
ACS — MCQs

On this page
A 67-year-old man comes to the emergency department because of retrosternal chest pressure and shortness of breath for 4 hours. The symptoms started while he was walking to work and have only minimally improved with rest. He has a history of type 2 diabetes mellitus. He has smoked one pack of cigarettes daily for 35 years. He appears uncomfortable. His pulse is 95/min. Serum studies show a normal troponin concentration. An ECG shows no abnormalities. Which of the following is the most likely underlying cause of this patient's symptoms?
A 67-year-old man presents to the emergency department with a 1-hour history of nausea and upper abdominal and substernal chest pain radiating to his lower jaw. He vomited several times before arriving at the hospital. His last visit to the primary care physician was 6 months ago during which he complained of fatigue, ‘slowing down’ on his morning walks, and abdominal pain that exacerbated by eating spicy food. His current medications include atorvastatin, metformin, insulin, omeprazole, aspirin, enalapril, nitroglycerin, and metoprolol. Today, his blood pressure is 95/72 mm Hg in his right arm and 94/73 in his left arm, heart rate is 110/min, temperature is 37.6°C (99.6°F), and respiratory rate is 30/min. On physical examination, he is diaphoretic and his skin is cool and clammy. His cardiac enzymes were elevated. He is treated appropriately and is admitted to the hospital. On day 5 of his hospital stay, he suddenly develops breathlessness. His blood pressure drops to 80/42 mm Hg. On examination, bibasilar crackles are heard. Cardiac auscultatory reveals a high pitched holosystolic murmur over the apex. Which of the following most likely lead to the deterioration of this patient’s condition?
A 67-year-old man is brought to the emergency department because of the sudden onset of severe substernal chest pain at rest. He has a history of hypertension, type 2 diabetes mellitus, and alcohol use disorder. He is diaphoretic and appears anxious. The lungs are clear to auscultation. An ECG shows ST-segment elevations in leads I, aVL, V5, and V6. One hour later, he develops dyspnea and a productive cough with frothy sputum. Which of the following best describes the most likely underlying pathophysiology of this patient's dyspnea?
A 61-year-old man is brought to the emergency department by ambulance because of severe retrosternal chest pain and shortness of breath for 30 minutes. Paramedics report that an ECG recorded en route to the hospital showed ST-segment elevation in I, aVL, and the precordial leads. On arrival, the patient is unresponsive to painful stimuli. Examination shows neither respiration nor pulse. Despite appropriate lifesaving measures, he dies 10 minutes later. Which of the following is the most likely cause of death in this patient?
A 74-year-old woman is brought by ambulance to the emergency department and presents with a complaint of excruciating chest pain that started about 45 minutes ago. The patient was sitting in the garden when she 1st noticed the pain in the upper abdomen. The pain has persisted and now localizes underneath of the sternum and the left shoulder. Milk of magnesia and aspirin were tried with no relief. The patient had previous episodes of chest pain that were of lesser intensity and rarely lasted more than 10 minutes. She is diabetic and has been managed for hypertension and rheumatoid arthritis in the past. On examination, the patient is breathless and sweating profusely. The vital signs include blood pressure 140/90 mm Hg and heart rate 118/min. The electrocardiogram (ECG) shows Q waves in leads V2 and V3 and raised ST segments in leads V2, V3, V4, and V5. Laboratory studies (including cardiac enzymes at 6 hours after admission show: Hematocrit 45% Troponin T 1.5 ng/mL Troponin I 0.28 ng/mL Creatine kinase (CK)-MB 0.25 ng/mL The patient is admitted and started on analgesia and reperfusion therapy. She shows initial signs of recovery until the 6th day of hospitalization when she starts vomiting and complaining of dizziness. Physical examination findings at this time included heart rate 110/min, temperature 37.7°C (99.9°F), blood pressure 90/60 mm Hg. Jugular venous pressure is 8 cm. A harsh pansystolic murmur is present at the left lower sternal border. ECG shows sinus tachycardia and ST-segment elevation with terminal negative T waves. Laboratory studies show: Hematocrit 38% Troponin T 1.15ng/mL Troponin I 0.18 ng/mL CK-MB 0.10 ng/mL Which of the following best explains the patient's current clinical condition?
