Down beat nystagmus is seen in?
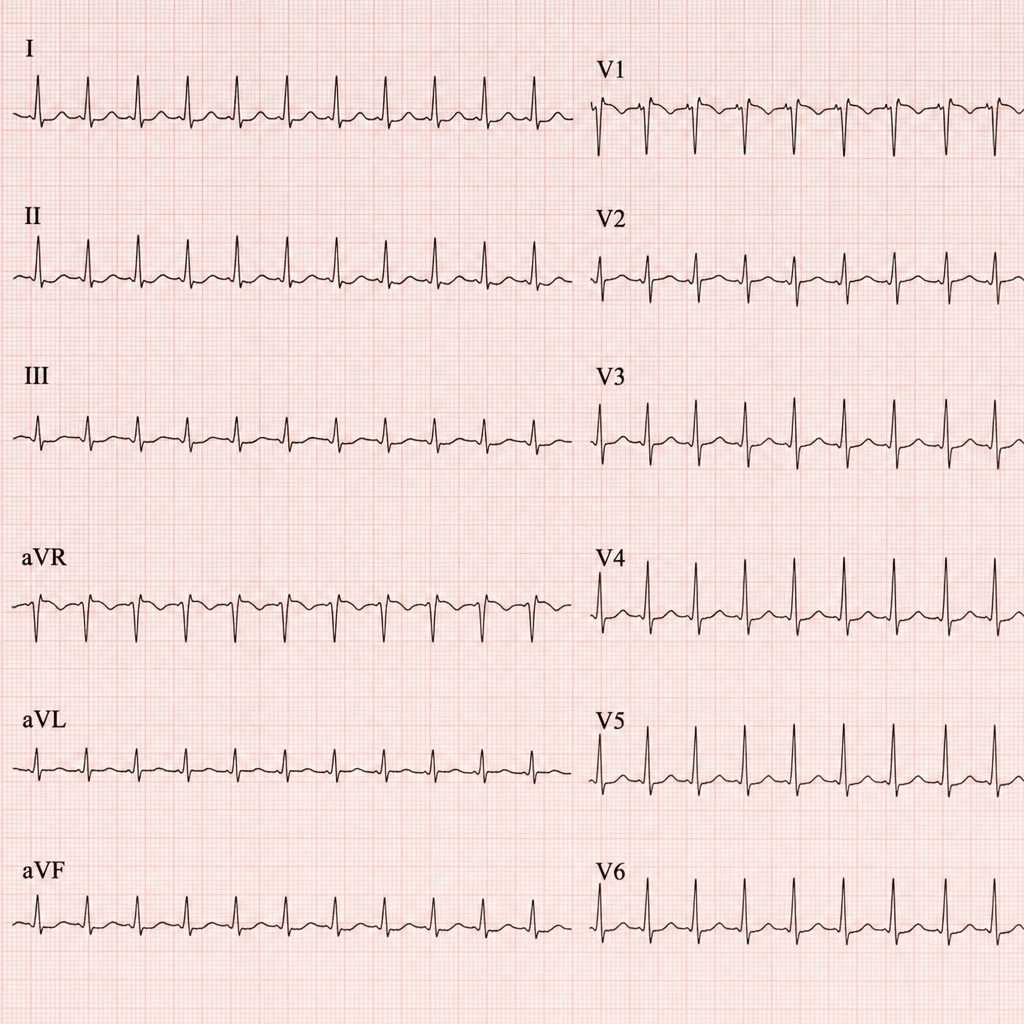
This patient came to the casualty with palpitations. His ECG has been shown below. What is your diagnosis?
