
Gynecological Disorders — MCQs

On this page
What is the best treatment option for a septate uterus?
45 years female with 3 months of menorrhagia. USG showing 2 cm submucosal fibroid. What is the most appropriate management option?
60-year-old female with a history of intermittent bleeding. What is the diagnosis based on the ultrasound image?

Which of the following treatments is used for vulvar atrophy and itching?
Green frothy vaginal discharge is produced by –
Dilatation & curettage (D&C) is contraindicated in-
What is the most reliable method to confirm the correct placement of a ring pessary in a patient with uterine prolapse?
In a woman complaining of AUB following image was seen in endoscopic examination of uterus. What will be the diagnosis?
What type of uterine anomaly is shown in this X-ray HSG image?

Long-standing pelvic inflammatory disease (PID) may lead to which of the following complications?
Gynecological Disorders Indian Medical PG Practice Questions and MCQs
Question 1121: What is the best treatment option for a septate uterus?
- A. Tompkins Metroplasty
- B. Jones metroplasty
- C. Strassmann metroplasty
- D. Transcervical hysteroscopic resection of the septum (Correct Answer)
Explanation: ***Transcervical hysteroscopic resection of the septum*** - This procedure involves using a **hysteroscope** to visualize and resect the **fibrous or muscular septum** that divides the uterine cavity, restoring a normal uterine shape. - It is considered the gold standard due to its **minimally invasive nature**, effectiveness in improving reproductive outcomes, and lower risk of complications compared to abdominal approaches. *Tompkins Metroplasty* - This is an **abdominal surgical procedure** primarily used for the repair of a **bicornuate uterus**, not typically for a septate uterus. - It involves resecting the uterine fundus to create a single uterine cavity, which is more invasive than hysteroscopic septum resection. *Jones metroplasty* - This procedure is also an **abdominal approach** used for the surgical correction of a **bicornuate uterus**, not a septate uterus. - It involves excising the septal portion and approximating the uterine walls. *Strassmann metroplasty* - This is another **abdominal surgical technique** that is primarily indicated for the repair of a **bicornuate or didelphys uterus**, where a large defect needs to be corrected. - It involves reconstructing the uterus through a fundal incision, which is significantly more invasive than hysteroscopic septal resection for a septate uterus.
Question 1122: 45 years female with 3 months of menorrhagia. USG showing 2 cm submucosal fibroid. What is the most appropriate management option?
- A. Hysteroscopic myomectomy (Correct Answer)
- B. Oral contraceptive pills for symptom management
- C. Progesterone therapy for conservative management
- D. Endometrial biopsy to rule out malignancy
Explanation: **Hysteroscopic myomectomy** - A **2 cm submucosal fibroid** causing **menorrhagia** is best treated with hysteroscopic myomectomy to directly remove the fibroid and resolve the bleeding. - This approach is definitive for symptomatic submucosal fibroids and allows for immediate relief of heavy bleeding. *Oral contraceptive pills for symptom management* - While OCPs can reduce menstrual bleeding, they primarily manage symptoms and do not address the underlying cause, which is the **submucosal fibroid**. - For a **symptomatic submucosal fibroid**, a more definitive treatment is usually preferred over long-term symptom suppression. *Progesterone therapy for conservative management* - Progesterone therapy can help reduce bleeding but also does not remove the **submucosal fibroid** itself. - It is often used for dysfunctional uterine bleeding or smaller fibroids with less severe symptoms, not typically for a 2 cm submucosal fibroid causing significant menorrhagia. *Endometrial biopsy to rule out malignancy* - While ruling out malignancy is important in cases of abnormal uterine bleeding, an **endometrial biopsy** is not the primary treatment for a **submucosal fibroid** identified on USG. - The most appropriate next step given the clear diagnosis is to address the known cause of menorrhagia, which is the fibroid.
Question 1123: 60-year-old female with a history of intermittent bleeding. What is the diagnosis based on the ultrasound image?
- A. Endometrial polyp (Correct Answer)
- B. Ca endometrium
- C. Submucosal fibroid
- D. Endometrial hyperplasia
Explanation: ***Endometrial polyp*** - The ultrasound image shows a well-defined, **echogenic focal lesion within the endometrial cavity**, which is characteristic of an endometrial polyp. - In a 60-year-old female with intermittent bleeding, a polyp is a common cause of **postmenopausal bleeding** and is often identified as an intracavitary mass on ultrasound. - Endometrial polyps appear as **focal, hyperechoic or isoechoic masses** with a smooth contour projecting into the endometrial cavity. *Ca endometrium* - **Endometrial carcinoma** typically appears as diffuse endometrial thickening (>4-5 mm in postmenopausal women), irregular endometrial-myometrial interface, or heterogeneous endometrial echoes, often with evidence of myometrial invasion. - While bleeding is a cardinal symptom of endometrial carcinoma, the distinct **focal, well-circumscribed nature** of the lesion on ultrasound is less typical for carcinoma, which tends to be more diffuse and irregular. *Submucosal fibroid* - A **submucosal fibroid** (leiomyoma) is a benign smooth muscle tumor originating from the myometrium that protrudes into the endometrial cavity. - While it can appear as an intracavitary mass and cause abnormal bleeding, fibroids often have a more **heterogeneous or hypoechoic appearance** with posterior acoustic shadowing, compared to the isoechoic to hyperechoic appearance of a polyp. - The feeding vessel sign (blood flow at the base) is more characteristic of polyps than fibroids. *Endometrial hyperplasia* - **Endometrial hyperplasia** presents as **diffuse, uniform endometrial thickening** rather than a focal intracavitary mass. - It typically shows homogeneous increased echogenicity of the entire endometrium without a discrete, well-defined lesion as seen with a polyp. - While it can cause postmenopausal bleeding, the focal nature of the lesion in this case makes hyperplasia less likely.
