Which of the following conditions is the MOST COMMON cause of rib notching?
For pericardial calcifications, which is the best investigation?
Barium swallow is used for -
"String of beads" appearance on horizontal abdominal view X-ray is suggestive of:
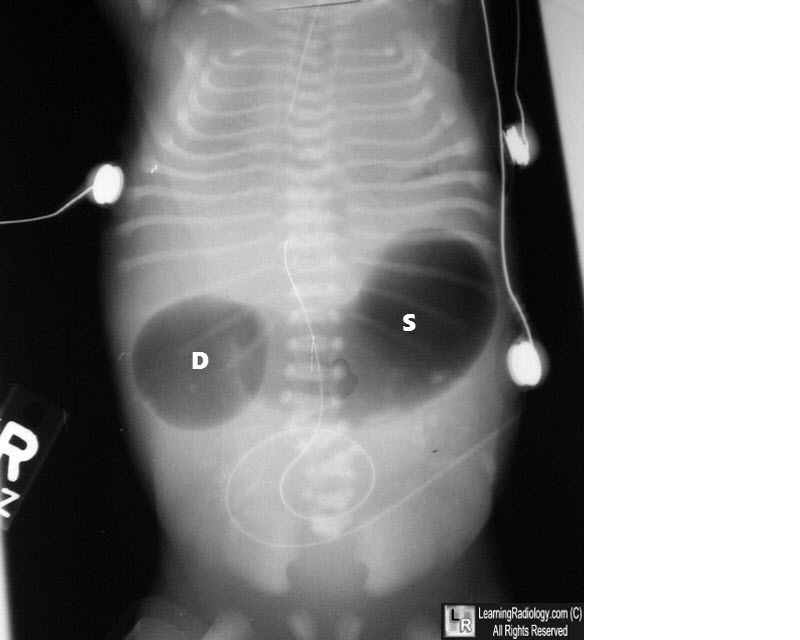
What condition is indicated by the double bubble sign on an abdominal X-ray?
Investigation with least radiation dose in the diagnosis of Meckel's diverticulum is -
What is the echogenic lesion size criterion for chronic pancreatitis?
What is the CT scan finding in a carotid cavernous sinus fistula?
On imaging, diffuse axonal injury is characterized by -
What is the investigation of choice for whole body imaging in metastatic breast cancer?
NEET-PG 2013 - Radiology NEET-PG Practice Questions and MCQs
Question 31: Which of the following conditions is the MOST COMMON cause of rib notching?
- A. Coarctation of aorta (Correct Answer)
- B. Atrial septal defect
- C. Chronic superior venacava obstruction
- D. Congenital interruption of aorta
Explanation: ***Coarctation of aorta*** - **Coarctation of the aorta** is the classic and **most common cause** of rib notching. - The notching is caused by the enlargement and tortuosity of the **intercostal arteries** as they provide collateral circulation to bypass the narrowed aorta. *Chronic superior venacava obstruction* - Chronic superior vena cava (SVC) obstruction may lead to the development of collateral circulation through the azygos and hemiazygos veins, but it does **not typically cause rib notching**. - Rib notching is specifically related to collateral flow bypassing an aortic obstruction, not a venous obstruction. *Atrial septal defect* - An **atrial septal defect (ASD)** is a communication between the atria that can lead to right heart volume overload and pulmonary hypertension. - While it's a congenital heart defect, an ASD does **not cause rib notching** as it does not involve an obstruction of systemic arterial flow requiring collateral circulation via the intercostal arteries. *Congenital interruption of aorta* - While **congenital interruption of the aorta** also involves an aortic obstruction, it is a **much rarer condition** than coarctation of the aorta. - Due to its rarity, it is not considered the most common cause of rib notching, even though it would theoretically lead to similar collateral vessel formation.
Question 32: For pericardial calcifications, which is the best investigation?