A 62-year-old man is brought to the emergency department because of right-sided weakness and subjective decreased sensation that started 30 minutes ago. The patient reports that his symptoms started to ease 5 minutes after onset and have now completely resolved. He has hypertension, hyperlipidemia, and type 2 diabetes mellitus. He has smoked one pack of cigarettes daily for 40 years. His current medications include lisinopril, metformin, and sitagliptin. He is 183 cm (6 ft 0 in) tall and weighs 105 kg (220 lb); BMI is 32 kg/m2. He appears well. His temperature is 36.5°C (97.7°F), pulse is 80/min, and blood pressure is 150/88 mm Hg. Neurological examination shows no abnormalities. Cardiac examination shows regular rate and rhythm and a left-sided carotid bruit. Complete blood count, serum glucose, and electrolytes are within the reference ranges. An ECG shows sinus rhythm and left axis deviation. A CT scan of the head without contrast shows no abnormalities. Carotid doppler ultrasound shows 45% stenosis in the left carotid artery and 15% stenosis in the right. Which of the following is the most appropriate next step in management?
A 53-year-old man with a past medical history significant for hyperlipidemia, hypertension, and hyperhomocysteinemia presents to the emergency department complaining of 10/10 crushing, left-sided chest pain radiating down his left arm and up his neck into the left side of his jaw. His ECG shows ST-segment elevation in leads V2-V4. He is taken to the cardiac catheterization laboratory for successful balloon angioplasty and stenting of a complete blockage in his left anterior descending coronary