
Lipid metabolism — MCQs

On this page
Colipase is an enzyme found in secretions from which of the following? (Recent NEET Pattern 2018)
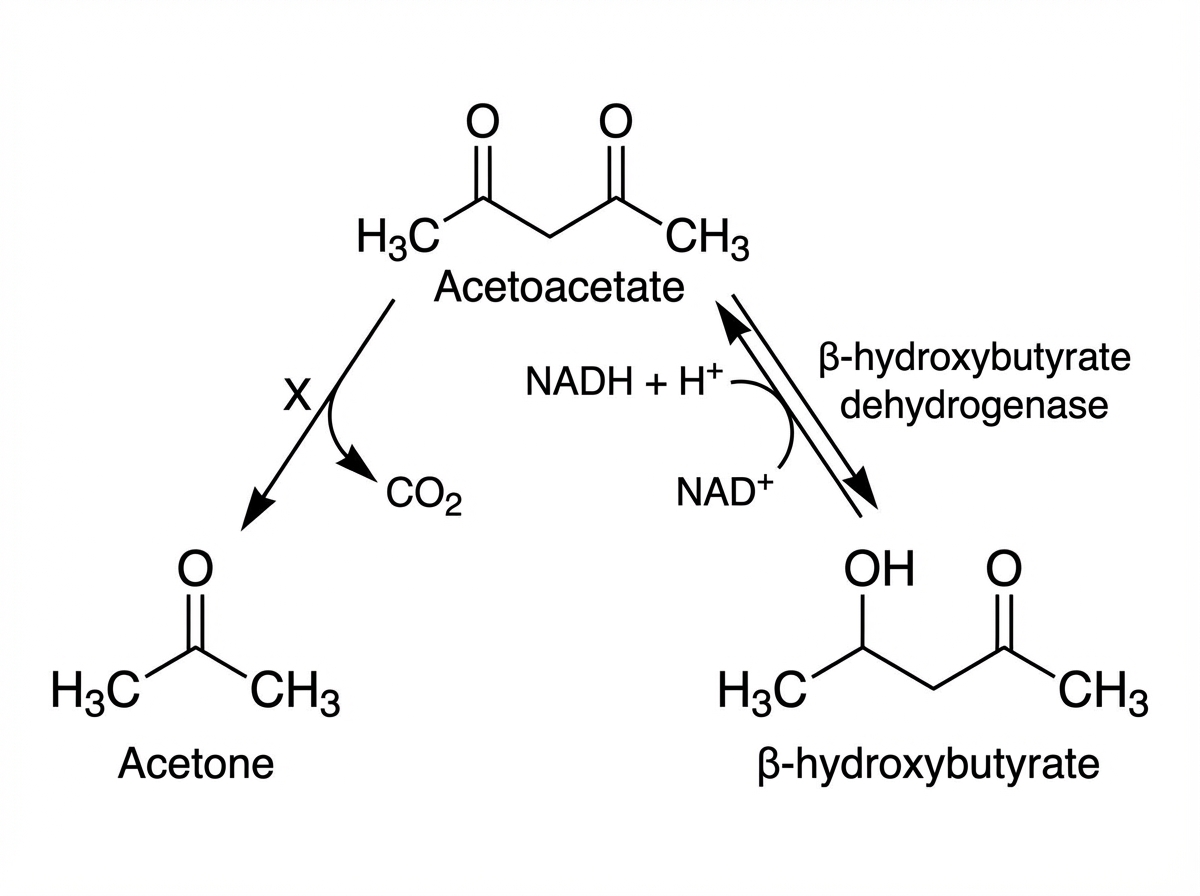
Name the mechanism shown as $X$ below.