- A. Ultrasound
- B. CT scan (Correct Answer)
- C. MRI
- D. Transesophageal echocardiography
Explanation: ***Correct: CT scan*** - **CT scans** are highly sensitive and specific for detecting **pericardial calcifications** due to their excellent spatial resolution and ability to measure calcium density (Hounsfield units). - They provide detailed anatomical information about the **pericardium** and can accurately map the extent, location, and thickness of calcified areas. - **CT is the gold standard** for detecting and quantifying pericardial calcification, particularly in constrictive pericarditis. *Incorrect: Ultrasound* - While ultrasound (echocardiography) can visualize the pericardium and may detect calcifications, its ability to definitively identify and characterize **calcifications** is limited compared to CT. - **Acoustic shadowing** from calcifications can obscure underlying structures, making a precise assessment challenging. - Useful for detecting pericardial effusion and thickening, but not optimal for calcification assessment. *Incorrect: MRI* - **MRI excels** in visualizing soft tissues, pericardial inflammation, and fluid collections, but it is **poor at detecting calcium**. - Calcifications typically appear as signal voids (black) on MRI, making it difficult to differentiate them from other structures, air, or motion artifacts. - MRI is valuable for assessing pericardial inflammation and constriction but not the preferred method for calcification. *Incorrect: Transesophageal echocardiography* - TEE offers high-resolution images of cardiac structures and is primarily used for assessing valve function, intracardiac masses, endocarditis, and aortic pathology. - Its utility in detecting and characterizing **pericardial calcifications** is limited compared to CT, especially for diffuse or subtle calcifications. - The pericardium is not optimally visualized with TEE compared to transthoracic echocardiography.
Question 33: Barium swallow is used for -
- A. Colon
- B. Esophagus (Correct Answer)
- C. Duodenum
- D. Jejunum
Explanation: ***Esophagus*** - A **barium swallow** specifically visualizes the **esophagus**, pharynx, and sometimes the early stomach. - It's used to identify abnormalities like **dysphagia**, strictures, **achalasia**, or tumors by coating the mucosal lining. *Colon* - The colon is typically examined using a **barium enema**, where barium sulfate is administered rectally. - This procedure is effective for visualizing the large intestine for conditions like **polyps**, diverticula, or inflammatory bowel disease. *Duodenum* - While a barium swallow may transiently show the **duodenum**, its primary target is the esophagus and stomach. - More detailed imaging of the duodenum often requires an **upper GI series (UGI)**, which is a broader study of the upper digestive tract. *Jejunum* - The jejunum is part of the small intestine and is best visualized through a **small bowel follow-through (SBFT)** procedure. - This involves ingesting barium and taking serial X-rays as it progresses through the small bowel, to detect conditions like **Crohn's disease** or obstructions.
Question 34: "String of beads" appearance on horizontal abdominal view X-ray is suggestive of:
- A. Intussusception
- B. Sigmoid volvulus
- C. Small bowel obstruction (Correct Answer)
- D. Large bowel obstruction
Explanation: ***Small bowel obstruction*** - A "string of beads" appearance on a horizontal abdominal view X-ray refers to small gas bubbles trapped between the valvulae conniventes in a dilated small bowel loop. - This finding is highly suggestive of **complete small bowel obstruction**, particularly when accompanied by multiple air-fluid levels and dilated bowel loops. *Intussusception* - While it causes obstruction, intussusception usually appears as a **target sign** (doughnut sign) on ultrasound or a **meniscus sign** on barium enema, not a string of beads on plain X-ray. - Plain X-rays may show signs of **bowel obstruction**, but the string of beads is not characteristic. *Sigmoid volvulus* - Sigmoid volvulus is characterized by a **dilated loop of colon** forming an inverted U-shape, often described as a **coffee bean sign** or **omega sign**, on plain X-ray. - This involves the large bowel, and the "string of beads" specifically relates to gas in the small bowel. *Large bowel obstruction* - Large bowel obstruction typically presents with a **dilated colon** proximal to the obstruction and a collapsed distal colon, often with absent or minimal gas in the rectum and sigmoid. - While air-fluid levels can be present, the "string of beads" is a specific sign of gas within dilated small bowel loops, distinguishing it from most large bowel obstructions.
Question 35: What condition is indicated by the double bubble sign on an abdominal X-ray?
