
Cardiovascular System — MCQs

On this page
From the given pressure-volume curve, identify the end-diastolic volume (EDV) and end-systolic volume (ESV), then calculate the ejection fraction using the formula EF = (EDV - ESV)/EDV × 100%.
What is the definition of preload in the context of cardiac physiology?
Which of the following statements about volume receptors is NOT true?
Which of the following factors increases stroke volume?
Which one of the following is the CORRECT statement regarding coronary blood flow?
Mechanism by which Ach decreases heart rate is by:
Which of the following components are included in microcirculation?
What is the primary neural mechanism responsible for vasoconstriction in the skin?
Volume receptors are primarily located in which of the following?
In which lead is the normal P wave inverted?
Cardiovascular System Indian Medical PG Practice Questions and MCQs
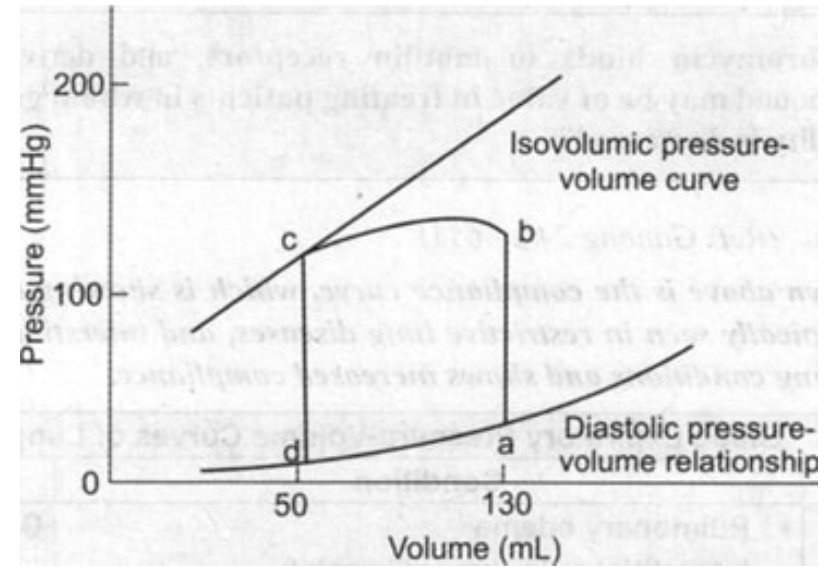
Question 881: From the given pressure-volume curve, identify the end-diastolic volume (EDV) and end-systolic volume (ESV), then calculate the ejection fraction using the formula EF = (EDV - ESV)/EDV × 100%.
- A. 40%
- B. 50%
- C. 55%
- D. 60% (Correct Answer)
Explanation: ***60%*** - From the pressure-volume loop, the **end-diastolic volume (EDV)** is the volume at point 'a', which is **130 mL**. - The **end-systolic volume (ESV)** is the volume at point 'd', which is **50 mL**. - Using the formula EF = (EDV - ESV) / EDV × 100% = (130 mL - 50 mL) / 130 mL × 100% = 80 mL / 130 mL × 100% = **61.5%**, which rounds to **60%** (the closest option). *40%* - To obtain an ejection fraction of 40%, the ESV would need to be higher, or the EDV lower, than what is indicated by the points 'a' and 'd' on the graph. - (130 - ESV) / 130 = 0.40 => 130 - ESV = 52 => ESV = 78 mL. This isn't consistent with the graph. *50%* - An ejection fraction of 50% would mean that the heart ejected half of its EDV. - (130 - ESV) / 130 = 0.50 => 130 - ESV = 65 => ESV = 65 mL. This value for ESV is not depicted at point 'd'. *55%* - For an ejection fraction of 55%, the calculation would yield a different ESV than what is presented in the curve. - (130 - ESV) / 130 = 0.55 => 130 - ESV = 71.5 => ESV = 58.5 mL. This is not the ESV at point 'd'.
Question 882: What is the definition of preload in the context of cardiac physiology?
