
Labor and Delivery — MCQs

On this page
A female patient collapses soon after delivery. There is profuse bleeding and features of disseminated intravascular coagulation. Which of the following is the most likely etiology?
What is the presenting diameter of a fully flexed head?
A 41-week pregnant female, confirmed by radiological investigation and very sure of her last menstrual period, presents with no uterine contractions, no effacement, and no dilatation. Which of the following should not be administered?
Given the following partogram data, identify the most likely diagnosis: Cervical dilation curve shows a prolonged labor with the cervical dilation falling to the right of the alert line.
Which of the following describes the points marked in the diagram of pelvic measurements?

Which of these steps is followed first for the management of shoulder dystocia after McRoberts maneuver?
What does the term 'crowning' refer to in the context of childbirth?
When the fetus is at station +2 and the fetal skull reaches the pelvic floor, which of the following statements is MOST clinically relevant?
What would be the type of presentation when the engaging diameter is mentovertical?
What is the primary clinical advantage of the occipitoanterior position in childbirth?
Labor and Delivery Indian Medical PG Practice Questions and MCQs
Question 1061: A female patient collapses soon after delivery. There is profuse bleeding and features of disseminated intravascular coagulation. Which of the following is the most likely etiology?
- A. Uterine atony
- B. Peripartum cardiomyopathy
- C. Rupture of the uterus during delivery
- D. Amniotic fluid embolism (Correct Answer)
Explanation: ***Amniotic fluid embolism as a complication of pregnancy*** - **Amniotic fluid embolism** is a rare but catastrophic complication where amniotic fluid enters the maternal circulation, leading to sudden **cardiovascular collapse**, **respiratory distress**, and **disseminated intravascular coagulation (DIC)**. - The rapid onset of symptoms after delivery, along with profuse bleeding and features of DIC, is highly characteristic of this condition. *Uterine atony* - **Uterine atony** is the most common cause of **postpartum hemorrhage**, typically leading to profuse bleeding due to the uterus's inability to contract. - While it causes significant bleeding, it does not typically cause the triad of sudden cardiovascular collapse, respiratory distress, and DIC seen in amniotic fluid embolism. *Peripartum cardiomyopathy as a cause of collapse* - **Peripartum cardiomyopathy** can lead to heart failure and cardiovascular collapse, but it typically develops **gradually** in the peripartum period. - It does not directly cause profuse bleeding or DIC; rather, its complications might include thromboembolic events, which are distinct from the primary events described. *Rupture of the uterus during delivery* - **Uterine rupture** causes significant hemorrhage and can lead to maternal collapse. - However, it primarily results in **external or internal bleeding** from the rupture site and does not typically trigger the widespread systemic inflammatory response and DIC as rapidly or profoundly as an amniotic fluid embolism.
Question 1062: What is the presenting diameter of a fully flexed head?
- A. Suboccipito-frontal diameter
- B. Occipito-frontal diameter
- C. Biparietal diameter
- D. Suboccipito-bregmatic diameter (Correct Answer)
Explanation: ***Suboccipito-bregmatic diameter*** - This diameter measures from the **nape of the neck** (**suboccipital region**) to the **anterior fontanelle** (**bregma**), which is the smallest presenting diameter of the fetal head when it is in **full flexion**. - A fully flexed head presents the smallest and most favorable diameter for vaginal birth, allowing for optimal passage through the birth canal. *Suboccipito-frontal diameter* - This diameter is measured from the **nape of the neck to the center of the forehead**, indicating a less flexed head than the suboccipito-bregmatic diameter. - While it represents some flexion, it is not the ideal presenting diameter for a fully flexed head and is larger than the suboccipito-bregmatic diameter. *Occipito-frontal diameter* - This diameter is measured from the **occipital protuberance to the forehead**, representing a **deflexed** or **partially flexed** head. - This presentation is less favorable for vaginal delivery as it is a larger diameter than either the suboccipito-bregmatic or suboccipito-frontal diameters. *Biparietal diameter* - This diameter measures the **widest transverse diameter of the fetal head**, between the two parietal eminences. - While clinically important for assessing head size and growth, it is **not a presenting longitudinal diameter** that describes the leading part of the fetal head during engagement and descent.
Question 1063: A 41-week pregnant female, confirmed by radiological investigation and very sure of her last menstrual period, presents with no uterine contractions, no effacement, and no dilatation. Which of the following should not be administered?