- A. Duodenal stenosis
- B. Volvulus
- C. All of the options
- D. Duodenal atresia (Correct Answer)
Explanation: ***Duodenal atresia*** - The **double bubble sign** on an abdominal X-ray is pathognomonic for **duodenal atresia**, characterized by two air-filled bubbles: one in the stomach and one in the proximal duodenum, separated by the pylorus. - This congenital anomaly results from a complete obstruction of the duodenum, preventing the passage of air and fluid past this point. *Duodenal stenosis* - While also an obstruction of the duodenum, **duodenal stenosis** is an incomplete obstruction, meaning some gas will pass beyond the duodenum. - This would result in gas being present in the distal bowel, which is not seen with a classic "double bubble" where the bowel distal to the duodenum is gasless. *Volvulus* - **Volvulus** involves the twisting of a loop of intestine, leading to obstruction and potentially ischemia. - While it can cause obstruction, it typically presents with a "corkscrew" appearance on an upper GI series or signs of diffuse bowel distension, not the isolated double bubble. *All of the options* - The double bubble sign is highly specific to **duodenal atresia** due to the complete obstruction it signifies. - Other conditions like duodenal stenosis and volvulus cause different radiological patterns, making this option incorrect.
Question 36: Investigation with least radiation dose in the diagnosis of Meckel's diverticulum is -
- A. MRI
- B. CT
- C. Contrast radiography
- D. Technetium -99m scanning (Correct Answer)
Explanation: ***Technetium-99m scanning*** - **Technetium-99m pertechnetate scan** (Meckel's scan) is the **gold standard investigation** for diagnosing Meckel's diverticulum with ectopic gastric mucosa - Among the investigations that can actually **diagnose Meckel's diverticulum**, it has the **lowest radiation dose** (approximately 1-2 mSv) - The radioisotope is specifically taken up by ectopic gastric mucosa, providing both diagnostic utility and relatively low radiation exposure - **Sensitivity: 85-95%** for detecting ectopic gastric mucosa in Meckel's diverticulum - The radiation dose is comparable to a few months of natural background radiation and significantly lower than CT or contrast studies *MRI* - While **MRI uses no ionizing radiation**, it is **not a standard or practical investigation** for diagnosing Meckel's diverticulum - MRI cannot identify ectopic gastric mucosa specifically - It is rarely used in clinical practice for this indication - The question asks about investigation "in the diagnosis" of Meckel's diverticulum, implying a test that is actually used diagnostically *CT* - **Computed Tomography (CT)** delivers a **high radiation dose** (typically 5-10 mSv or more) - While it can identify structural abnormalities, it is not specific for Meckel's diverticulum - Not the first-line investigation for this condition *Contrast radiography* - **Contrast studies** (barium studies) use **moderate ionizing radiation** (3-5 mSv) - Limited utility in diagnosing Meckel's diverticulum as it primarily assesses luminal patency - Cannot identify ectopic gastric mucosa - Lower sensitivity compared to Tc-99m scanning
Question 37: What is the echogenic lesion size criterion for chronic pancreatitis?
- A. > 2 mm
- B. > 3 mm (Correct Answer)
- C. > 1 mm
- D. > 4 mm
Explanation: ***> 3 mm*** - An echogenic lesion **greater than 3 mm** in size is a diagnostic criterion for **chronic pancreatitis** when observed on ultrasound imaging. - This represents one of the **major features** in ultrasound diagnosis of chronic pancreatitis, particularly when echogenic foci demonstrate acoustic shadowing (suggesting calcifications). - This criterion is part of established diagnostic frameworks and helps differentiate pathological calcifications from minor, non-specific findings. *> 4 mm* - While a **4 mm threshold** would indicate significant findings, the established diagnostic criterion for chronic pancreatitis uses **> 3 mm** as the cutoff. - Using a higher threshold would reduce sensitivity for detecting chronic pancreatitis. *> 2 mm* - A lesion larger than **2 mm** is generally considered below the established diagnostic threshold for **chronic pancreatitis**. - This size may represent early changes or incidental findings that are not yet definitive for diagnosis. *> 1 mm* - A lesion **greater than 1 mm** is too small to be a definitive criterion for **chronic pancreatitis** and could represent minor, non-pathological findings. - Such small echogenic foci lack sufficient specificity for diagnosing chronic pancreatic disease.
Question 38: What is the CT scan finding in a carotid cavernous sinus fistula?
