
Neoplasia — MCQs

On this page
Grade of tumor denotes
In which type of cancer is K-ras mutation most commonly observed?
Which of the following is included in the Modified Bloom Richardson criteria for Carcinoma Breast?
A 59-year-old lady presents with a progressive, painless lump in the breast. What is the cause of the skin change associated with breast cancer?
An elderly male is known as a smoker presented with chronic cough, significant weight loss, and fatigue. Serum calcium level is raised. A lung biopsy was done, and it showed large atypical cells with hyperchromasia. What is the probable diagnosis?
What is the T stage classification for a lung carcinoma measuring 2.5 cm and not involving the pleura?
A 25-year-old male presented with a 2cm thyroid nodule. A thyroidectomy was done. The histology picture is given below. What could be the diagnosis based on the histological findings?
Anaplasia is
RET proto-oncogene is associated with the development of
Which is the most common type of male breast cancer?
Neoplasia Indian Medical PG Practice Questions and MCQs
Question 861: Grade of tumor denotes
- A. Degree of differentiation (Correct Answer)
- B. Degree of anaplasia
- C. Stage of disease
- D. Vascular invasion
Explanation: ***Degree of differentiation*** - The grade of a tumor is primarily defined by the **degree of differentiation** of the cancer cells, indicating how much the tumor cells resemble normal cells [2]. - Grading helps predict the **aggressiveness** of cancer and its behavior in the body. *Vascular invasion* - Vascular invasion refers to the presence of cancer cells within blood vessels and is more associated with tumor **stage** rather than the **grade**. - It indicates the potential for cancer to metastasize, but it does not reflect the differentiation of cells. *Stage of disease* - The stage of disease encompasses the extent of tumor spread and includes aspects such as **size** and **lymph node involvement**, rather than the cellular characteristics of differentiation. - Staging is about **how advanced** the cancer is, while grading focuses on the **appearance** of the tumor cells. *Degree of anaplasia* - Anaplasia refers to the loss of differentiation and organization of cells [1][2], which can relate to tumor **grade**, but it is not synonymous with grading itself. - While higher grades indicate greater anaplasia, not all anaplastic tumors are graded the same due to other factors influencing classification. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Neoplasia, pp. 278-280. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Neoplasia, pp. 276-278.
Question 862: In which type of cancer is K-ras mutation most commonly observed?
- A. Prostate cancer
- B. Gastric cancer
- C. Liver cancer
- D. Pancreatic cancer (Correct Answer)
Explanation: ***Pancreatic carcinoma*** - K-ras mutations are found in **over 90%** of pancreatic adenocarcinomas, making it a hallmark of this cancer type [1]. - These mutations are involved in the **initiation and progression** of pancreatic tumors [1]. *Hepatic carcinoma* - Hepatic carcinoma is more associated with mutations in **TP53** and **CTNNB1**, rather than K-ras mutations. - K-ras mutations are not a primary driver in the context of liver cancer development. *Prostate carcinoma* - Prostate carcinoma typically involves mutations in **PTEN** and **TMPRSS2-ERG** fusion genes, not K-ras. - K-ras mutations are not a significant feature in the pathogenesis of prostate cancer. *Gastric carcinoma* - Gastric carcinoma can have mutation involvement often related to **CDH1** and **TP53**, with variable K-ras mutation presence. - K-ras mutations are less frequent when compared to other mutations seen in gastric tumorigenesis. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Pancreas, pp. 897-898.
Question 863: Which of the following is included in the Modified Bloom Richardson criteria for Carcinoma Breast?