- A. Volume of blood in the ventricles at the end of systole
- B. Volume of blood in the ventricles at the end of diastole (Correct Answer)
- C. Amount of blood pumped by the heart per beat
- D. Resistance to blood flow in the arteries
Explanation: ***Volume of blood in the ventricles at the end of diastole*** - Preload represents the **initial stretching** of the cardiac myocytes prior to contraction, largely determined by the **volume of blood filling the ventricles** at the end of relaxation (diastole). - This **end-diastolic volume** directly correlates with the ventricular muscle fiber length at the start of systole, influencing the force of contraction according to the **Frank-Starling mechanism**. *Volume of blood in the ventricles at the end of systole* - This describes the **end-systolic volume**, which is the amount of blood remaining in the ventricle after it has contracted and ejected blood. - End-systolic volume is a determinant of the **ejection fraction** but does not define preload. *Amount of blood pumped by the heart per beat* - This refers to the **stroke volume**—the volume of blood ejected from the left ventricle with each heartbeat. - While preload influences stroke volume, stroke volume itself is not the definition of preload. *Resistance to blood flow in the arteries* - This describes **afterload**, which is the pressure or resistance the ventricle must overcome to eject blood during systole. - Afterload primarily affects the *force* needed for contraction, rather than the initial stretch or filling volume of the heart.
Question 883: Which of the following statements about volume receptors is NOT true?
- A. They are located in carotid sinus (Correct Answer)
- B. They are low pressure receptors
- C. They mediate vasopressin release
- D. They provide afferents for thirst control
Explanation: ***They are located in carotid sinus*** - Volume receptors, primarily **atrial stretch receptors** and receptors in the **pulmonary vessels**, are located in the low-pressure areas of the circulation, not the carotid sinus. - The carotid sinus primarily contains **baroreceptors** which detect changes in arterial pressure, not blood volume. *They are low pressure receptors* - This statement is true; volume receptors are indeed **low-pressure receptors** found in the atria and great veins. - They primarily monitor **extracellular fluid volume** and central venous pressure. *They provide afferents for thirst control* - This statement is true; when blood volume decreases, the firing rate of these receptors decreases, signaling the **central nervous system** to stimulate thirst. - This is an important mechanism for regulating **fluid intake** and maintaining hydration. *They mediate vasopressin release* - This statement is true; a decrease in blood volume reduces the afferent signaling from volume receptors, which consequently stimulates the release of **vasopressin (ADH)**. - Vasopressin then increases **water reabsorption** in the kidneys to conserve fluid.
Question 884: Which of the following factors increases stroke volume?
- A. Increased end-diastolic and end-systolic volumes
- B. Decreased end-diastolic and end-systolic volumes
- C. Increased end-diastolic volume and decreased end-systolic volume (Correct Answer)
- D. Decreased end-diastolic volume and increased end-systolic volume
Explanation: ***Increased end-diastolic volume and decreased end-systolic volume*** - **Stroke volume (SV)** is calculated as **End-Diastolic Volume (EDV)** minus **End-Systolic Volume (ESV)**. Therefore, increasing the volume before contraction while decreasing the volume after contraction will maximize the ejected blood. - A higher **EDV** signifies greater **preload** (more blood filling the ventricle), and a lower **ESV** indicates more complete ejection of blood, often due to increased **contractility** or decreased **afterload**. *Increased end-diastolic and end-systolic volumes* - While an **increased EDV** would tend to increase stroke volume, an **increased ESV** suggests that the heart is ejecting less blood per beat, which would decrease stroke volume. - The combined effect makes it less likely to unequivocally increase stroke volume, as the increase in ESV might offset or even surpass the effect of increased EDV. *Decreased end-diastolic and end-systolic volumes* - Both a **decreased EDV** (less filling) and a **decreased ESV** (more complete ejection) work against each other in terms of stroke volume calculation. - If **EDV** decreases, there's less blood to eject, and if the decrease in **EDV** is proportionally larger than the decrease in **ESV**, stroke volume will decrease. *Decreased end-diastolic volume and increased end-systolic volume* - A **decreased EDV** means less blood is available for ejection, reducing preload and the amount of blood the heart can pump. - An **increased ESV** means the heart is ejecting less blood with each beat, indicating reduced contractility or increased afterload, both of which would decrease stroke volume.
Question 885: Which one of the following is the CORRECT statement regarding coronary blood flow?
