
Trauma — MCQs

On this page
What is the typical color change observed in contusions as they progress over time?
A 5-year-old child falls and sustains a laceration to the forehead. Which of the following statements is true about lacerations?
A 45-year-old male presents with severe abdominal pain following a high-speed car accident. On examination, there is tenderness in the right upper quadrant and epigastrium with guarding. What is the most likely organ to be injured?
Which of the following is most commonly associated with full-thickness burns?
What is the best initial management for a burn patient with a suspected inhalation injury?
What does a bluish-purple discoloration behind the mastoid indicate?
A patient presents to the emergency department following blunt abdominal trauma with severe abdominal pain, a pulse of 112 beats per minute, and a systolic blood pressure of 80 mmHg. Based on ATLS principles, what is the immediate next step in management?
Estimate volume of Ringer lactate in first 8 hours for a 50 kg male with 40% TBSA second-degree burns?
What is the most common indication for performing a tracheostomy?
Most common organ injured in penetrating injury of the abdomen:
Trauma Indian Medical PG Practice Questions and MCQs
Question 1111: What is the typical color change observed in contusions as they progress over time?
- A. Yellow to green
- B. Red to blue
- C. Blue to green
- D. Red to yellow (Correct Answer)
Explanation: ***Red to yellow*** - Contusions typically start as **red to purplish-blue** due to deoxygenated hemoglobin in extravasated blood. - Over time, hemoglobin is broken down into **biliverdin (green)** and then **bilirubin (yellow)**. *Yellow to green* - This sequence is incorrect as **green (biliverdin)** usually precedes **yellow (bilirubin)** in the breakdown pathway of hemoglobin. - Yellow is generally the final stage before resolution, not an intermediate stage transitioning to green. *Red to blue* - While contusions start **red** and quickly turn **blue/purple** due to deoxygenated hemoglobin, this option only covers the initial phase. - It misses the subsequent color changes that occur as **hemoglobin** is metabolized. *Blue to green* - This sequence is partially correct but incomplete; blue/purple is an early color. - It omits the initial **red** phase and the final **yellow** resolution, which are important parts of the color progression.
Question 1112: A 5-year-old child falls and sustains a laceration to the forehead. Which of the following statements is true about lacerations?
- A. They are clean-cut wounds
- B. They do not bleed
- C. They have irregular margins (Correct Answer)
- D. They heal without scarring
Explanation: ***They have irregular margins*** - Lacerations are characterized by **torn, jagged, and irregular wound edges** due to the blunt force mechanism of injury. - This irregularity distinguishes them from **incised wounds**, which have clean, sharp margins. *They are clean-cut wounds* - This statement is incorrect because **lacerations** result from blunt trauma, causing the skin and underlying tissues to **tear irregularly**. - **Incised wounds**, not lacerations, are typically clean-cut and caused by sharp objects. *They do not bleed* - This is incorrect; lacerations often **bleed significantly** depending on the depth and location of the injury, as blood vessels are damaged. - The amount of bleeding can vary but is almost always present to some degree. *They heal without scarring* - This is incorrect; all but the most superficial lacerations will heal with **some degree of scarring**, especially if they are deep, wide, or become infected. - The extent of scarring depends on factors like wound depth, location, infection, and individual healing responses.
Question 1113: A 45-year-old male presents with severe abdominal pain following a high-speed car accident. On examination, there is tenderness in the right upper quadrant and epigastrium with guarding. What is the most likely organ to be injured?
