All SubjectsAnatomy (110)Anesthesiology (34)Biochemistry (129)Community Medicine (109)Dental (16)Dermatology (34)ENT (62)Forensic Medicine (100)General Medicine (2)Internal Medicine (120)Microbiology (108)Obstetrics and Gynecology (79)Ophthalmology (78)Orthopaedics (41)Pathology (90)Pediatrics (33)Pharmacology (134)Physiology (91)Psychiatry (6)Psychiatry (81)Radiology (41)Surgery (52)
Q101
What is the recommended time frame for completing a blood transfusion after initiation?
Q102
What is the recommended rate of correction for sodium deficit in patients with chronic hyponatremia?
Q103
Graham Steell murmur is associated with which of the following conditions?
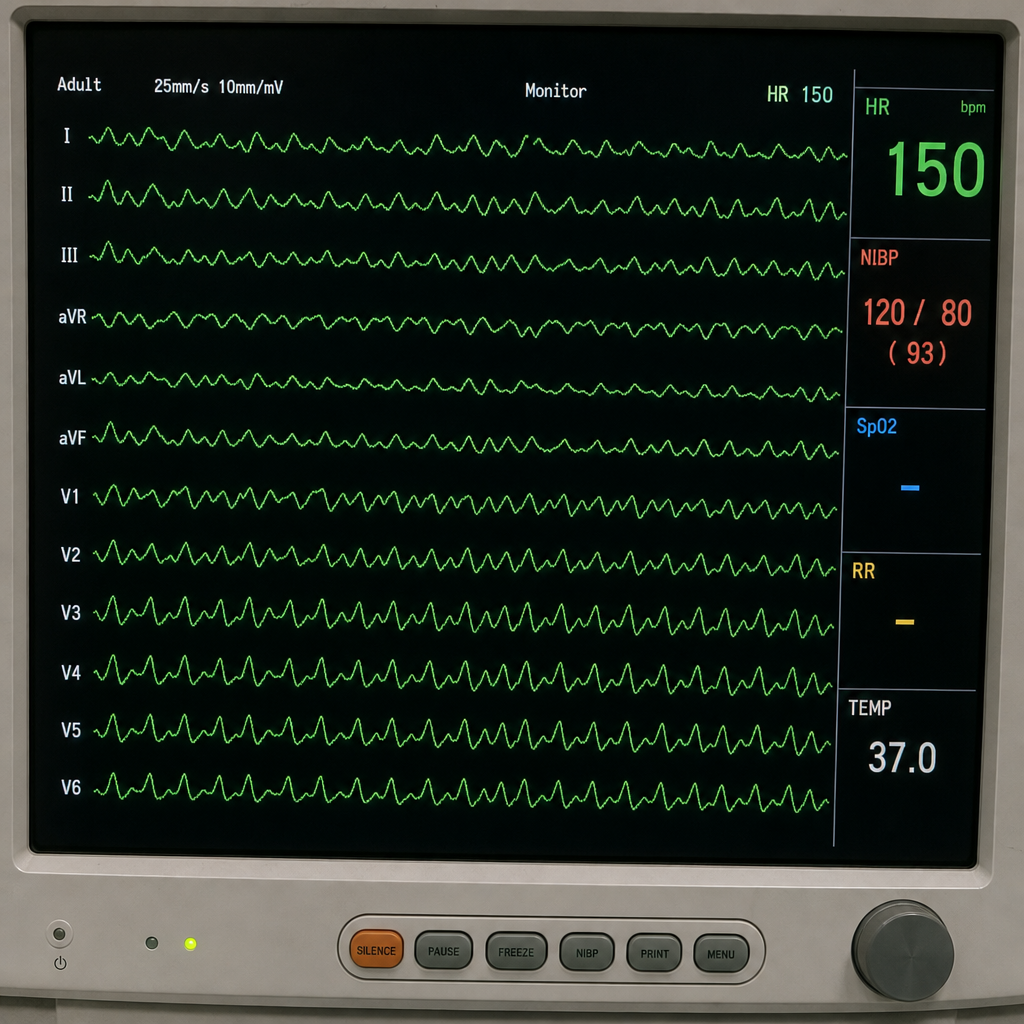
Q104
Refer to the provided ECG image. It demonstrates which of the following?
Q105
Wireless capsule endoscopy is done to visualize which of the following condition?
Q106
In a patient with heart disease, which condition is most commonly associated with left atrial enlargement?
Q107
Lovibond profile sign is seen in ?
Q108
All are seen in Behçet's syndrome except:
Q109
Match stick test is positive in ?
Q110
Which of the following is a characteristic feature of Granulomatosis with polyangiitis?