- A. Coronary blood flow is directly related to perfusion pressure and inversely related to resistance (Correct Answer)
- B. Coronary blood flow is inversely related to perfusion pressure and directly related to resistance
- C. Coronary blood flow is directly related to perfusion pressure and also to resistance
- D. Coronary blood flow is inversely related to both pressure and resistance
Explanation: ***Coronary blood flow is directly related to perfusion pressure and inversely related to resistance*** - According to Ohm's law, **blood flow** is directly proportional to the **pressure gradient (perfusion pressure)** and inversely proportional to the **vascular resistance**. - This fundamental principle applies to coronary circulation, meaning higher pressure drives more flow, while higher resistance impedes it. *Coronary blood flow is inversely related to perfusion pressure and directly related to resistance* - This statement contradicts the basic principles of **fluid dynamics** and **Ohm's law**, where a higher pressure gradient generally leads to increased flow. - Direct proportionality to resistance would imply that increased obstruction leads to increased flow, which is physiologically incorrect. *Coronary blood flow is directly related to perfusion pressure and also to resistance* - While a direct relationship with **perfusion pressure** is correct, directly relating flow to **resistance** is incorrect. - Increased resistance, such as that caused by **atherosclerosis**, reduces blood flow, not increases it. *Coronary blood flow is inversely related to both pressure and resistance* - An inverse relationship with **pressure** is incorrect as an increase in the driving pressure should increase flow. - An inverse relationship with **resistance** is correct, but the inverse relationship with pressure makes the entire statement incorrect.
Question 886: Mechanism by which Ach decreases heart rate is by:
- A. Prolongation of action potential duration
- B. Reduction in calcium influx
- C. Inhibition of sympathetic activity
- D. Delayed diastolic depolarization (Correct Answer)
Explanation: ***Delayed diastolic depolarization*** - Acetylcholine (ACh) binding to muscarinic receptors on nodal cells increases **potassium permeability**, leading to a more negative maximal diastolic potential. - This slows the rate of **spontaneous depolarization** (pacemaker potential), thereby delaying the point at which the threshold for an action potential is reached and reducing heart rate. *Prolongation of action potential duration* - ACh typically **shortens** the action potential duration in atrial and nodal cells by increasing potassium efflux, which hyperpolarizes the cell and hastens repolarization. - A prolonged action potential duration would generally lead to a **slower heart rate** by increasing the refractory period, but this is achieved through different ionic mechanisms and is not the primary mechanism of ACh. *Reduction in calcium influx* - While ACh does reduce the inward **calcium current (ICa)** in nodal cells, contributing to a slower heart rate and weaker contractility, this effect primarily influences the upstroke and peak of the action potential. - The more **fundamentally important mechanism** for heart rate reduction is the impact on the pacemaker potential's slope, which is governed by altered ion conductances, predominantly potassium. *Inhibition of sympathetic activity* - ACh acts directly on **muscarinic receptors** on cardiac cells to decrease heart rate, which is a parasympathetic effect. - It does not directly inhibit sympathetic nerve activity but rather **counteracts sympathetic effects** by directly modulating cardiac cell physiology.
Question 887: Which of the following components are included in microcirculation?
- A. Capillaries
- B. Aorta
- C. Arteries and veins
- D. Capillaries, venules, and arterioles (Correct Answer)
Explanation: ***Capillaries, venules, and arterioles*** - **Microcirculation** is the portion of the **circulatory system** that includes the **smallest blood vessels**, specifically the **arterioles**, **capillaries**, and **venules**. - These vessels are crucial for the **delivery of oxygen** and **nutrients** to tissues and the removal of waste products. *Capillaries* - While **capillaries** are a vital part of **microcirculation** and the primary site of nutrient and waste exchange, they alone do not encompass the entire microcirculatory unit. - The microcirculation also includes the vessels that feed into and drain from the capillaries: the **arterioles** and **venules**. *Aorta* - The **aorta** is the **largest artery** in the body, part of the **macrocirculation**, which distributes blood from the heart to the systemic circulation. - It is not considered part of the **microcirculation** due to its large size and primary function as a high-pressure conduit rather than a site of exchange. *Arteries and veins* - **Arteries** and **veins** are primarily components of the **macrocirculation**, responsible for transporting blood to and from the systemic and pulmonary circuits. - While arterioles and venules (small arteries and veins) are part of the microcirculation, the broader terms "arteries" and "veins" typically refer to the larger vessels and do not exclusively define the microcirculatory network.