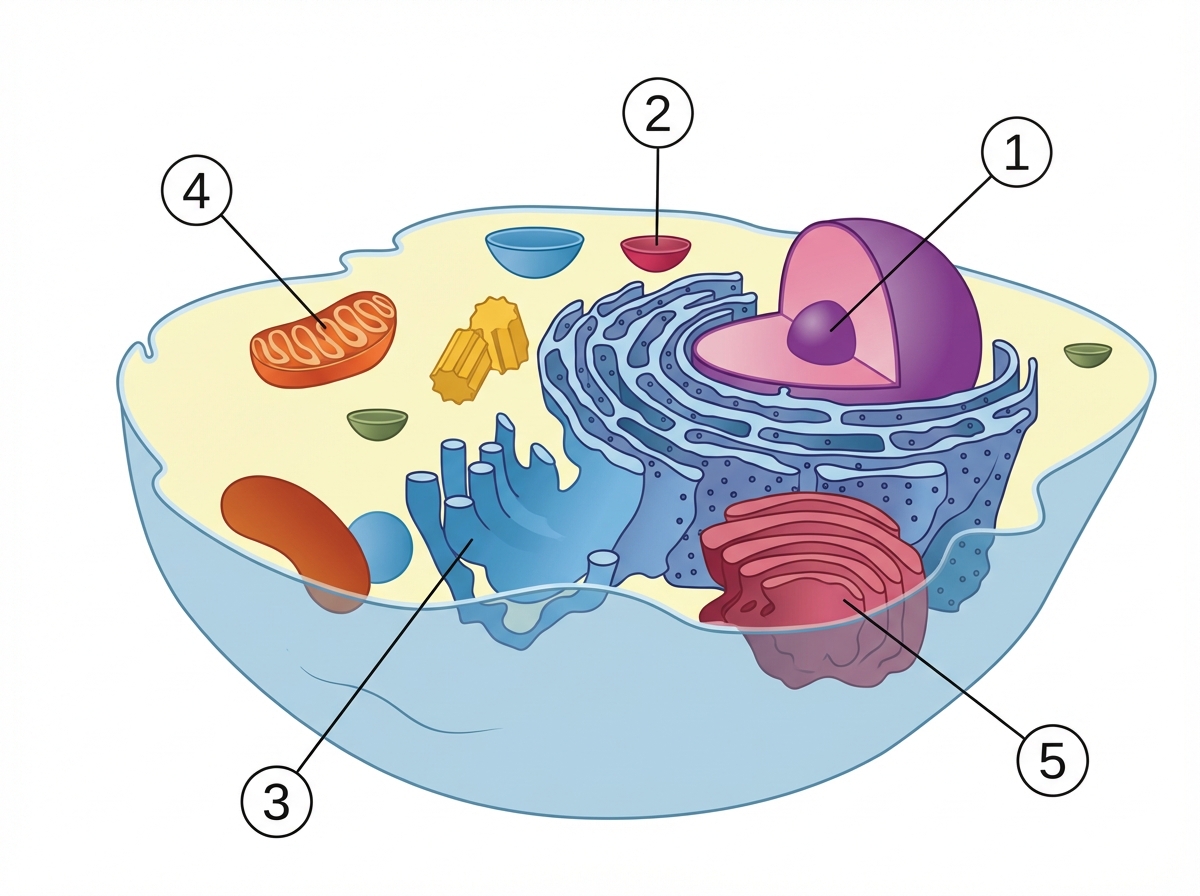
Which is the location of HMG CoA synthase in cholesterol metabolism?
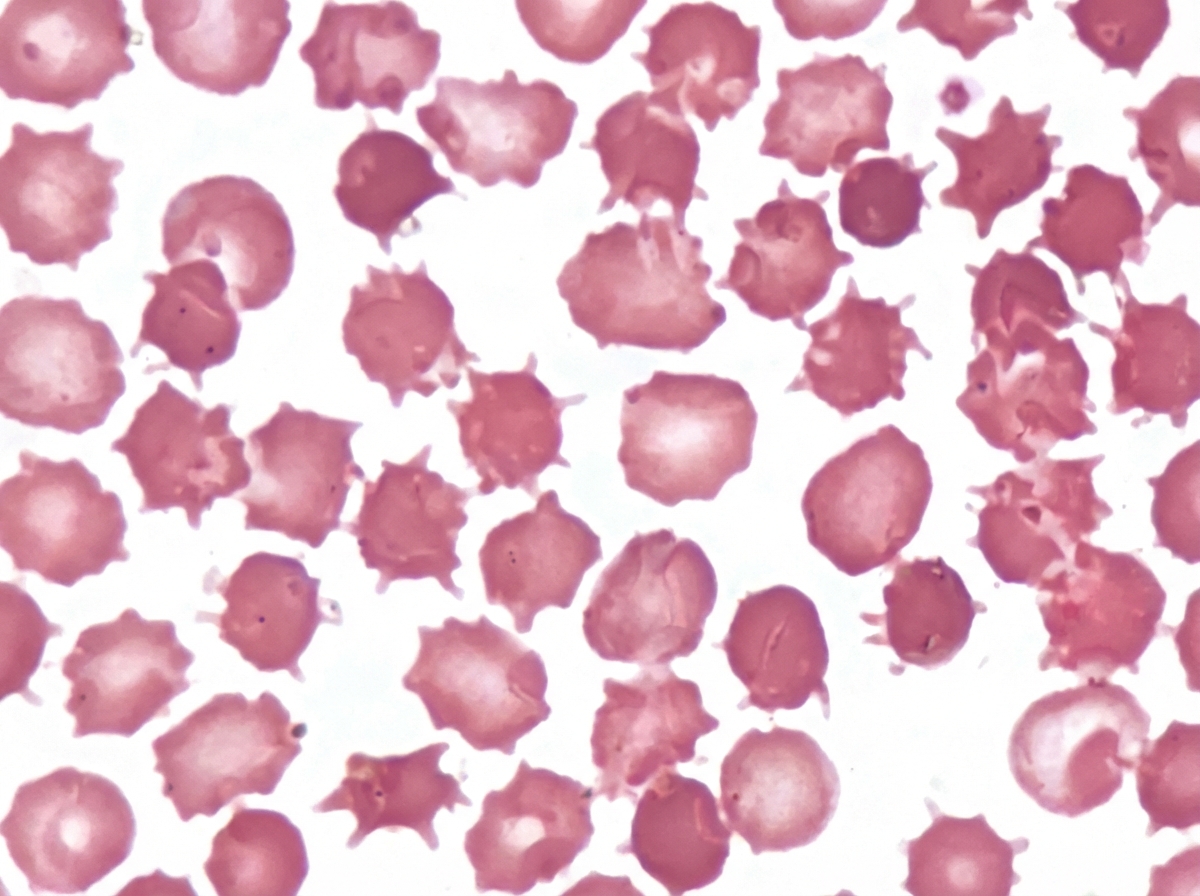
An adult male presented with a protruding abdomen, diarrhea, visual symptoms, and neurological manifestations. His LDL is low. Based on the peripheral smear finding shown in the image, what is the likely diagnosis?
A patient came to the hospital with severe abdominal pain, and lipase levels were elevated. On imaging, a stone is found in the common bile duct (CBD). Which enzyme is most likely elevated in this condition?
Lipid metabolism US Medical PG Practice Questions and MCQs
Question 1: Colipase is an enzyme found in secretions from which of the following? (Recent NEET Pattern 2018)
- A. Salivary glands
- B. Gallbladder
- C. Pancreas (Correct Answer)
- D. Small intestine
- E. Liver
Explanation: ***Pancreas*** - The pancreas is the primary source of **colipase** secretion in the digestive system. - Colipase is an essential co-factor for **pancreatic lipase**, helping it to anchor to the surface of **lipid droplets** and digest triglycerides in the presence of bile salts. - Colipase is secreted by pancreatic acinar cells along with other pancreatic enzymes into the duodenum. *Salivary glands* - The salivary glands (parotid, submandibular, sublingual) produce saliva containing enzymes like **amylase** and **lingual lipase**. - These glands do not secrete colipase, which is involved in fat digestion in the small intestine, not in the mouth. *Gallbladder* - The gallbladder stores and releases **bile**, which aids in fat emulsification. - Bile does not contain colipase; colipase is produced by the pancreas and works synergistically with bile salts during fat digestion. *Small intestine* - The small intestine is where most nutrient absorption occurs and produces some enzymes (e.g., brush border enzymes like maltase, lactase). - The small intestine does not synthesize colipase; it receives colipase from pancreatic secretions via the pancreatic duct. *Liver* - The liver produces bile, which is stored in the gallbladder and released into the duodenum to emulsify fats. - The liver does not produce colipase; this enzyme is specifically secreted by pancreatic acinar cells.
Question 2: Name the mechanism shown as $X$ below.