- A. Intracervical foley’s
- B. PGE1 tab
- C. PGE2 gel
- D. PGF2alpha (Correct Answer)
Explanation: ***PGF2alpha*** - **Prostaglandin F2-alpha (carboprost)** is primarily used for **postpartum hemorrhage** and is contraindicated for cervical ripening or labor induction in a live fetus due to its powerful uterotonic effects that can lead to uterine hyperstimulation and fetal distress. - Its mechanism of action involves strong uterine contractions and vasoconstriction, which is not suitable for a routine induction where cervical ripening is the initial goal. *Intracervical foley's* - A **Foley catheter** is a mechanical method for cervical ripening, acting by local pressure to stimulate endogenous prostaglandin release, and is a safe option for an unfavorable cervix. - It does not involve pharmacological agents and is often preferred in situations where prostaglandin use is contraindicated. *PGE1 tab* - **Prostaglandin E1 (misoprostol)** is a synthetic prostaglandin commonly used in tablet form for cervical ripening and labor induction. - It effectively softens and effaces the cervix, and is a widely accepted and safe method for an unfavorable cervix in a 41-week pregnancy. *PGE2 gel* - **Prostaglandin E2 (dinoprostone)**, available as a gel or insert, is a common and effective pharmacological agent for cervical ripening and labor induction. - It works by stimulating direct cervical changes and uterine contractions, which would be indicated in this scenario of an unripe cervix.
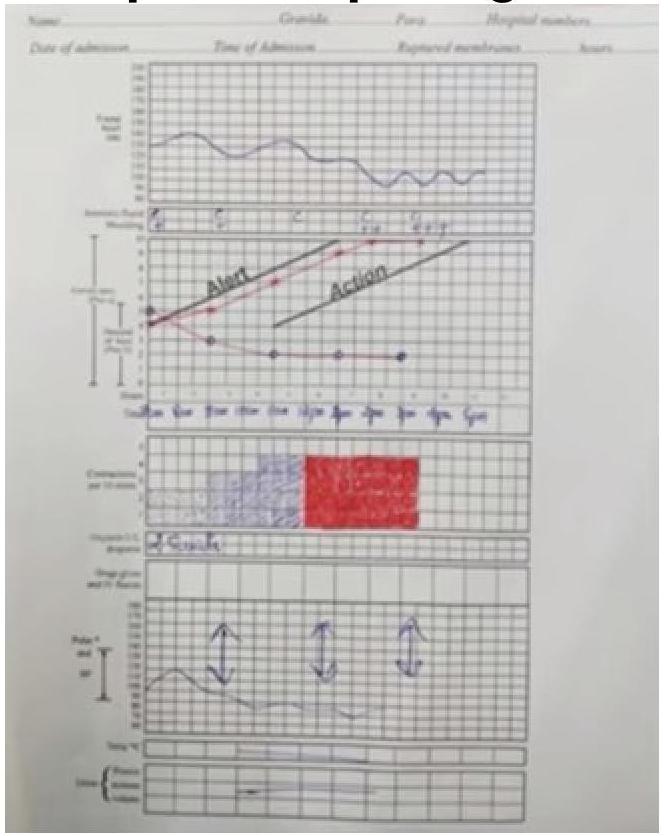
Question 1064: Given the following partogram data, identify the most likely diagnosis: Cervical dilation curve shows a prolonged labor with the cervical dilation falling to the right of the alert line.
- A. Cephalopelvic Disproportion (CPD) (Correct Answer)
- B. Rupture of the uterus during labor
- C. Inadequate uterine contractions
- D. Maternal exhaustion
Explanation: ***Cephalopelvic Disproportion (CPD)*** - A cervical dilation curve that crosses the **alert line** and approaches or crosses the **action line** on a partogram indicates **prolonged labor** or **arrest of labor**. This pattern is highly suggestive of CPD, where the fetal head is too large to pass through the maternal pelvis. - While other factors can cause prolonged labor, CPD is a common cause of **protracted active phase disorders** and **labor arrest**, characterized by a cervix that fails to dilate adequately despite sufficient contractions. *Inadequate uterine contractions* - While inadequate uterine contractions (hypotonic contractions) can lead to **prolonged labor**, the partogram does not provide direct information about the frequency or intensity of contractions to conclusively make this diagnosis. - If contractions were primarily the issue, augmenting labor with oxytocin would be expected to improve the dilation curve, which is not indicated as the primary problem here. *Rupture of the uterus during labor* - Uterine rupture is a catastrophic event typically presenting with sudden **severe pain**, **vaginal bleeding**, **fetal heart rate abnormalities**, and potentially **maternal shock**. - While it can lead to cessation of labor progress, the partogram pattern of a slowly deviating dilation curve over time is not characteristic of an acute uterine rupture. *Maternal exhaustion* - Maternal exhaustion is a common consequence of **prolonged labor** but is not a primary cause of labor arrest or a specific diagnosis reflected by the cervical dilation curve alone. - It often accompanies other underlying issues like CPD or inefficient uterine contractions, rather than being the sole etiology for the observed partogram.