- A. Desmoplasia
- B. Lymphovascular invasion
- C. Mitotic rate (Correct Answer)
- D. Nuclear pleomorphism
Explanation: ***Mitotic rate*** - The **Modified Bloom-Richardson (Nottingham) criteria** for breast carcinoma grading includes three components: **tubular/glandular formation**, **nuclear pleomorphism**, and **mitotic rate**. - **Mitotic rate** assesses the frequency of cell division and is scored based on the number of mitoses per 10 high-power fields. - A higher mitotic rate indicates more aggressive tumor growth and contributes to a higher histological grade. *Desmoplasia* - **Desmoplasia** refers to the fibrous stromal reaction surrounding a tumor and is a common feature of invasive carcinomas. - While it is associated with tumor invasion, it is **not one of the three specific criteria** used in the Modified Bloom-Richardson grading system. - The MBR system focuses on cellular morphology and proliferative activity, not stromal response. *Lymphovascular invasion* - **Lymphovascular invasion** (LVI) indicates the presence of tumor cells within lymphatic or blood vessels, signifying higher metastatic potential. - While LVI is an important **prognostic factor** in breast cancer staging and treatment planning, it is **not part of the MBR histological grading criteria**. - The MBR system evaluates only tubular formation, nuclear features, and mitotic activity. *Nuclear pleomorphism* - **Nuclear pleomorphism** (nuclear grade/nuclear atypia) is actually **one of the three components** of the Modified Bloom-Richardson criteria. - It assesses variation in nuclear size, shape, and chromatin pattern within tumor cells. - Both mitotic rate and nuclear pleomorphism are correct components of the MBR system; however, if forced to choose one answer, mitotic rate is more distinctly quantifiable and is often emphasized in teaching contexts.
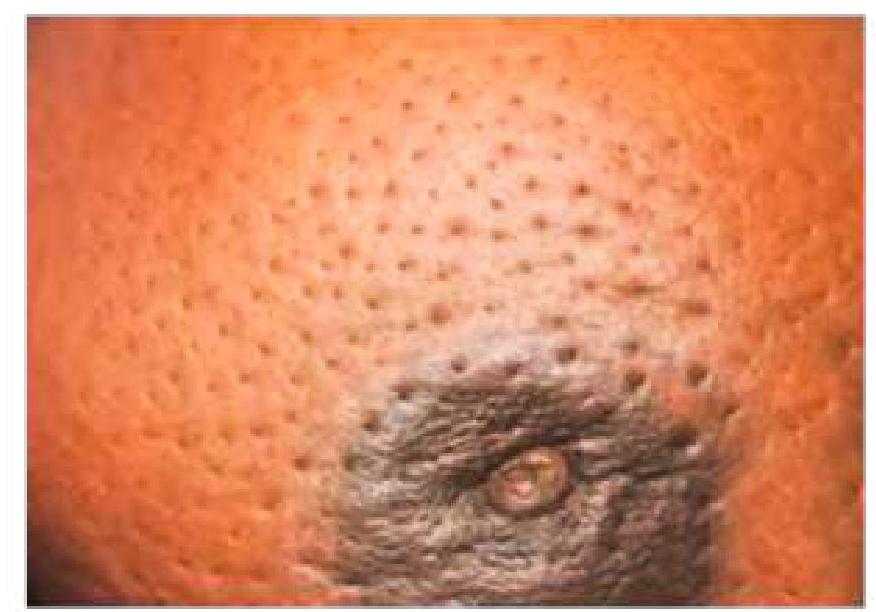
Question 864: A 59-year-old lady presents with a progressive, painless lump in the breast. What is the cause of the skin change associated with breast cancer?
- A. Infiltration of subdermal lymphatics (Correct Answer)
- B. Infiltration of the lactiferous duct
- C. Involvement of Cooper’s ligament
- D. Spread of the tumor to the anterior chest wall
Explanation: ***Infiltration of subdermal lymphatics*** - The skin change described often refers to **peau d'orange**, which is caused by the **blockage of superficial lymphatic vessels** by tumor cells [1]. - This lymphatic obstruction leads to **edema** and dimpling of the skin, resembling an orange peel [1]. *Infiltration of the lactiferous duct* - While cancer can arise in or infiltrate lactiferous ducts, this primarily causes symptoms like **nipple discharge**, inversion, or a palpable mass. - It does not directly explain the specific **skin dimpling** or **peau d'orange** appearance. *Involvement of Cooper's ligament* - Involvement of **Cooper's ligaments** (suspensory ligaments of the breast) can cause skin dimpling or retraction [1]. - However, the image depicts widespread **peau d'orange**, which is more commonly associated with lymphatic involvement than direct ligamentous retraction [1]. *Spread of the tumor to the anterior chest wall* - Tumor extension to the **anterior chest wall** signifies advanced disease and can cause **fixation of the breast** to underlying structures or skin ulceration [2]. - This typically results in **immobility of the breast** or an ulcerated lesion, not the widespread edematous and dimpled appearance of **peau d'orange**. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 453-454. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 456-457.