Question 888: What is the primary neural mechanism responsible for vasoconstriction in the skin?
- A. Sympathetic (Correct Answer)
- B. Parasympathetic
- C. Enteric nervous system
- D. Somatic nervous system
Explanation: ***Sympathetic nervous system*** - The **sympathetic nervous system** primarily controls blood vessel tone, including vasoconstriction in the skin, through the release of **norepinephrine**. - **Adrenergic receptors** (alpha-1) on vascular smooth muscle cells respond to norepinephrine, leading to contraction and narrowing of the blood vessels. *Parasympathetic nervous system* - The **parasympathetic nervous system** generally has very limited, if any, direct innervation to cutaneous blood vessels for vasoconstriction; its primary role in the cardiovascular system is to decrease heart rate. - While it can cause vasodilation in some tissues, it does not mediate vasoconstriction in the skin. *Somatic nervous system* - The **somatic nervous system** is responsible for voluntary muscle control and transmitting sensory information, not for regulating **autonomic functions** like skin blood flow. - It innervates **skeletal muscles** and sensory receptors directly, lacking connections to cutaneous blood vessels for vasoconstriction. *Enteric nervous system* - The **enteric nervous system** is a complex network of neurons found within the walls of the **gastrointestinal tract**, where it primarily controls digestion. - It does not play any direct role in regulating vasoconstriction in the skin.
Question 889: Volume receptors are primarily located in which of the following?
- A. Carotid sinus and aortic arch
- B. Right and left atria (Correct Answer)
- C. Pulmonary arteries only
- D. Renal juxtaglomerular apparatus
Explanation: **Correct: *Right and left atria*** - The **atria** contain **low-pressure baroreceptors** (volume receptors) that primarily sense changes in circulating blood volume. - These receptors respond to stretching of the atrial walls, which occurs with increased blood volume, signaling the need for fluid excretion. *Incorrect: Carotid sinus and aortic arch* - These locations house **high-pressure baroreceptors** that primarily regulate **arterial blood pressure**, not circulating volume. - They respond to changes in the stretch of the arterial walls caused by blood pressure fluctuations. *Incorrect: Renal juxtaglomerular apparatus* - This apparatus primarily senses changes in **renal perfusion pressure** and **sodium delivery** to the distal tubule. - It plays a crucial role in regulating blood pressure and fluid balance through the **renin-angiotensin-aldosterone system (RAAS)**, but its primary role is not as a volume receptor. *Incorrect: Pulmonary arteries only* - While pulmonary baroreceptors exist, they primarily monitor **pulmonary arterial pressure** and do not serve as the main volume receptors for the systemic circulation. - Volume receptors are distributed more broadly within the low-pressure venous system.
Question 890: In which lead is the normal P wave inverted?
- A. LI
- B. LII
- C. aVF
- D. aVR (Correct Answer)
Explanation: **Correct: *aVR*** - In lead **aVR**, the electrical activity is recorded from the perspective of the **right arm** towards the left foot and arm. Since the P wave represents atrial depolarization, which normally originates in the **sinoatrial node** in the right atrium and spreads leftward and inferiorly, the impulse moves away from the positive electrode of aVR. - This movement away from aVR's positive electrode causes a **negative (inverted)** deflection, which is a normal finding for the P wave in this lead. *Incorrect: LI* - Lead I records electrical activity between the **right arm (negative)** and the **left arm (positive)**. - As atrial depolarization moves towards the left arm, the P wave is normally **upright** in lead I. *Incorrect: LII* - Lead II records electrical activity between the **right arm (negative)** and the **left leg (positive)**. - Because atrial depolarization (from SA node) spreads downwards and to the left, it moves predominantly towards the positive electrode of lead II, resulting in an **upright** P wave. *Incorrect: aVF* - Lead aVF records electrical activity towards the **left foot (positive)**, providing an inferior view of the heart. - Since atrial depolarization moves inferiorly towards the left leg, the P wave in aVF is typically **upright**.
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Start For Free