- A. Enlarged superior ophthalmic vein (Correct Answer)
- B. Enlarged inferior ophthalmic vein
- C. Enlarged superior ophthalmic artery
- D. Enlarged inferior ophthalmic artery
Explanation: ***Enlarged superior ophthalmic vein*** * A carotid cavernous sinus fistula (CCSF) causes **high-pressure arterial blood** to shunt into the **venous system** of the cavernous sinus. * This increased pressure leads to retrograde flow and congestion in the draining veins, most notably the **superior ophthalmic vein**, causing its dilation. *Enlarged inferior ophthalmic vein* * While the inferior ophthalmic vein can also be involved in some cases of CCSF, the **superior ophthalmic vein** is typically more prominent and consistently affected due to its primary drainage pathway. * The inferior ophthalmic vein is less frequently the primary or most notable imaging finding compared to the superior ophthalmic vein. *Enlarged superior ophthalmic artery* * A CCSF involves an abnormal connection between the **carotid artery** (an artery) and the **cavernous sinus** (a venous structure), leading to venous, not arterial, dilation. * Arteries in the orbital region, like the superior ophthalmic artery, would not typically enlarge as a direct result of increased venous pressure in the cavernous sinus. *Enlarged inferior ophthalmic artery* * Similar to the superior ophthalmic artery, the inferior ophthalmic artery is an **arterial structure** and would not enlarge due to a high-flow arteriovenous shunt within the cavernous sinus. * The pathological changes in CCSF are primarily observed in the **venous drainage pathways**.
Question 39: On imaging, diffuse axonal injury is characterized by -
- A. Patchy ill-defined low density lesion mixed with small hyperdensities of petechial hemorrhage
- B. Crescentic extra-axial hematoma
- C. White matter lucencies
- D. Multiple small petechial hemorrhages (Correct Answer)
Explanation: ***Multiple small petechial hemorrhages*** - Diffuse axonal injury (DAI) is characterized on imaging by numerous **small petechial hemorrhages** at the **gray-white matter junction**, **corpus callosum**, and **brainstem**. - These microhemorrhages are the **hallmark imaging finding** and are best visualized on MRI (GRE/SWI sequences), though they can be seen on CT as small hyperdensities. - This is the **most specific** and characteristic finding that defines DAI. *Patchy ill-defined low density lesion mixed with small hyperdensities of petechial hemorrhage* - While this description can be seen in DAI (combining edema with microhemorrhages), it is **less specific** and could represent other entities. - This mixed pattern is more commonly associated with **contusions** where there is more prominent parenchymal injury with larger areas of edema and hemorrhage. - DAI classically shows predominantly **small punctate hemorrhages** rather than larger patchy low-density lesions. *Crescentic extra-axial hematoma* - A crescentic extra-axial collection describes a **subdural hematoma**, which is an entirely separate entity from DAI. - Subdural hematomas are located between the dura and arachnoid membranes, whereas DAI involves direct **axonal shearing injury** within brain parenchyma. *White matter lucencies* - This is a **non-specific finding** that can occur in many conditions including ischemia, demyelination, and chronic small vessel disease. - While DAI can cause white matter edema leading to lucencies, this does not capture the **characteristic petechial hemorrhages** that define the condition on imaging.
Question 40: What is the investigation of choice for whole body imaging in metastatic breast cancer?
- A. Angiography
- B. Venography
- C. Magnetic Resonance Imaging
- D. CT Scan (Correct Answer)
Explanation: ***CT Scan (Correct answer for NEET 2013)*** - **Contrast-enhanced CT scan** was the standard imaging modality for **whole-body staging** in metastatic breast cancer at the time of this exam (2013). - CT offers **excellent spatial resolution** for detecting metastases in **bone, lung, liver, and lymph nodes**. - It is widely available, relatively quick, and provides comprehensive anatomical information. - **Modern Update:** While CT was the standard in 2013, **PET-CT (FDG-PET/CT) is now considered the gold standard** for whole-body staging in metastatic breast cancer due to its combined metabolic and anatomical imaging capabilities. However, PET-CT was not among the options in this historical question. *Magnetic Resonance Imaging* - **MRI** is highly sensitive for specific sites, particularly for **brain metastases** and **bone metastases (especially spine and bone marrow)**. - **Whole-body MRI** protocols are emerging but require longer acquisition times and specialized equipment. - Not ideal as a single first-line modality for comprehensive whole-body staging compared to CT (or modern PET-CT). *Angiography* - **Angiography** is an invasive vascular imaging procedure used to visualize **arterial blood flow**. - It has **no role in routine metastatic screening or staging** of breast cancer. - Reserved for specific indications like preoperative vascular mapping or interventional procedures. *Venography* - **Venography** specifically visualizes **venous structures** and is used to detect venous thrombosis or venous obstructions. - It is **not applicable** for detecting solid organ metastases, bone lesions, or lymph node involvement in cancer staging.