Question 865: An elderly male is known as a smoker presented with chronic cough, significant weight loss, and fatigue. Serum calcium level is raised. A lung biopsy was done, and it showed large atypical cells with hyperchromasia. What is the probable diagnosis?
- A. Large cell carcinoma (Correct Answer)
- B. Small cell lung carcinoma
- C. Squamous cell carcinoma
- D. Lung adenocarcinoma
Explanation: ***Squamous cell carcinoma*** - The presence of **hyperchromatic atypical cells** in the lung biopsy [2] and **elevated serum calcium levels** are indicative of paraneoplastic hypercalcemia often seen in squamous cell carcinoma. - This type of lung cancer typically occurs in **smokers** [1] and is associated with **chronic cough** and **weight loss**. *Large cell neuroendocrine tumor* - While it may show large atypical cells, this tumor type is less commonly associated with **hypercalcemia** or the smoking history highlighted here. - Characteristically, it tends to have a more aggressive course and distinct histological features not indicated in the vignette. *Small cell carcinoma* - This type typically presents with **central lung lesions** and is associated with secretory syndromes like **SIADH**, not hypercalcemia. - Histologically, it features small round blue cells rather than the large atypical cells described in this case. *Adenocarcinoma* - Often arises peripherally in the lung and typically does not present with hypercalcemia. - Histological features include **gland formation**, which contrasts with the **large atypical cells** noted in the biopsy. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Respiratory Tract Disease, pp. 336-337. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lung, pp. 723-724.
Question 866: What is the T stage classification for a lung carcinoma measuring 2.5 cm and not involving the pleura?
- A. T1a (tumor ≤ 1 cm)
- B. T2 (tumor > 3 cm)
- C. T1c (tumor > 2 cm but ≤ 3 cm) (Correct Answer)
- D. T1b (tumor > 1 cm but ≤ 2 cm)
Explanation: ***T1c (tumor > 2 cm but ≤ 3 cm)*** - A lung carcinoma measuring 2.5 cm falls within the **T1c classification** because it is greater than 2 cm but no larger than 3 cm. - The absence of **pleural involvement** confirms this is not a higher T stage (T2 or above) [1]. - According to the **8th Edition TNM Classification**, T1c specifically denotes tumors in this size range [1]. *T1a (tumor ≤ 1 cm)* - This classification is for tumors that are **1 cm or less in greatest dimension**, which is much smaller than the 2.5 cm tumor in the question. - T1a represents the **smallest category** of primary lung tumors [1]. *T2 (tumor > 3 cm)* - A T2 classification applies to tumors that are **larger than 3 cm** (T2a: > 3-4 cm, T2b: > 4-5 cm), which does not apply to a 2.5 cm tumor [1]. - T2 can also include smaller tumors with specific features like **visceral pleural invasion**, **main bronchus involvement**, or causing **atelectasis/obstructive pneumonitis**, none of which are present here [1]. *T1b (tumor > 1 cm but ≤ 2 cm)* - This classification applies to tumors **greater than 1 cm but not exceeding 2 cm** in greatest dimension. - The 2.5 cm tumor in the question **exceeds this size range**, making T1b incorrect [1]. - T1b represents an intermediate size between T1a and T1c [1]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lung, p. 725.
