
Pediatric Radiology — MCQs

On this page
The "triangular cord sign" on ultrasonography is indicative of which condition in a neonate?
A neonate presented on day one of life with bilious vomiting. What is the first investigation to be done?
The lung-head ratio is useful in the diagnosis of which of the following conditions?
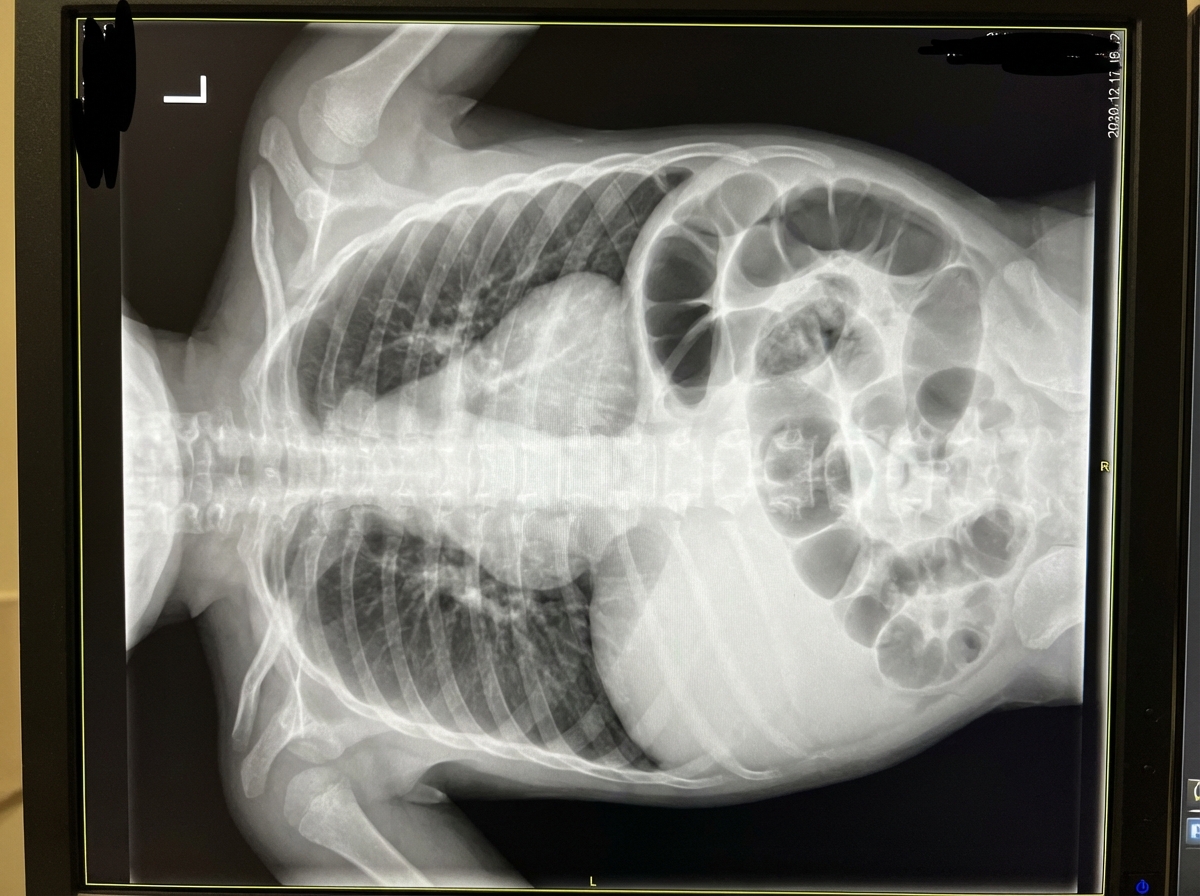
Given the provided X-ray of a neonate, what is the diagnosis?
Wimberger's ring is seen in:
Pediatric Radiology Indian Medical PG Practice Questions and MCQs
Question 1: The "triangular cord sign" on ultrasonography is indicative of which condition in a neonate?
