All SubjectsAnatomy (110)Anesthesiology (34)Biochemistry (129)Community Medicine (109)Dental (16)Dermatology (34)ENT (62)Forensic Medicine (100)General Medicine (2)Internal Medicine (120)Microbiology (108)Obstetrics and Gynecology (79)Ophthalmology (78)Orthopaedics (41)Pathology (90)Pediatrics (33)Pharmacology (134)Physiology (91)Psychiatry (6)Psychiatry (81)Radiology (41)Surgery (52)
Q71
Torsades de pointes is seen in all except
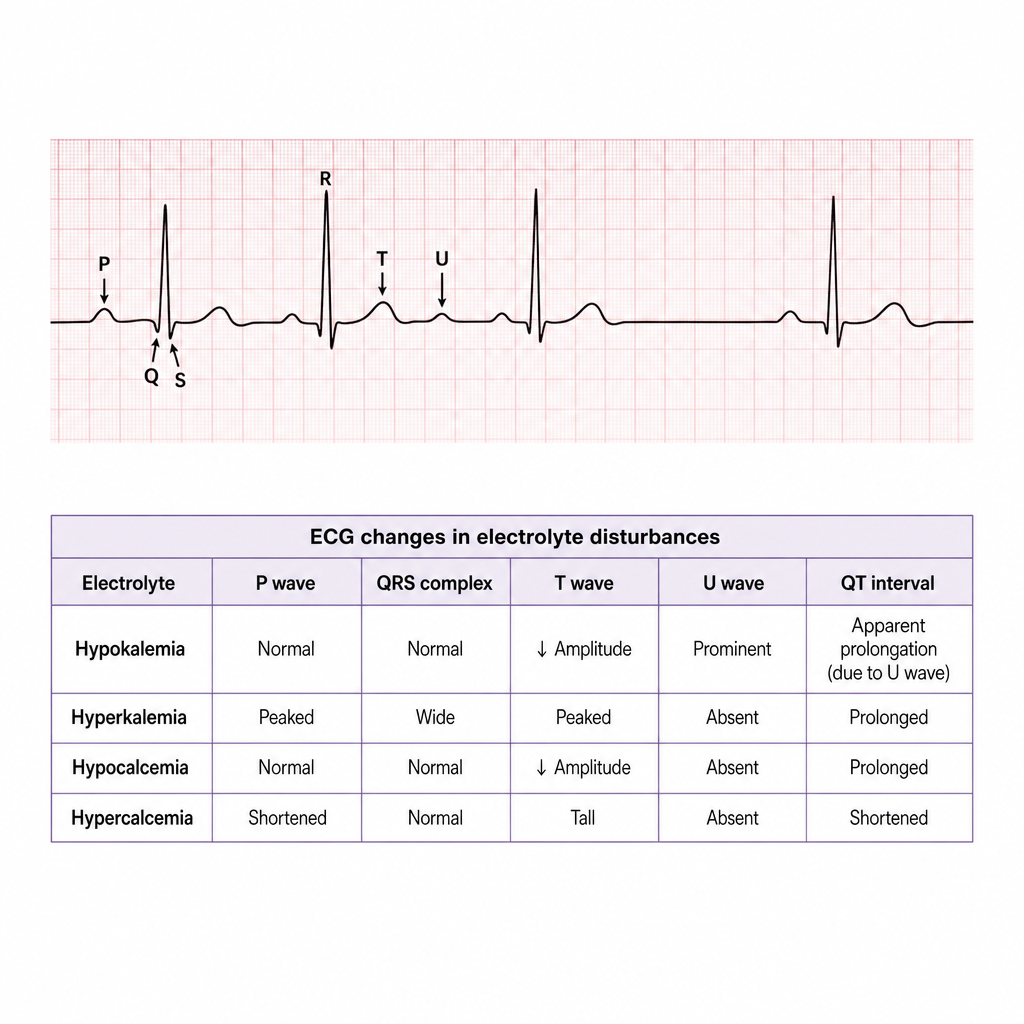
Q72
ECG image showing U wave. Patient is on furosemide and beta blocker. What is the most likely diagnosis?
Q73
Which of the following statements is true regarding the diagnostic criteria for Chronic Obstructive Pulmonary Disease (COPD)?
Q74
In which condition is Cepacia syndrome most commonly associated?
Q75
What is the most common cause of lobar consolidation?
Q76
Which of the following is not a clinical feature of Bronchiectasis?
Q77
The physiological marker of the last stage of acute asthma is
Q78
Which of the following is a characteristic finding in distal RTA?
Q79
Which of the following is not a feature of distal renal tubular acidosis
Q80
Hyperkalemia aciduria is seen in