
Diseases of the Retina — MCQs

On this page
What is the power of lens attached to this instrument to visualize the entire retina?

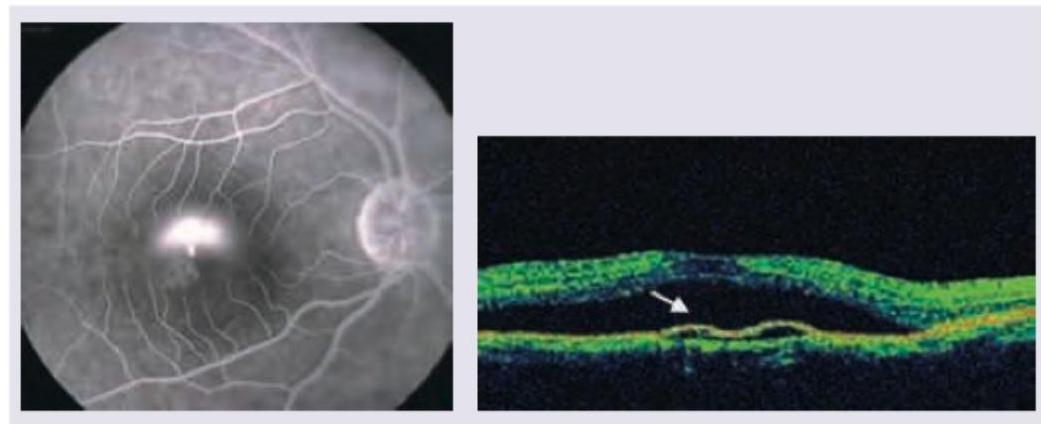
A 25-year-old young male presented with complaints of diminished vision in the right eye. On examination vision in left eye is 6/6 and right eye is 6/18. Shown are the FFA and optical coherence topography of the patient. The pathology lies in which layer of retina?
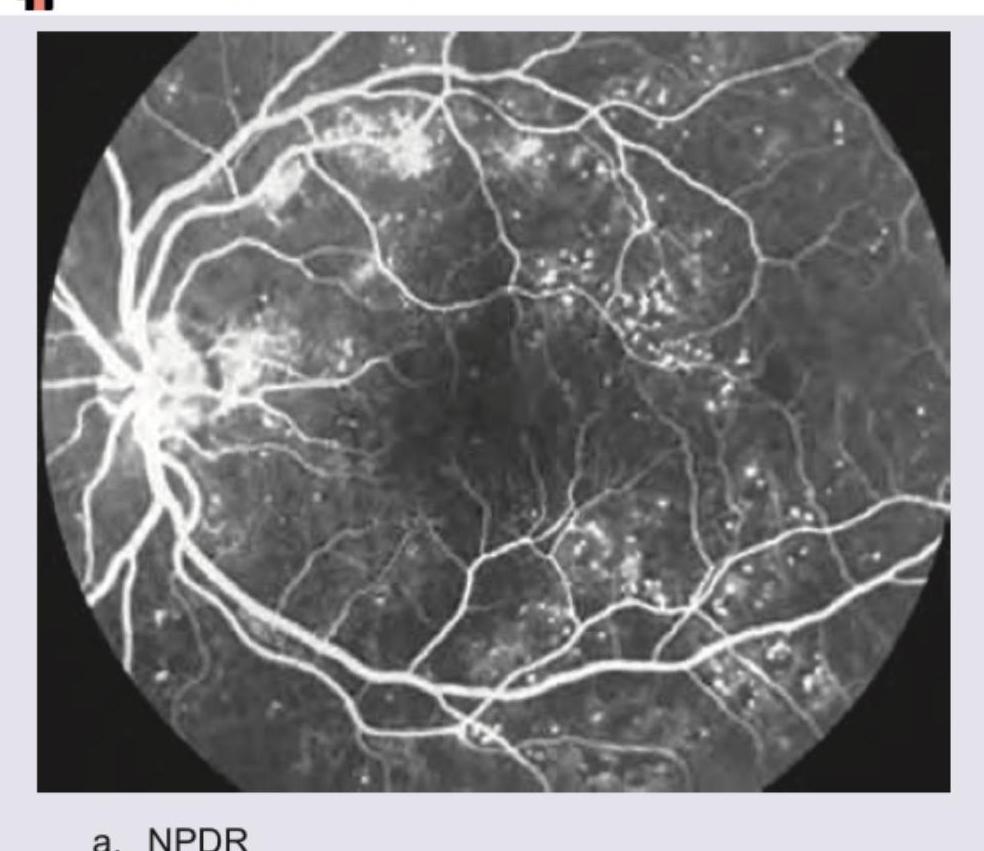
Identify the FFA picture:
Consider the following causes of visual loss : 1. Obstruction of the central retinal artery 2. Vitreous and retinal haemorrhage 3. Cataract 4. Retinal detachment Which of the above causes are associated with acute visual loss in a patient?