- A. Galactosemia
- B. Biliary atresia (Correct Answer)
- C. Hepatitis
- D. None of the above
Explanation: **Explanation:** The **triangular cord sign** is a highly specific ultrasonographic finding for **Biliary Atresia (BA)**. It represents a cone-shaped or triangular fibrotic mass of the cranial part of the extrahepatic biliary tree. On ultrasound, it appears as an echogenic (hyperechoic) area located anterior to the bifurcation of the portal vein. A thickness of **>4 mm** is generally considered diagnostic. **Why Biliary Atresia is correct:** In BA, there is progressive fibro-obliterative destruction of the extrahepatic biliary system. The "triangular cord" is the sonographic visualization of this fibrous remnant at the porta hepatis. When combined with an absent or small, irregular gallbladder (ghost gallbladder sign), it is a pathognomonic finding. **Why other options are incorrect:** * **Galactosemia:** This is a metabolic disorder. While it can cause neonatal jaundice and hepatomegaly, it does not involve anatomical obliteration of the bile ducts; diagnosis is via enzyme assays and urine reducing sugars. * **Hepatitis (Neonatal):** This is the primary differential for BA. On ultrasound, neonatal hepatitis typically shows a patent biliary tree and a normal-sized gallbladder. It lacks the specific fibrous cord seen in BA. **High-Yield Clinical Pearls for NEET-PG:** * **Gold Standard Diagnosis:** Intraoperative Cholangiogram (IOCG). * **Best Initial Screening:** Ultrasound (looking for the triangular cord sign). * **Functional Imaging:** HIDA scan (shows uptake by the liver but **no excretion** into the bowel even after 24 hours). * **Surgical Management:** Kasai Procedure (Hepatoportoenterostomy), ideally performed before 60 days of life. * **Liver Biopsy:** Shows bile duct proliferation and portal fibrosis.
Question 2: A neonate presented on day one of life with bilious vomiting. What is the first investigation to be done?
- A. Chest skiagram
- B. Babygram (Correct Answer)
- C. Ultrasound
- D. Manometry
Explanation: **Explanation:** The clinical presentation of **bilious vomiting** in a neonate on the first day of life is a surgical emergency until proven otherwise. It indicates an intestinal obstruction distal to the Ampulla of Vater. **Why Babygram is the correct answer:** A **Babygram** (a single-view X-ray including both the chest and abdomen) is the initial screening investigation of choice. It is rapid, non-invasive, and provides immediate clues to the level of obstruction. Characteristic gas patterns on a babygram can diagnose conditions like: * **Double Bubble Sign:** Duodenal atresia. * **Triple Bubble Sign:** Jejunal atresia. * **Gasless Abdomen:** Suggestive of esophageal atresia without fistula or high-level obstruction. * **Pneumoperitoneum:** Indicating perforation. **Analysis of Incorrect Options:** * **Chest Skiagram (A):** While useful for respiratory distress or esophageal atresia, it does not provide sufficient information about the abdominal gas patterns necessary to evaluate bilious vomiting. * **Ultrasound (C):** Though excellent for diagnosing Pyloric Stenosis (which presents with *non-bilious* vomiting) or identifying the "whirlpool sign" in midgut volvulus, it is usually performed after the initial X-ray. * **Manometry (D):** This is used for functional disorders like Hirschsprung disease in older infants; it has no role in the acute emergency management of a neonate with bilious vomiting. **Clinical Pearls for NEET-PG:** * **Gold Standard for Malrotation/Volvulus:** Upper GI Contrast Study (showing "corkscrew" appearance). * **Most common cause of neonatal bowel obstruction:** Duodenal atresia (associated with Down Syndrome). * **Management Rule:** Any neonate with bilious vomiting requires an immediate X-ray to rule out life-threatening **Midgut Volvulus**.
Question 3: The lung-head ratio is useful in the diagnosis of which of the following conditions?
