ulcer disease
Practice Questions
Helicobacter pylori infection
Practice Questions
Celiac disease
Practice Questions
Irritable bowel syndrome
Practice Questions
Diverticular disease
Practice Questions
GI bleeding (upper and lower)
Practice Questions
Small intestinal bacterial overgrowth
Practice Questions
Malabsorption syndromes
Practice Questions
Colorectal cancer screening
Practice Questions
Functional GI disorders
Practice Questions
Anorectal disorders
Practice Questions
GI motility disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app