The most typical clinical presentation of a retinoblastoma is
While working in a primary health centre, an elderly patient presents with a history of sudden loss of vision and curtain falling sensation in one eye. This symptom is highly suggestive that the patient has the following condition:
In diabetes mellitus the following findings are seen in ophthalmoscopy except:
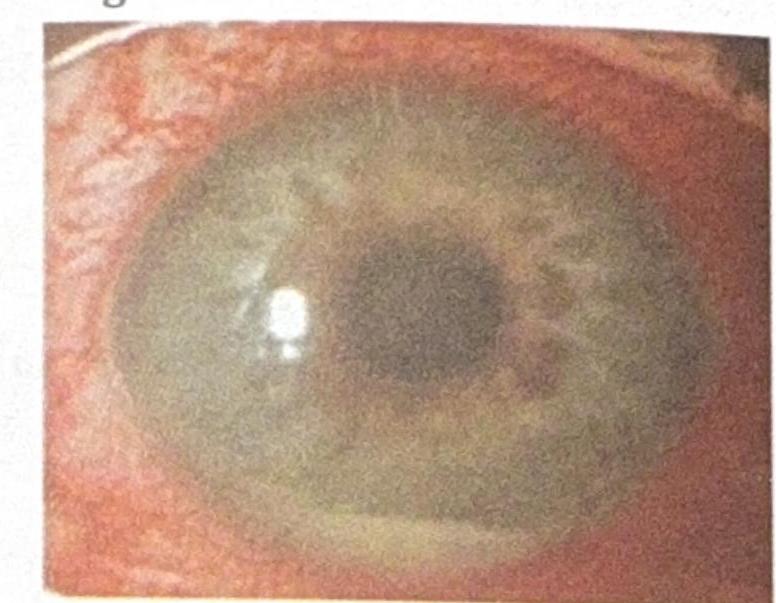
A patient presents with sudden painful diminution of vision, difficulty looking in light (photophobia), and circumcorneal congestion with hypopyon. What is the most likely diagnosis?
A patient presented with gradual loss in night vision and peripheral vision. Based on the fundoscopic image provided, what is the most likely diagnosis?