artery. Echocardiogram the following day shows decreased left ventricular function and regional wall motion abnormalities. A follow-up echocardiogram 14 days later shows a normal ejection fraction and no regional wall motion abnormalities. This post-infarct course illustrates which of the following concepts?
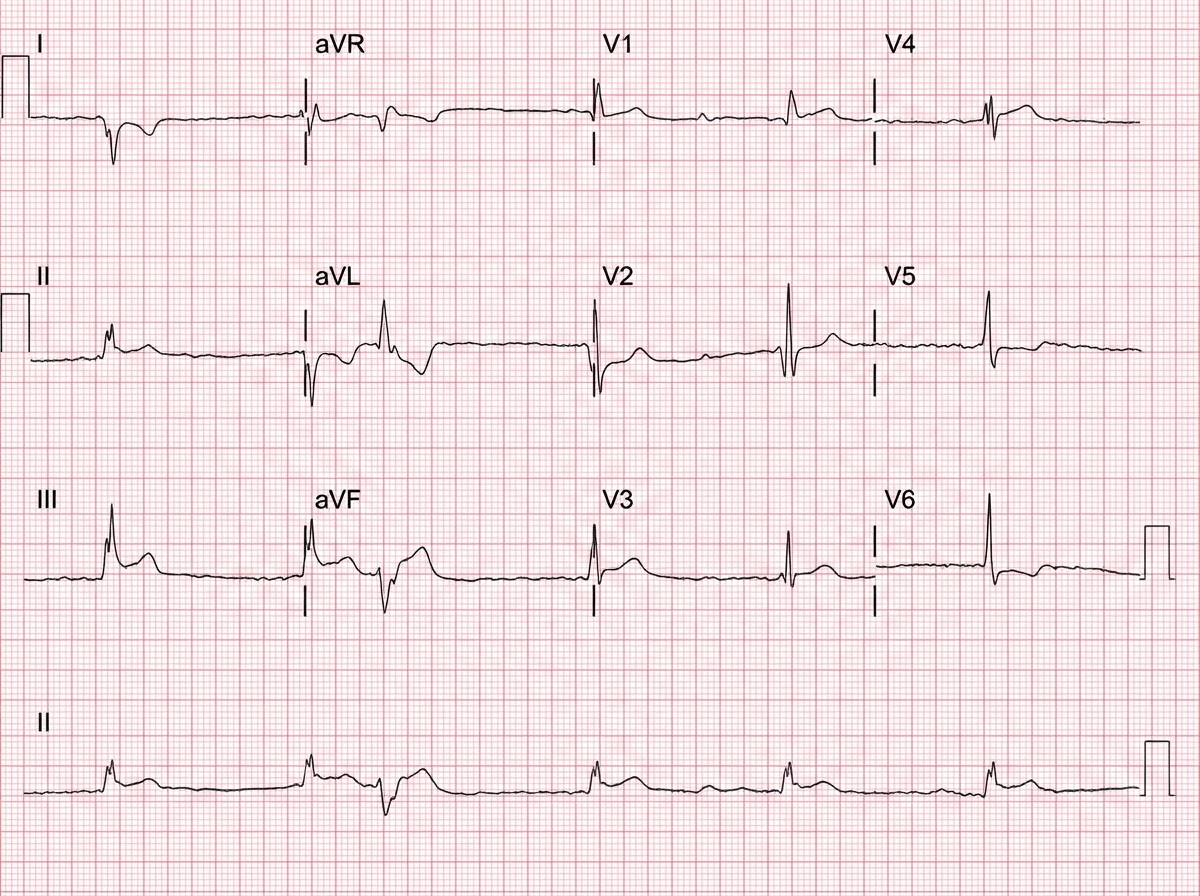
A 49-year-old man was brought to the emergency department by ambulance with complaints of sudden-onset chest pain that radiates into his neck and down his left arm. This substernal pain started 2 hours ago while he was having dinner. His past medical history is remarkable for hypercholesterolemia that is responsive to therapy with statins and coronary artery disease. His temperature is 37.0°C (98.6°F), blood pressure is 155/90 mm Hg, pulse is 112/min, and respiratory rate is 25/min. Troponin I levels are elevated. A 12-lead ECG was performed (see image). What is the most likely etiology of this patient’s presentation?
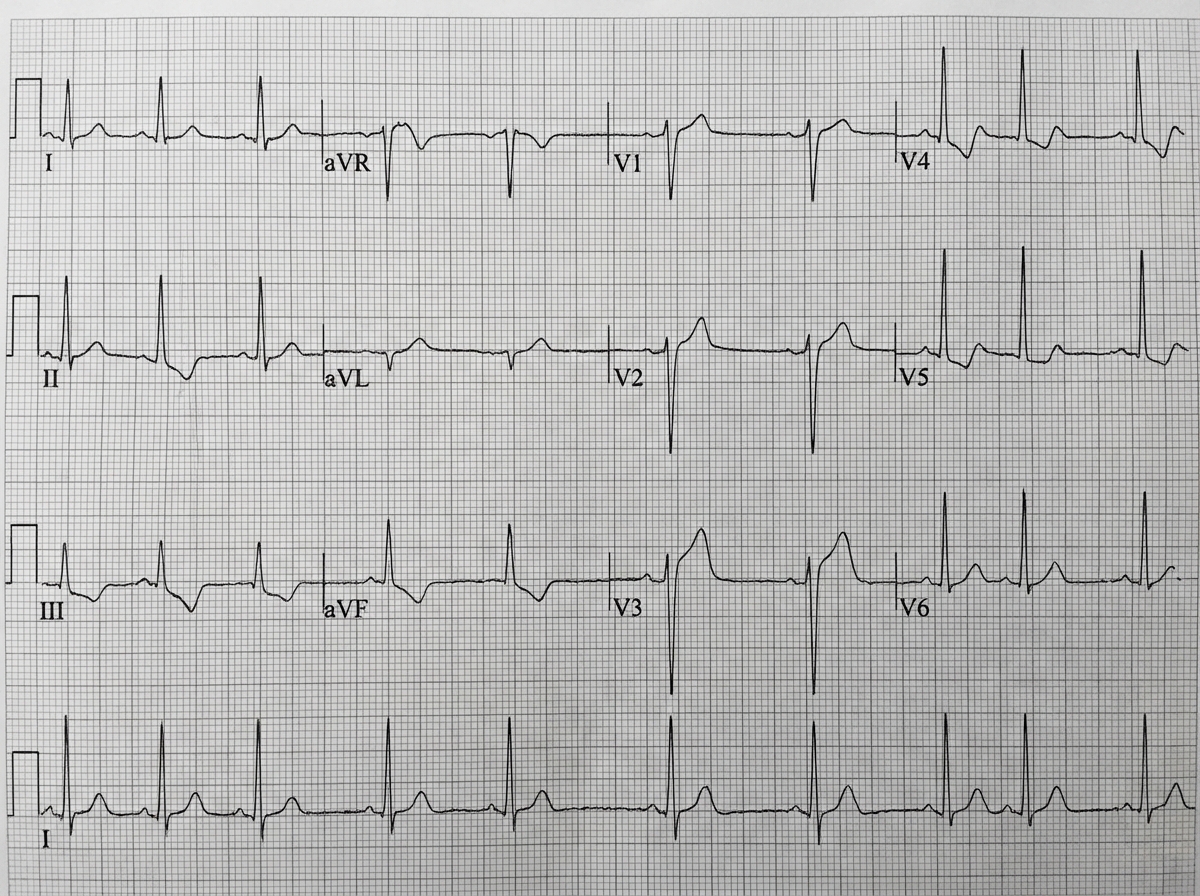
A 71-year-old man develops worsening chest pressure while shoveling snow in the morning. He tells his wife that he has a squeezing pain that is radiating to his jaw and left arm. His wife calls for an ambulance. On the way, he received chewable aspirin and 3 doses of sublingual nitroglycerin with little relief of pain. He has borderline diabetes and essential hypertension. He has smoked 15–20 cigarettes daily for the past 37 years. His blood pressure is 172/91 mm Hg, the heart rate is 111/min and the temperature is 36.7°C (98.0°F). On physical examination in the emergency department, he looks pale, very anxious and diaphoretic. His ECG is shown in the image. Troponin levels are elevated. Which of the following is the best next step in the management of this patient condition?
