All SubjectsAnatomy (104)Anesthesiology (21)Biochemistry (179)Community Medicine (104)Dental (9)Dermatology (21)ENT (2)Forensic Medicine (41)General Medicine (2)Internal Medicine (79)Microbiology (83)Obstetrics and Gynecology (63)Ophthalmology (68)Orthopaedics (36)Pathology (82)Pediatrics (43)Pharmacology (85)Physiology (91)Psychiatry (2)Psychiatry (20)Radiology (28)Surgery (53)
Q91
Which of the following is not a neural plate inducer?
Q92
Unilateral lacrimal gland destruction may be caused by?
Q93
Which of the following extraocular muscle has the longest tendon?
Q94
After trauma, a person cannot move their eye outward beyond the midpoint. Which nerve is injured?
Q95
In the case of a penile injury, which of the following structures prevents the extravasation of blood?
Q96
A person inhaled a peanut two days ago and is now unable to cough it out. Where is the possible location?
Q97
In axillary nerve paralysis, which of the following statements is false?
Q98
The commonest site of aspiration of a foreign body in the supine position is into the:
Q99
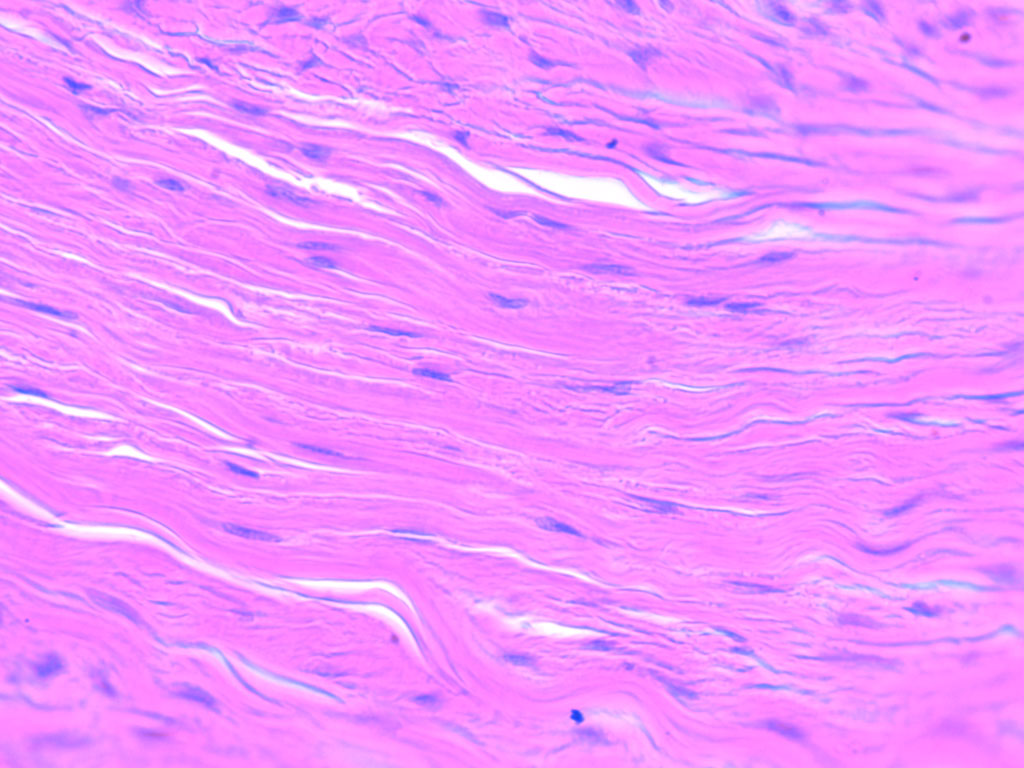
Identify the type of connective tissue present in the image.
Q100
Which arteries supply the talus?