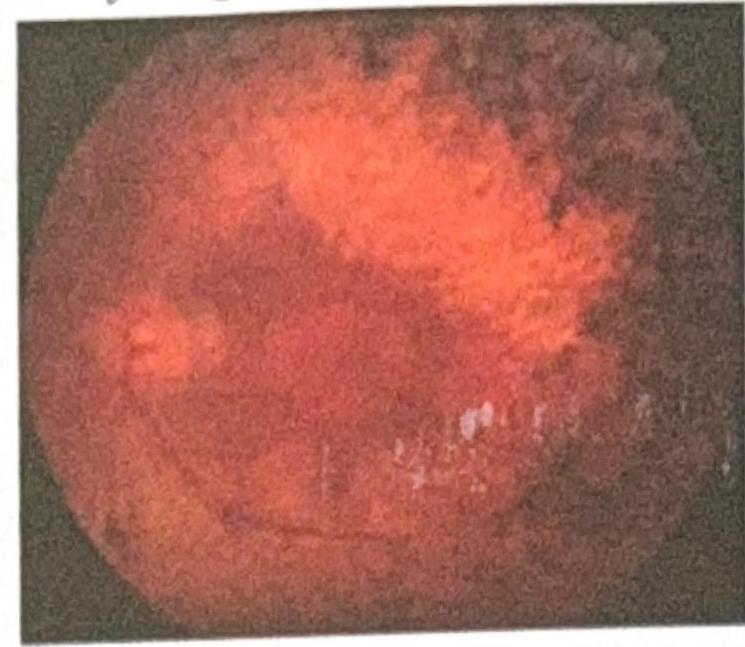
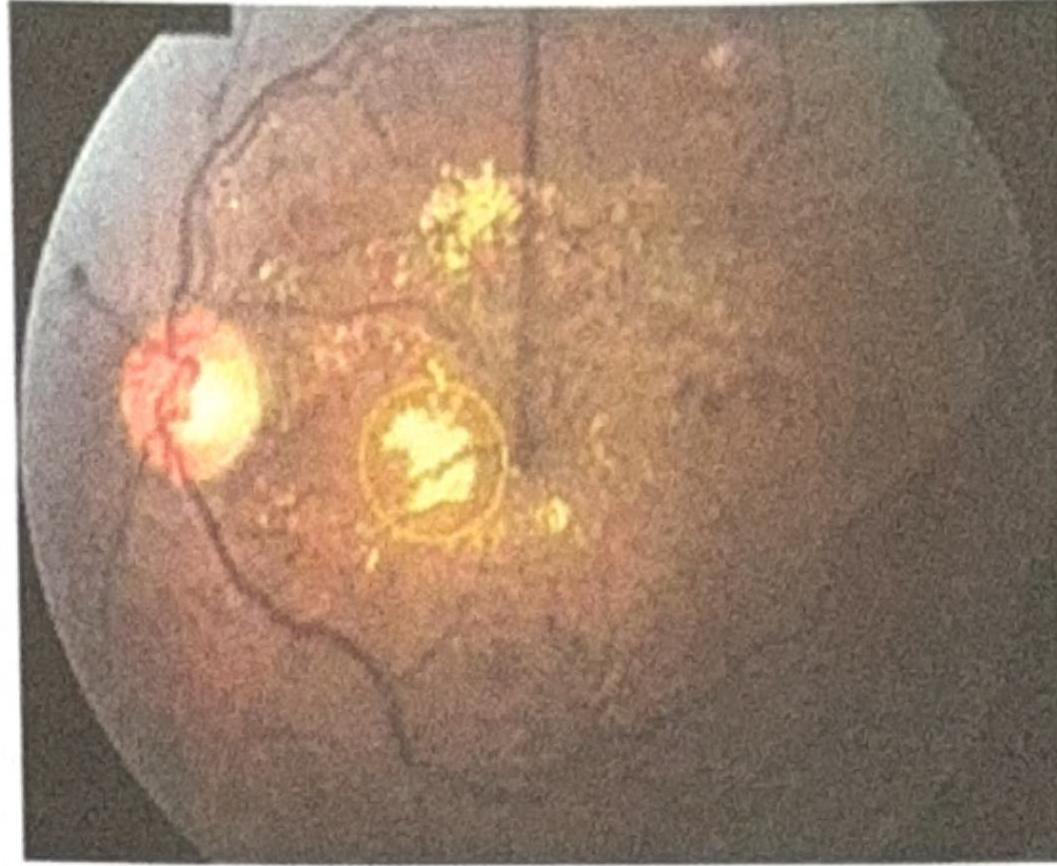
An elderly woman presented with gradual painless diminution of vision. The fundus picture is shown below. What is the most likely diagnosis?
Practice by Chapter
Retinal Anatomy and Physiology
Practice Questions
Age-Related Macular Degeneration
Practice Questions
Diabetic Retinopathy
Practice Questions
Retinal Vascular Diseases
Practice Questions
Retinal Detachment
Practice Questions
Hereditary Retinal Dystrophies
Practice Questions
Inflammatory Retinal Diseases
Practice Questions
Retinal Tumors
Practice Questions
Retinopathy of Prematurity
Practice Questions
Retinal Imaging Techniques
Practice Questions
Intravitreal Pharmacotherapy
Practice Questions
Vitreoretinal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app