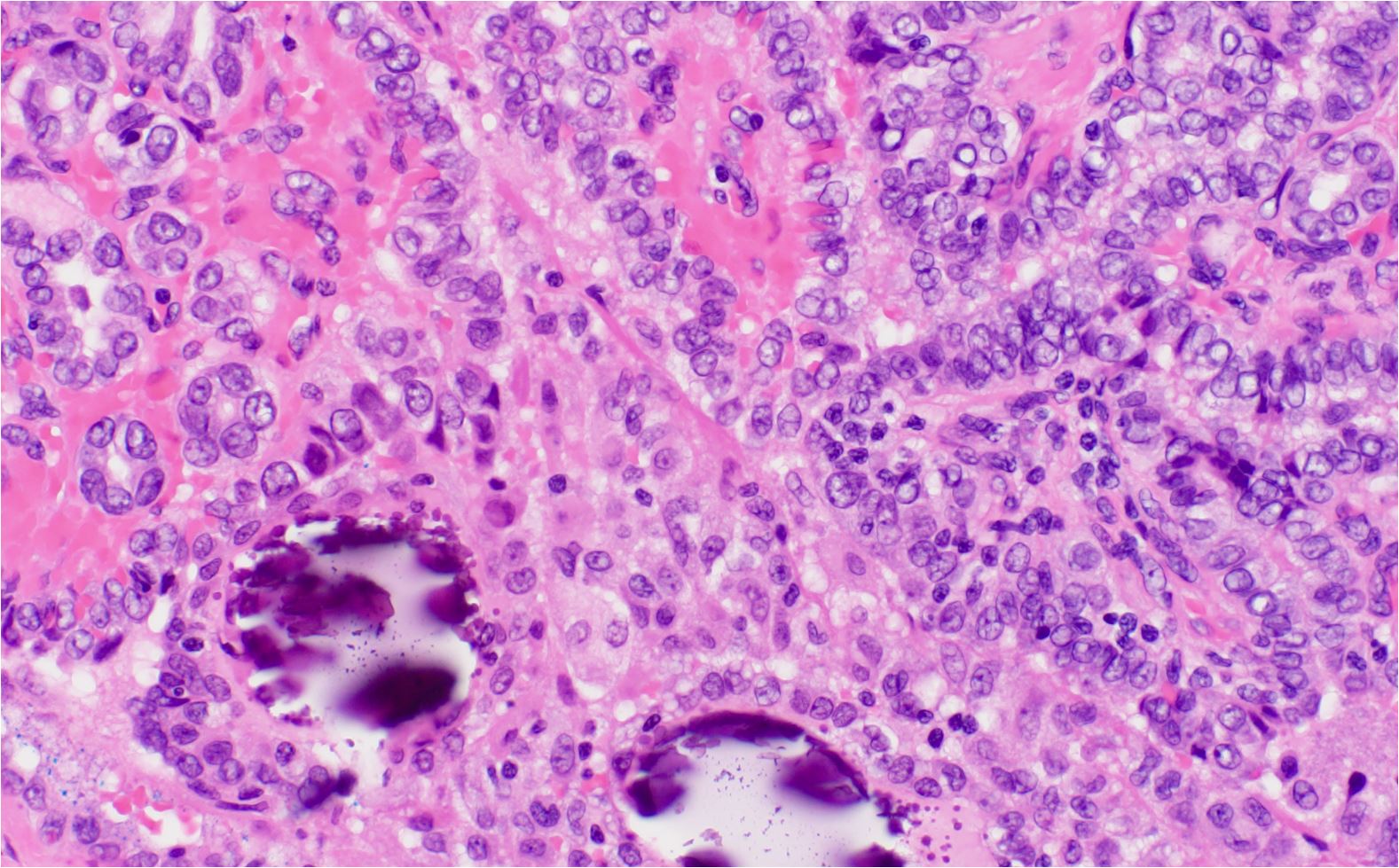
Question 867: A 25-year-old male presented with a 2cm thyroid nodule. A thyroidectomy was done. The histology picture is given below. What could be the diagnosis based on the histological findings?
- A. Papillary thyroid carcinoma (Correct Answer)
- B. Follicular thyroid adenoma
- C. Graves' disease
- D. Adenomatous goiter
Explanation: ***Papillary carcinoma thyroid*** [1] - Typically presents as a **thyroid nodule** with distinctive histological features such as **papillary structures** and nuclear **grooves or inclusions** [1]. - Often associated with a history of radiation exposure and is the most common type of **thyroid cancer** in young adults. *Graves disease* - Characterized by **hyperthyroidism** and usually presents with diffuse **goiter** rather than a solitary nodule. - Histological findings typically show **diffuse hyperplasia** rather than a well-circumscribed nodule. *Adenomatous goitre* - Usually presents as a **multinodular goiter** with no malignant potential. - Histologically characterized by **colloid accumulation** and enlarged follicles, not indicative of malignancy. *Follicular adenoma* [2] - Characterized by a well-encapsulated nodule with **uniform follicular cells** and abundant **colloid** [1,2]. - Does not exhibit the **invasive features** seen in malignancies like papillary carcinoma [1]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1099-1101. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 428-429.