- A. Spleen
- B. Stomach
- C. Pancreas
- D. Liver (Correct Answer)
Explanation: ***Liver*** - The **liver** is the most commonly injured solid organ in blunt abdominal trauma due to its large size and relatively fixed position against the posterior abdominal wall and ribs, making it susceptible to shear forces during deceleration injuries. - Liver injury typically presents with **right upper quadrant tenderness** which may extend to the epigastrium, along with guarding and signs of hemorrhage. - The clinical presentation of RUQ pain with guarding following high-speed deceleration injury is classic for hepatic trauma. *Spleen* - The **spleen** is the second most commonly injured solid organ in blunt abdominal trauma but typically presents with pain in the **left upper quadrant** and left shoulder (Kehr's sign due to diaphragmatic irritation). - While splenic injury is common, the right upper quadrant tenderness described here points away from this diagnosis. *Pancreas* - **Pancreatic injuries** are less common in blunt trauma (occurs in only 1-2% of cases) and usually result from direct epigastric blows over the vertebral column (handlebar injuries, seat belt injuries). - It typically presents with **delayed symptoms** including severe epigastric pain radiating to the back, elevated amylase/lipase, often hours after the incident. - The immediate presentation with RUQ tenderness is more consistent with liver injury. *Stomach* - **Stomach injuries** from blunt trauma are rare (less than 1% of cases) due to its mobile nature and protective location beneath the rib cage. - When injured, it causes chemical peritonitis from leakage of gastric contents, presenting with generalized peritonitis rather than localized RUQ/epigastric tenderness.
Question 1114: Which of the following is most commonly associated with full-thickness burns?
- A. Painless white or charred appearance (Correct Answer)
- B. Blister formation
- C. Severe pain
- D. Reddened, moist skin
Explanation: ***Painless white or charred appearance*** - Full-thickness burns destroy nerve endings, leading to a **loss of sensation** and therefore **painless** tissues. - The destruction of all skin layers results in a characteristic **white, leathery, or charred appearance**. *Blister formation* - Blister formation is primarily associated with **partial-thickness burns** (second-degree), where the epidermis and part of the dermis are damaged. - In full-thickness burns, the destruction is too deep to allow for blister formation at the surface. *Severe pain* - Severe pain is most characteristic of **superficial partial-thickness burns** (second-degree), where nerve endings are exposed but not destroyed. - Full-thickness burns involve the complete destruction of nerve endings in the affected area, leading to **absent or minimal pain** within the burned area itself, though surrounding partial-thickness areas may be painful. *Reddened, moist skin* - **Reddened, moist skin** is typical of **superficial burns** (first-degree) or **superficial partial-thickness burns** (second-degree). - These burns affect only the epidermis or superficial dermis, leaving the deeper structures intact and often producing a raw, weeping surface.
Question 1115: What is the best initial management for a burn patient with a suspected inhalation injury?
- A. Bronchoscopy
- B. Immediate intubation (Correct Answer)
- C. High-flow oxygen
- D. Intravenous fluid resuscitation
Explanation: ***Immediate intubation*** - **Early intubation** is the standard of care for burn patients with **suspected inhalation injury** because progressive airway edema develops over 12-24 hours following thermal injury. - The principle is **"intubate early or never"** - delaying intubation can make it technically impossible once significant edema develops, leading to emergent surgical airway. - **Indications for early intubation** include: facial/neck burns, singed nasal hairs, carbonaceous sputum, hoarseness, stridor, or respiratory distress. - **Airway takes priority** over all other interventions in the ABC (Airway-Breathing-Circulation) sequence. *High-flow oxygen* - While **high-flow oxygen** is important for treating potential **carbon monoxide poisoning**, it does not protect the airway from progressive edema. - Oxygen should be administered, but only after securing the airway in patients with suspected inhalation injury. - CO poisoning is treated with oxygen, but airway compromise is the immediate life threat. *Bronchoscopy* - **Bronchoscopy** is useful for diagnosing the extent of airway injury and can help guide management decisions. - However, it is not the initial priority - securing the airway comes first. - Bronchoscopy can be performed after intubation to assess injury severity. *Intravenous fluid resuscitation* - **Fluid resuscitation** using formulas like **Parkland formula** (4 mL/kg/%TBSA) is crucial for burn management to prevent hypovolemic shock. - However, in the ABC sequence, airway management precedes circulation management. - Fluids are started after ensuring airway patency and adequate oxygenation.