Question 1065: Which of the following describes the points marked in the diagram of pelvic measurements?
- A. Diagonal conjugate (Correct Answer)
- B. Obstetric conjugate measurement
- C. True conjugate measurement
- D. Oblique conjugate measurement
Explanation: ***Diagonal conjugate*** - The image depicts a **bimanual examination** where one hand is inserted vaginally to measure the distance from the **lower border of the pubic symphysis** to the **sacral promontory**. - This measurement directly corresponds to the **diagonal conjugate**, which is a clinically estimated measurement of the pelvic inlet. *Obstetric conjugate measurement* - The **obstetric conjugate** is the smallest anteroposterior diameter through which the fetal head must pass. - It extends from the **middle of the sacral promontory** to the **innermost aspect of the pubic symphysis** and cannot be measured directly by clinical examination. *True conjugate measurement* - The **true conjugate**, also known as the anatomical conjugate, extends from the **sacral promontory** to the **upper border of the pubic symphysis**. - Like the obstetric conjugate, it is not directly palpable and must be estimated from the diagonal conjugate (true conjugate = diagonal conjugate - 1.5 to 2 cm). *Oblique conjugate measurement* - The **oblique conjugate** measures the distance between the sacroiliac joint on one side to the iliopectineal eminence on the opposite side. - This measurement is not typically assessed during a routine pelvic examination as depicted and is more relevant for identifying asymmetric pelvic deformities.
Question 1066: Which of these steps is followed first for the management of shoulder dystocia after McRoberts maneuver?
- A. 90 degree rotation of posterior shoulder
- B. Emergency c-section
- C. Suprapubic pressure (Correct Answer)
- D. Sharp flexion of hip joints towards abdomen
Explanation: ***Suprapubic pressure*** - After performing the **McRoberts maneuver**, applying **suprapubic pressure** is the next step to aid in dislodging the anterior shoulder from behind the pubic symphysis. - This maneuver helps to adduct the fetal shoulders and rotates the anterior shoulder into a more oblique diameter, often allowing for delivery. *90-degree rotation of posterior shoulder* - This describes components of the **Wood's screw maneuver**, which, while effective, is typically attempted *after* suprapubic pressure if initial maneuvers fail. - The Wood's screw maneuver involves rotating the fetal shoulders to disimpact the anterior shoulder, but it is not the *first* step following McRoberts and suprapubic pressure. *Emergency C-section* - An **emergency C-section** is reserved for cases where all other *manual maneuvers* have failed to resolve shoulder dystocia and is not a primary or early step in the management algorithm. - The goal is to first attempt less invasive maneuvers to deliver the baby vaginally, as a C-section carries its own set of risks. *Sharp flexion of hip joints towards abdomen* - This action describes the **McRoberts maneuver** itself, which involves hyperflexing the mother's hips towards her abdomen to flatten the sacrum and rotate the symphysis pubis cephalad. - The question asks for the step *after* McRoberts maneuver, not the maneuver itself.
Question 1067: What does the term 'crowning' refer to in the context of childbirth?
- A. Biparietal diameter at the inlet of pelvis
- B. Biparietal diameter at the ischial spine
- C. Biparietal diameter just outside the vulval outlet
- D. Biparietal diameter at the vulval outlet (Correct Answer)
Explanation: ***Biparietal diameter at the vulval outlet*** - **Crowning** specifically refers to the moment when the largest diameter of the baby's head (the **biparietal diameter**) has passed through the pelvic outlet and becomes visible at the vaginal opening without receding between contractions. - This signifies that the head is fully engaged and will no longer slip back, making birth imminent. *Biparietal diameter at the inlet of pelvis* - The **biparietal diameter** at the inlet of the pelvis describes the initial engagement of the fetal head into the pelvis, which is a much earlier stage than crowning. - This stage is referred to as **engagement**, not crowning, and there is no visible head at this point. *Biparietal diameter at the ischial spine* - The **ischial spines** are a landmark often used to assess the fetal head's station in the pelvis (how far down it has descended). - While important for assessing progress, the biparietal diameter reaching the ischial spines indicates a **station 0**, which is still internal and not visible at the vulva, thus not crowning. *Biparietal diameter just outside the vulval outlet* - If the **biparietal diameter** is **just outside** the vulval outlet, it implies the head has already been born or is so far progressed that crowning has already occurred or the head is delivering. - Crowning specifically describes the moment it becomes visible and sustained at the outlet, not outside it.
Question 1068: When the fetus is at station +2 and the fetal skull reaches the pelvic floor, which of the following statements is MOST clinically relevant?
- A. Forceps may be applied if necessary. (Correct Answer)
- B. Crowning occurs at this stage.
- C. There is a risk of deep transverse arrest.