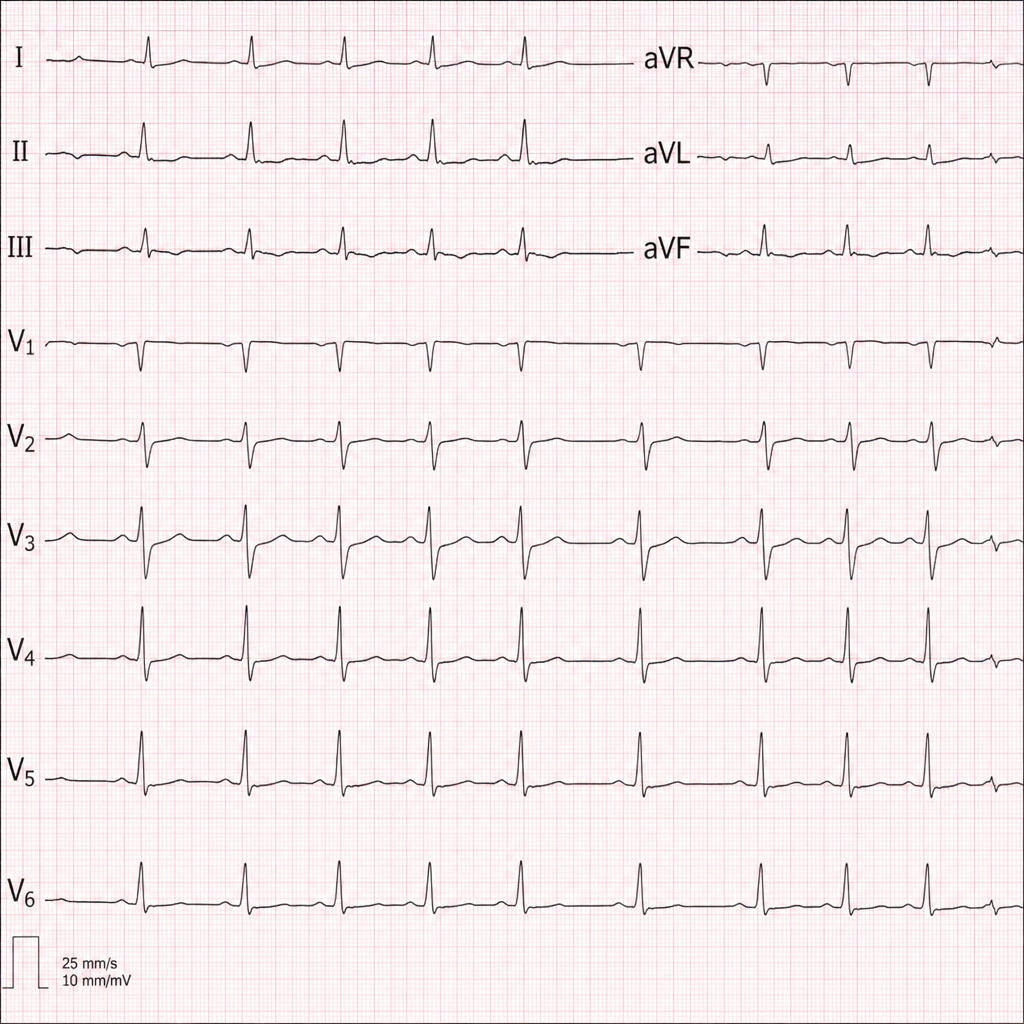
Diagnose the underlying medical disorder based on the ECG changes.
Which of the following is not an absolute indication for hemodialysis?
Which of the following is NOT a feature of scleroderma?
A 40-year-old male patient presents to the Emergency department with central chest pain for 2 hours. The ECG shows ST segment depression and cardiac troponins are elevated. The patient has a positive history of previous PCI 3 months back. He is administered Aspirin, Clopidogrel, Nitrates, and LMWH in the Emergency Department and shifted to the coronary care unit. What is the best recommended course of further action?
What is the best immediate management strategy for a patient experiencing respiratory alkalosis due to anxiety-induced hyperventilation?
Adrenal reserve is best tested by means of infusion with
What is the recommended time frame for completing a blood transfusion after initiation?
What is the recommended rate of correction for sodium deficit in patients with chronic hyponatremia?