- A. Thiolase
- B. Nonenzymatic decarboxylation (Correct Answer)
- C. HMG CoA Lyase
- D. L-beta hydroxyl butyrate dehydrogenase
- E. HMG CoA synthase
Explanation: ***Nonenzymatic decarboxylation*** - The image shows **acetoacetate converting into acetone**, with the release of **carbon dioxide (CO2)**. This process is a spontaneous, **nonenzymatic decarboxylation** that occurs in conditions like diabetic ketoacidosis. - The absence of an enzyme indicated at "X" further supports that this is a **nonenzymatic reaction**. *Thiolase* - **Thiolase** is an enzyme involved in the synthesis of acetoacetyl CoA, and also in the breakdown of fatty acids, but not in the conversion of acetoacetate to acetone. - This enzyme catalyzes the **condensation of two acetyl-CoA** molecules to form acetoacetyl-CoA or the cleavage of acetoacetyl-CoA. *HMG CoA Lyase* - **HMG CoA lyase** is an enzyme that catalyzes the cleavage of HMG-CoA to **acetoacetate and acetyl-CoA** during ketogenesis. - It works upstream in the ketone body synthesis pathway, not directly converting acetoacetate to acetone. *HMG CoA synthase* - **HMG CoA synthase** is an enzyme that catalyzes the condensation of **acetoacetyl-CoA and acetyl-CoA** to form HMG-CoA, the first committed step of ketogenesis. - It works upstream in the pathway, not in the conversion of acetoacetate to acetone. *L-beta hydroxyl butyrate dehydrogenase* - The image already labels **beta-hydroxybutyrate dehydrogenase**, which interconverts **acetoacetate and beta-hydroxybutyrate** using NADH and NAD+. - This enzyme is responsible for the reversible reduction of acetoacetate to beta-hydroxybutyrate, and not for the formation of acetone.
Question 3: Which is the location of HMG CoA synthase in cholesterol metabolism?
- A. 1
- B. 2 (Correct Answer)
- C. 3
- D. 4
- E. 5
Explanation: ***2*** - HMG CoA synthase is a key enzyme in the cholesterol synthesis pathway, specifically converting acetoacetyl-CoA to **hydroxymethylglutaryl-CoA (HMG-CoA)**. - This step occurs in the **cytosol**, which is indicated by '2' in the diagram. - The cytosolic form of HMG-CoA synthase is specifically involved in cholesterol biosynthesis. *1* - '1' points to the **nucleus**, which is primarily involved in DNA replication and transcription, not cholesterol synthesis. - While gene expression control for cholesterol synthesis occurs here (e.g., SREBP regulation), the enzymatic reaction itself does not take place in the nucleus. *3* - '3' indicates the **smooth endoplasmic reticulum (SER)**, which is involved in later steps of cholesterol synthesis, such as the conversion of squalene to cholesterol. - However, the initial steps catalyzed by HMG CoA synthase occur in the cytosol, not directly on the SER. *4* - '4' points to a **mitochondrion**, which is involved in energy production through the citric acid cycle and oxidative phosphorylation. - Note: There is a mitochondrial HMG-CoA synthase, but it is involved in **ketone body synthesis**, not cholesterol metabolism. *5* - '5' represents another cellular structure not involved in the HMG-CoA synthase step of cholesterol synthesis. - The cholesterol synthesis pathway begins in the cytosol with the formation of HMG-CoA before proceeding to other compartments.
Question 4: An adult male presented with a protruding abdomen, diarrhea, visual symptoms, and neurological manifestations. His LDL is low. Based on the peripheral smear finding shown in the image, what is the likely diagnosis?