A 73-year-old man presents to the emergency department with acute substernal chest pain that began a few hours ago. The pain is described as a "pressure" that radiates to his left arm. His past medical history is significant for hypertension and hyperlipidemia. He is on chlorthalidone for his hypertension and simvastatin for hyperlipidemia. He has a 30 pack-year history of smoking and drinks 1-2 beers on weekends. His EKG shows ST depressions in the anterior precordial leads and he is given the proper medications and sent for emergency revascularization. Seven days later, he develops dyspnea that worsens in the supine position. Bibasilar crackles are heard on pulmonary auscultation. Cardiac exam reveals a new 3/6 holosystolic murmur best heard at the apex with radiation to the axilla. What is the most likely etiology of this patient's new symptoms?
Practice by Chapter
ACS pathophysiology and classification
Practice Questions
STEMI diagnosis and management
Practice Questions
NSTEMI diagnosis and management
Practice Questions
Unstable angina
Practice Questions
Cardiac biomarkers
Practice Questions
ECG interpretation in ACS
Practice Questions
Reperfusion strategies
Practice Questions
Antiplatelet therapy
Practice Questions
Anticoagulation in ACS
Practice Questions
Complications of MI
Practice Questions
Secondary prevention
Practice Questions
Special populations (elderly, renal dysfunction)
Practice Questions
Risk stratification in ACS
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app