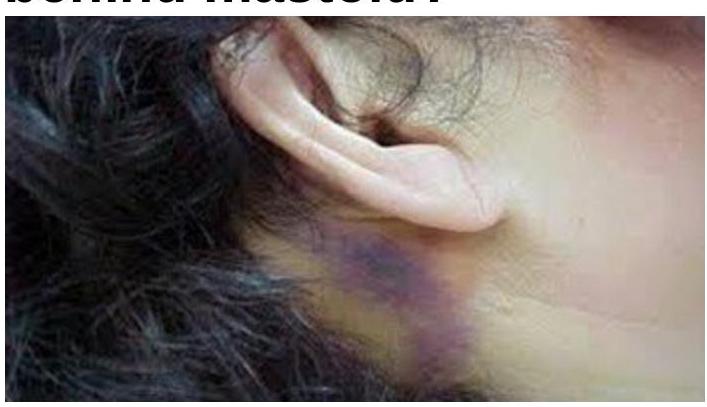
Question 1116: What does a bluish-purple discoloration behind the mastoid indicate?
- A. Battle sign (Correct Answer)
- B. Bezold abscess
- C. Both A and B
- D. None of the options
Explanation: ***Battle sign*** - A **bluish-purple discoloration behind the mastoid** (postauricular ecchymosis) is a classic sign of a **basilar skull fracture**, particularly involving the middle cranial fossa. - This bruising is caused by the extravasation of blood from the fracture site into the soft tissues over the mastoid process. *Bezold abscess* - A Bezold abscess is a rare complication of **mastoiditis**, where infection erodes through the mastoid tip and spreads to the soft tissues of the neck. - It presents as a **painful swelling in the neck** and is typically not associated with a bluish-purple discoloration *behind* the mastoid unless there is significant necrotic tissue or a secondary hematoma, which is not the primary feature. *Both A and B* - These conditions represent distinct pathologies, one related to **trauma (Battle sign)** and the other to **infection (Bezold abscess)**. - While both involve the mastoid region, their underlying causes and typical presentations are different. *None of the options* - The image directly displays the characteristic bruising of a Battle sign, making this option incorrect. - The appearance is highly indicative of a specific medical condition.
Question 1117: A patient presents to the emergency department following blunt abdominal trauma with severe abdominal pain, a pulse of 112 beats per minute, and a systolic blood pressure of 80 mmHg. Based on ATLS principles, what is the immediate next step in management?
- A. IV fluid resuscitation and stabilization (Correct Answer)
- B. Nasogastric decompression
- C. Exploratory laparotomy
- D. CT scan of abdomen
Explanation: ***IV fluid resuscitation and stabilization*** - The patient has **Class III hemorrhagic shock** (tachycardia 112 bpm, hypotension SBP 80 mmHg) following blunt abdominal trauma - Per **ATLS guidelines**, the priority is **"resuscitation before diagnosis"** - immediate aggressive IV fluid resuscitation with **2 large-bore IV lines** and **crystalloid boluses** - **Simultaneous actions** include: blood typing and crossmatch, FAST examination at bedside, and preparing the OR - The patient's **response to resuscitation** determines next steps: if remains unstable despite fluids → immediate laparotomy; if stabilizes → CT scan for further evaluation - **"No one goes to the OR dry"** - basic trauma principle requiring resuscitation initiation before definitive surgery *Exploratory laparotomy* - While likely needed given the unstable presentation, **immediate laparotomy without initiating resuscitation violates ATLS protocols** - The correct approach is **resuscitation WHILE preparing for surgery**, not delaying resuscitation until in the OR - Surgery is indicated for **persistent hemodynamic instability despite adequate resuscitation** or positive FAST with shock *CT scan of abdomen* - CT is **contraindicated in hemodynamically unstable patients** - correct assessment - This patient needs **bedside FAST examination** instead, which can be done during resuscitation - CT is reserved for **hemodynamically stable patients** after trauma *Nasogastric decompression* - Not a priority in acute trauma resuscitation - May be placed during resuscitation but does not address the **life-threatening hypovolemic shock** - Has no role in initial stabilization of hemorrhagic shock
Question 1118: Estimate volume of Ringer lactate in first 8 hours for a 50 kg male with 40% TBSA second-degree burns?