- A. Abetalipoproteinemia (Correct Answer)
- B. EDTA changes
- C. Uremia
- D. Burns
- E. Liver disease
Explanation: ***Abetalipoproteinemia*** - The image shows **acanthocytes (spur cells)**, characterized by irregularly spaced, blunt projections, which are a hallmark of **abetalipoproteinemia** due to abnormal lipid metabolism and membrane defects. - The clinical presentation of a **protruding abdomen (steatorrhea/malabsorption)**, **diarrhea**, **visual symptoms (retinopathy)**, **neurological manifestations (ataxia, peripheral neuropathy)**, and **low LDL** all strongly point to abetalipoproteinemia, a disorder affecting the synthesis of B-apolipoprotein and chylomicrons. *EDTA changes* - **EDTA changes** typically manifest as **rouleaux formation**, platelet satellite formation, or cell shrinkage, with red blood cell morphology generally remaining normal in terms of spur cell formation. - These changes are **artifactual** and are not associated with the patient's systemic symptoms like malabsorption, neurological issues, or specific lipid profile findings. *Uremia* - While **uremia** can cause various red blood cell abnormalities, including **burr cells (echinocytes)** with regularly spaced, pointed projections, it generally does not cause the irregularly shaped **acanthocytes** seen in the image. - The systemic symptoms of uremia would primarily involve **renal dysfunction (e.g., elevated BUN, creatinine)**, which are not mentioned, and not specifically the **visual or malabsorption symptoms** seen here. *Burns* - Severe **burns** can lead to red blood cell fragmentation, causing **schistocytes** or **microspherocytes** due to heat-induced damage. - Burns are not typically associated with the formation of **acanthocytes** or the constellation of symptoms (malabsorption, neurological, visual) and lipid profile (low LDL) described in this patient. *Liver disease* - Advanced **liver disease (cirrhosis)** can cause **spur cell anemia** with acanthocytes due to altered cholesterol-to-phospholipid ratio in RBC membranes. - However, the key distinguishing feature is the **low LDL** in this patient, which is characteristic of abetalipoproteinemia, whereas liver disease typically does not present with specifically **low LDL** as a prominent feature. - Additionally, the constellation of **visual symptoms (retinopathy)** and **neurological manifestations** with malabsorption are more consistent with the fat-soluble vitamin deficiency (A, E, K) seen in abetalipoproteinemia rather than isolated liver pathology.
Question 5: A patient came to the hospital with severe abdominal pain, and lipase levels were elevated. On imaging, a stone is found in the common bile duct (CBD). Which enzyme is most likely elevated in this condition?
- A. ALT
- B. GGT
- C. LDH
- D. AST
- E. ALP (Correct Answer)
Explanation: ***ALP (Alkaline Phosphatase)*** - **ALP** is the **most characteristic enzyme elevation** in **biliary obstruction** from a CBD stone. - ALP is found in high concentrations in the **bile duct epithelium** and hepatocytes adjacent to bile ducts, and rises dramatically with **cholestasis** and **obstructive jaundice**. - In CBD stone obstruction, ALP typically rises **3-10 times normal**, making it the hallmark biochemical marker of this condition. - While lipase is elevated due to associated pancreatitis, **ALP elevation specifically indicates the biliary obstruction**. *GGT (Gamma-Glutamyl Transferase)* - **GGT** is also elevated in **cholestasis** and **bile duct obstruction**. - GGT often rises in parallel with ALP and helps confirm the hepatobiliary origin of ALP elevation (vs. bone source). - However, **ALP is more specific** and typically shows greater magnitude of elevation in acute CBD obstruction, making it the **most likely** elevated enzyme in this clinical context. *ALT (Alanine Aminotransferase)* - **ALT** may be **mildly to moderately elevated** if there is secondary hepatocellular injury from biliary obstruction. - However, ALT primarily indicates **hepatocyte damage** rather than cholestasis, and its elevation is typically **less pronounced** than ALP in obstructive biliary disease. - The pattern in CBD obstruction is **cholestatic** (high ALP) rather than **hepatocellular** (high ALT). *AST (Aspartate Aminotransferase)* - **AST** can be elevated in various conditions including liver, heart, and muscle damage. - Like ALT, it may show mild elevation in biliary obstruction but is **not the primary marker**. - AST is less specific than ALP for diagnosing CBD stone obstruction. *LDH (Lactate Dehydrogenase)* - **LDH** is a **non-specific marker** of tissue damage found in multiple organs. - While it may be elevated, it provides little diagnostic value when specific markers like **ALP and lipase** are available. - LDH does not help differentiate biliary obstruction from other causes of abdominal pain.
Practice by Chapter
Fatty acid oxidation (beta-oxidation)
Practice Questions
Fatty acid synthesis
Practice Questions
Ketone body metabolism
Practice Questions
Cholesterol synthesis and regulation
Practice Questions
Lipoprotein metabolism
Practice Questions
Phospholipid metabolism
Practice Questions
Eicosanoid synthesis and function
Practice Questions
Steroid hormone synthesis
Practice Questions
Adipose tissue metabolism
Practice Questions
Brown vs. white adipose tissue
Practice Questions
Disorders of lipid metabolism
Practice Questions
Integration with carbohydrate metabolism
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Start For Free