Question 868: Anaplasia is
- A. Changing one type of epithelium to another
- B. Nuclear chromatin
- C. Lack of differentiation (Correct Answer)
- D. Morphological changes
Explanation: ***Lack of differentiation*** - Anaplasia refers to a **loss of differentiation** in cells, making them more primitive and less specialized [1]. - It is often seen in **malignant tumors**, indicating a poor prognosis and aggressive behavior [1]. *Morphological changes* - While anaplasia involves **morphological changes**, this term is too broad and can relate to various cellular alterations, not exclusively anaplasia [1]. - Anaplasia specifically emphasizes **lack of differentiation**, distinct from general changes in cell appearance [1]. *Changing one type of epithelium to another* - This describes a process known as **metaplasia**, where one adult cell type transforms into another, not anaplasia. - Anaplasia signifies a **de-differentiation** rather than a change to a different epithelial type [1]. *Nuclear chromatin* - While changes in **nuclear chromatin** can occur in anaplastic cells, this does not define anaplasia itself [1]. - Anaplasia primarily refers to **loss of cell differentiation**, making this option insufficient to describe the concept [1]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Neoplasia, pp. 276-280.
Question 869: RET proto-oncogene is associated with the development of
- A. Medullary carcinoma thyroid (Correct Answer)
- B. Astrocytoma
- C. Paraganglioma
- D. Hurthle cell tumor thyroid
Explanation: ***Medullary carcinoma thyroid*** - The **RET proto-oncogene** mutation is strongly linked to medullary thyroid carcinoma, particularly in Multiple Endocrine Neoplasia (MEN) type 2 syndrome [1]. - This carcinoma originates from **C-cells** of the thyroid, which produce calcitonin, and its presence is typically assessed via genetic testing. *Hurthle cell tumor thyroid* - Hurthle cell tumors, while associated with the thyroid, are not typically linked to **RET proto-oncogene** mutations but rather are considered a variant of follicular thyroid carcinoma. - They primarily appear as **eosinophilic cells** and are related to **radioactive iodine resistance**, which differs from medullary carcinoma. *Paraganglioma* - Paragangliomas arise from **neuroendocrine cells** and are associated with mutations in genes such as **SDHB** or **SDHD**, not RET. - They commonly present as **extra-adrenal pheochromocytomas** and are not related to thyroid pathology. *Astrocytoma* - Astrocytomas are primary **central nervous system tumors** that originate from astrocytic cells and have no known association with RET proto-oncogene mutations. - The mutations in this type of tumor are different, often involving genes like **TP53** and **IDH1**. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1102-1103.
Question 870: Which is the most common type of male breast cancer?
- A. Inflammatory Breast Cancer
- B. Invasive Ductal Carcinoma (Correct Answer)
- C. Invasive Lobular Carcinoma
- D. Mucinous Carcinoma
Explanation: ***Invasive Ductal Carcinoma*** - This is by far the most common type of breast cancer in men, accounting for approximately **80-90%** of all male breast cancer cases. - It originates in the **milk ducts** and then invades the surrounding breast tissue. *Invasive Lobular Carcinoma* - This type of cancer originates in the **milk-producing glands (lobules)**. - It is **extremely rare** in men due to the underdeveloped and non-functional lobules in the male breast. *Mucinous Carcinoma* - This is a **rare subtype** of invasive ductal carcinoma characterized by cancer cells that produce **mucin**. - It accounts for only a small percentage of male breast cancers, typically **2-3%** of cases. *Inflammatory Breast Cancer* - This is a **rare and aggressive** form of breast cancer characterized by rapid onset of redness, swelling, and warmth in the breast, often mistaken for an infection. - Although it can occur in men, it is not the most common type and represents a very small fraction of male breast cancer diagnoses.
Practice by Chapter
Nomenclature and Classification of Tumors
Practice Questions
Characteristics of Benign and Malignant Neoplasms
Practice Questions
Molecular Basis of Cancer
Practice Questions
Carcinogenesis and Carcinogens
Practice Questions
Tumor Progression and Metastasis
Practice Questions
Tumor Markers
Practice Questions
Paraneoplastic Syndromes
Practice Questions
Genetic Basis of Cancer
Practice Questions
Tumor Immunity
Practice Questions
Cancer Epidemiology and Prevention
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Start For Free