- A. 8 liters
- B. 4 liters (Correct Answer)
- C. 2 liters
- D. 6 liters
Explanation: **4 liters** - The Parkland formula is used for fluid resuscitation in burn patients: **4 mL x body weight (kg) x % TBSA burned**. - For a 50 kg male with 40% burns, the total fluid needed in the first 24 hours is 4 mL x 50 kg x 40% = **8000 mL (8 liters)**. Half of this volume is given in the first 8 hours, which is 8000 mL / 2 = **4000 mL (4 liters)**. *8 liters* - This volume represents the **total fluid requirement for the first 24 hours**, not just the first 8 hours. - The Parkland formula dictates that only half of the total 24-hour fluid volume is administered in the first 8 hours post-burn. *2 liters* - This amount is **insufficient** for adequate resuscitation of a patient with 40% total body surface area (TBSA) burns. - Administering only 2 liters would likely lead to **under-resuscitation and hypovolemic shock**. *6 liters* - This volume is **more than the recommended amount** for the first 8 hours but less than the total 24-hour requirement. - Over-resuscitation can lead to complications such as **compartment syndrome** and **pulmonary edema**.
Question 1119: What is the most common indication for performing a tracheostomy?
- A. Severe obstructive sleep apnea
- B. Tracheal stenosis
- C. Vocal cord paralysis
- D. Prolonged mechanical ventilation (Correct Answer)
Explanation: ***Prolonged mechanical ventilation*** - Maintaining an **endotracheal tube** for an extended period carries risks like **tracheal injury**, **vocal cord damage**, and difficulty with oral intake. - A tracheostomy provides a more comfortable and stable airway for **long-term respiratory support**, facilitates weaning from the ventilator, and reduces the risk of **ventilator-associated pneumonia**. *Severe obstructive sleep apnea* - While tracheostomy can effectively treat severe OSA by bypassing the upper airway obstruction, it is generally considered a **last resort** after less invasive treatments have failed. - The most common initial treatments for OSA include **CPAP**, weight loss, and oral appliances. *Tracheal stenosis* - Tracheal stenosis itself is a **structural narrowing** of the trachea that may or may not require tracheostomy, depending on its severity and location. - While a tracheostomy can bypass a severe stenosis, surgical repair of the trachea is often the definitive treatment for **severe tracheal stenosis**. *Vocal cord paralysis* - Unilateral vocal cord paralysis typically causes **hoarseness** and may not always necessitate a tracheostomy. - Bilateral vocal cord paralysis can lead to **airway obstruction**, but intervention usually involves vocal cord lateralization procedures or, in severe cases, a tracheostomy for airway patency.
Question 1120: Most common organ injured in penetrating injury of the abdomen:
- A. Liver
- B. Spleen
- C. Small bowel (Correct Answer)
- D. Colon
Explanation: ***Small bowel*** - The **small bowel** is the most frequently injured organ in penetrating abdominal trauma due to its extensive length and the large area it occupies within the abdominal cavity. - Its long, convoluted course makes it highly susceptible to being struck by projectiles or sharp objects traversing the abdomen. - Accounts for approximately **25-35%** of all penetrating abdominal injuries. *Liver* - The liver is commonly injured in both blunt and penetrating abdominal trauma, but it is the **second most frequent** organ injured in penetrating trauma. - Its large size and anterior position make it prone to injury, particularly in **gunshot wounds** or **stab wounds** to the upper abdomen. *Spleen* - The spleen is more frequently injured in **blunt abdominal trauma** rather than penetrating trauma. - While it can be injured by penetrating objects, its location in the left upper quadrant and protection by the rib cage makes it less exposed than the small bowel. *Colon* - The colon is the **third most commonly** injured organ in penetrating abdominal trauma. - Due to its fixed portions (ascending and descending colon) and large surface area, it is frequently encountered in penetrating injuries, but less so than the more mobile and extensive small bowel.
Practice by Chapter
Initial Assessment of Trauma Patient
Practice Questions
Advanced Trauma Life Support (ATLS) Principles
Practice Questions
Chest Trauma
Practice Questions
Abdominal Trauma
Practice Questions
Head Trauma
Practice Questions
Spinal Trauma
Practice Questions
Extremity Trauma
Practice Questions
Vascular Trauma
Practice Questions
Genitourinary Trauma
Practice Questions
Burns Management
Practice Questions
Mass Casualty Management
Practice Questions
Damage Control Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Start For Free