- A. Congenital diaphragmatic hernia (Correct Answer)
- B. Sequestration
- C. Ileal atresia
- D. Esophageal atresia
Explanation: **Explanation:** The **Lung-to-Head Ratio (LHR)** is a critical prenatal ultrasonographic parameter used primarily to assess the severity of pulmonary hypoplasia in fetuses with **Congenital Diaphragmatic Hernia (CDH)**. In CDH, abdominal viscera herniate into the thoracic cavity, compressing the developing lungs. The LHR is calculated by measuring the area of the contralateral (healthy) lung at the level of the four-chamber view of the heart and dividing it by the fetal head circumference. A lower LHR indicates more severe pulmonary hypoplasia and correlates with a poorer prognosis and higher need for postnatal ECMO (Extracorporeal Membrane Oxygenation). **Analysis of Incorrect Options:** * **Sequestration:** While this is a bronchopulmonary malformation, it is characterized by non-functional lung tissue with an anomalous systemic blood supply. Diagnosis is usually based on identifying the feeding systemic artery via Doppler, not LHR. * **Ileal Atresia:** This is a distal bowel obstruction. Antenatal ultrasound typically shows dilated bowel loops and polyhydramnios, but it does not involve lung measurement. * **Esophageal Atresia:** This is suggested prenatally by a "small or absent stomach bubble" and polyhydramnios. It does not directly impact lung volume in a way that requires LHR measurement. **High-Yield Clinical Pearls for NEET-PG:** * **Most common type of CDH:** Bochdalek hernia (Posterolateral, more common on the **Left** side). * **Morgagni Hernia:** Anterior/Retrosternal, usually occurs on the right side. * **Observed/Expected LHR (o/e LHR):** A more modern refinement of LHR that accounts for gestational age to better predict survival. * **Scaphoid abdomen:** A classic physical exam finding in newborns with CDH.
Question 4: Given the provided X-ray of a neonate, what is the diagnosis?
- A. Malrotation
- B. Congenital diaphragmatic hernia (Correct Answer)
- C. Pulmonary sequestration
- D. Pneumatoceles
Explanation: ***Congenital diaphragmatic hernia*** - Classic neonatal chest X-ray shows **bowel loops in the thoracic cavity** with **mediastinal shift** away from the affected side, typically left-sided. - Associated with **pulmonary hypoplasia** and immediate respiratory distress in newborns due to lung compression. *Malrotation* - Primarily an **abdominal condition** affecting bowel positioning around the **superior mesenteric artery**. - Chest X-ray would be normal; diagnosis requires **upper GI series** showing abnormal duodenal positioning. *Pulmonary sequestration* - Shows a **well-defined lung mass** with abnormal **systemic arterial supply** from the aorta. - Does not cause **bowel loops in chest** or immediate severe respiratory distress in neonates. *Pneumatoceles* - Appear as **thin-walled air-filled cysts** within the lung parenchyma, typically following pneumonia. - Do not show **bowel gas patterns** in the chest or cause mediastinal shift.
Question 5: Wimberger's ring is seen in:
- A. Rickets
- B. Scurvy (Correct Answer)
- C. Hemophilia
- D. Pellagra
Explanation: **Explanation:** **Wimberger’s ring sign** is a classic radiological feature of **Scurvy** (Vitamin C deficiency). In Scurvy, there is a failure of osteoid formation due to defective collagen synthesis, but osteoblastic activity continues to deposit calcium. This results in a thin, sclerotic (white) rim of calcification surrounding a central area of extreme radiolucency (rarefaction) in the epiphysis. **Why the other options are incorrect:** * **Rickets:** Characterized by Vitamin D deficiency leading to failure of mineralization of the osteoid. Key findings include cupping, fraying, and splaying of the metaphysis, and an increased "physeal" gap. * **Hemophilia:** Radiological findings typically involve joint destruction (hemophilic arthropathy), such as a widened intercondylar notch in the knee and squared lower pole of the patella. * **Pellagra:** A deficiency of Niacin (Vitamin B3) characterized by the "3 Ds" (Dermatitis, Diarrhea, Dementia). It does not have specific pathognomonic radiological bone signs. **High-Yield Clinical Pearls for Scurvy (NEET-PG):** 1. **Frankel’s Line:** Dense sclerotic line at the metaphysis (Zone of provisional calcification). 2. **Trummerfeld Zone:** A lucent (scorbutic) band proximal to Frankel’s line (site of microfractures). 3. **Pelkan Spur:** Marginal metaphyseal spurs caused by outward protrusion of the zone of provisional calcification. 4. **Subperiosteal Hemorrhage:** Leads to lifting of the periosteum, which becomes visible as it calcifies during healing.
Practice by Chapter
Normal Pediatric Developmental Anatomy
Practice Questions
Neonatal Imaging
Practice Questions
Pediatric Chest Imaging
Practice Questions
Pediatric Abdominal Imaging
Practice Questions
Pediatric Musculoskeletal Imaging
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital Heart Disease Imaging
Practice Questions
Pediatric Oncology Imaging
Practice Questions
Child Abuse Imaging
Practice Questions
Pediatric Interventional Radiology
Practice Questions
Radiation Protection in Pediatrics
Practice Questions
Sedation in Pediatric Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Start For Free