- D. Episiotomy must be performed at this station.
Explanation: ***Forceps may be applied if necessary.*** - At **station +2**, the fetal head has progressed significantly into the pelvis (2 cm below the ischial spines), indicating a **low-lying head** where instrumental delivery with **forceps** or a **vacuum extractor** can be safely performed if indicated (e.g., maternal exhaustion, fetal distress). - This station qualifies as **low forceps** or **outlet forceps** delivery, which are considered safe procedures when properly indicated. - The fetal head at this level has reached or is approaching the **pelvic floor**, meeting the prerequisites for assisted vaginal delivery. *Crowning occurs at this stage.* - **Crowning** specifically refers to the stage when the largest diameter of the fetal head is visible at the **vaginal introitus** and does not recede between contractions. - This occurs at approximately **station +4 to +5**, not at station +2. - While station +2 indicates significant descent, the fetus must descend further before crowning occurs. *There is a risk of deep transverse arrest.* - **Deep transverse arrest** occurs when the fetal head fails to internally rotate from the transverse position to an occipito-anterior or occipito-posterior position. - This complication typically occurs at **station 0 to +1** (mid-pelvis level), not at station +2. - By the time the fetal head reaches station +2 and the pelvic floor, internal rotation should have already occurred. *Episiotomy must be performed at this station.* - **Episiotomy** is **not mandatory** at any particular fetal station. - It is a selective procedure performed when indicated, typically just before crowning (around station +3 to +4), to prevent severe perineal trauma or expedite delivery. - The decision is based on clinical factors like fetal size, maternal tissue quality, and risk of severe laceration—not solely on fetal station.
Question 1069: What would be the type of presentation when the engaging diameter is mentovertical?
- A. Face
- B. Vertex
- C. Brow (Correct Answer)
- D. Breech
Explanation: ***Brow*** - The **mentovertical diameter** (13.5 cm) is the engaging diameter in **brow presentation**. - This diameter extends from the **chin (mentum) to the vertex** of the fetal head. - Brow presentation occurs when the fetal head is **partially deflexed**, presenting the area between the orbital ridge and the anterior fontanelle. - This is the **largest anteroposterior diameter** of the fetal head and makes vaginal delivery extremely difficult or impossible. *Face* - In **face presentation**, the fetal head is **completely hyperextended**, and the engaging diameter is **submentobregmatic** (9.5 cm), not mentovertical. - This diameter extends from below the chin to the bregma. - Face presentation can allow vaginal delivery if the mentum is anterior. *Vertex* - **Vertex presentation** is the most common and favorable presentation, with the fetal head fully flexed. - The engaging diameter is **suboccipitobregmatic** (9.5 cm), from the subocciput to the bregma. - The occiput presents first in this presentation. *Breech* - **Breech presentation** involves the fetal buttocks or feet presenting first. - The engaging diameter is **bitrochanteric** (transverse diameter), not related to cephalic diameters like mentovertical.
Question 1070: What is the primary clinical advantage of the occipitoanterior position in childbirth?
- A. It is the most favorable position for vaginal delivery.
- B. It allows optimal fetal head flexion reducing the presenting diameter. (Correct Answer)
- C. Anterior fontanelle is anterior in this position.
- D. It is associated with shorter labor duration and fewer complications.
Explanation: ***It allows optimal fetal head flexion reducing the presenting diameter.*** - In the occipitoanterior (OA) position, the fetal head is **well-flexed**, allowing the **smallest diameter** of the fetal head to present to the maternal pelvis - The presenting diameter is the **suboccipitobregmatic diameter** (~9.5 cm), which is the smallest anteroposterior diameter of the fetal head - This optimal flexion is the **primary clinical advantage** as it facilitates easier passage through the birth canal and reduces maternal and fetal trauma - The **occiput (posterior fontanelle)** faces anteriorly in this position, which is a key anatomical landmark used to diagnose OA position during vaginal examination *It is the most favorable position for vaginal delivery.* - While this statement is true, it is **too general** and doesn't explain the specific anatomical or mechanical reason - It describes an outcome rather than explaining the **primary clinical advantage** in terms of fetal head mechanics *Anterior fontanelle is anterior in this position.* - This statement is **anatomically incorrect** - In occipitoanterior position, the **occiput (posterior fontanelle)** is anterior, not the anterior fontanelle - The anterior fontanelle (bregma) is actually positioned **posteriorly** in the OA position *It is associated with shorter labor duration and fewer complications.* - This is a **consequence** of the favorable OA position, not the primary clinical advantage itself - The shorter labor and fewer complications result from the optimal fetal head flexion and smaller presenting diameter - This option describes an **outcome** rather than the underlying anatomical/mechanical advantage
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Start For Free