Question 1124: Which of the following treatments is used for vulvar atrophy and itching?
- A. Estrogen ointment (Correct Answer)
- B. Antihistamines
- C. Tamoxifen
- D. None of the options
Explanation: ***Estrogen ointment*** * **Estrogen ointment** is the primary treatment for vulvar atrophy and itching because it directly addresses the underlying cause of these symptoms, which is the decline in estrogen levels after **menopause**. * By restoring estrogen to the vulvar tissues, it helps to **thicken the epithelium**, improve blood flow, and increase lubrication, thereby alleviating dryness, itching, and discomfort. *Antihistamines* * **Antihistamines** are used to treat allergic reactions and reduce itching associated with conditions like hives or insect bites, but they do not address the hormonal deficiency causing vulvar atrophy. * While they might temporarily relieve some itching, they do not treat the underlying **tissue thinning** and dryness characteristic of vulvar atrophy. *Tamoxifen* * **Tamoxifen** is a selective estrogen receptor modulator (SERM) primarily used in the treatment and prevention of breast cancer, as it blocks estrogen's effects in breast tissue. * However, in vulvovaginal tissues, **tamoxifen can actually worsen atrophy and dryness** due to its anti-estrogenic effects, making it an inappropriate treatment for vulvar atrophy. *None of the options* * This option is incorrect because **estrogen ointment** is a well-established and effective treatment specifically designed to address vulvar atrophy and associated itching, by restoring estrogen levels to the affected tissues.
Question 1125: Green frothy vaginal discharge is produced by –
- A. Herpes simplex
- B. Candida albicans
- C. Trichomonas vaginalis (Correct Answer)
- D. Normal vaginal flora
Explanation: ***Trichomonas vaginalis*** - **Trichomoniasis**, caused by *Trichomonas vaginalis*, classically presents with a **yellowish-green, frothy, malodorous vaginal discharge**. - It is a **sexually transmitted infection** that can also cause vaginal itching, burning, and dyspareunia. *Herpes simplex* - Herpes simplex virus typically causes **painful genital ulcers** or sores, not a frothy discharge. - The discharge, if present, is usually clear or serous and associated with the open lesions. *Candida albicans* - *Candida albicans* (yeast infection) commonly produces a **thick, white, "cottage cheese-like" discharge** that is often associated with intense itching. - It does not typically cause a frothy, green discharge. *Normal vaginal flora* - Normal vaginal flora maintains a healthy vaginal environment and produces a **clear to whitish, non-irritating discharge** with no strong odor. - It does not cause a green, frothy discharge, which indicates an infection.
Question 1126: Dilatation & curettage (D&C) is contraindicated in-
- A. Pelvic inflammatory disease (PID) (Correct Answer)
- B. Endometriosis
- C. Ectopic pregnancy
- D. Abnormal uterine bleeding
Explanation: ***Pelvic inflammatory disease (PID)*** - D&C is **contraindicated** in PID due to the high risk of **spreading pre-existing infection** from the cervix or vagina into the sterile uterine cavity and beyond. - This procedure can worsen the infection, potentially leading to **sepsis**, **tubo-ovarian abscesses**, or chronic pain. *Endometriosis* - D&C is not typically contraindicated in **endometriosis**, as it is sometimes used diagnostically to rule out other causes of abnormal uterine bleeding, though it isn't a treatment for endometriosis itself. - Endometriosis involves the presence of **endometrial tissue outside the uterus**, and a D&C performed on the uterus does not directly exacerbate this condition. *Ectopic pregnancy* - D&C is not contraindicated in **ectopic pregnancy**; however, it is not the primary treatment. - A D&C may be performed if the diagnosis of ectopic pregnancy is uncertain and to rule out an **intrauterine pregnancy** or retained products of conception. *Abnormal uterine bleeding* - D&C is frequently indicated and can be both **diagnostic and therapeutic** for abnormal uterine bleeding, especially to investigate causes like polyps, fibroids, or endometrial hyperplasia. - It helps in obtaining tissue for **histopathological examination** to guide further management.
Question 1127: What is the most reliable method to confirm the correct placement of a ring pessary in a patient with uterine prolapse?
- A. If there is no bleeding observed
- B. If the patient reports discomfort
- C. If the ring is not visible externally
- D. If it remains in place after increased abdominal pressure (Correct Answer)
Explanation: ***If it remains in place after increased abdominal pressure*** - The most reliable method to confirm correct placement is to ensure the pessary **stays in position** when the patient coughs, strains, or performs a Valsalva maneuver, mimicking increased **intra-abdominal pressure**. - This maneuver confirms that the pessary is adequately supported by the **levator ani muscles** and the vaginal walls, preventing expulsion during daily activities. *If there is no bleeding observed* - While absence of bleeding is a good sign for immediate mucosal integrity, it does not confirm the **mechanical stability** of the pessary or its ability to support the prolapse long-term. - Bleeding can be a sign of improper fit or erosion, but its absence alone isn't a definitive indicator of correct placement. *If the patient reports discomfort* - Discomfort can indicate **improper fit**, too large a pessary, or even correct placement if the patient is unaccustomed to it. Therefore, discomfort is a poor indicator of correct placement. - A correctly placed pessary should generally be **unnoticeable** by the patient, though mild initial awareness can occur. *If the ring is not visible externally* - Not being visible externally indicates that the pessary is **internalized**, but this alone does not confirm that it is adequately supporting the uterus or that it will remain in place during activities that increase abdominal pressure. - A pessary can be inside the vagina but still be **improperly positioned** or sized to effectively manage the prolapse.
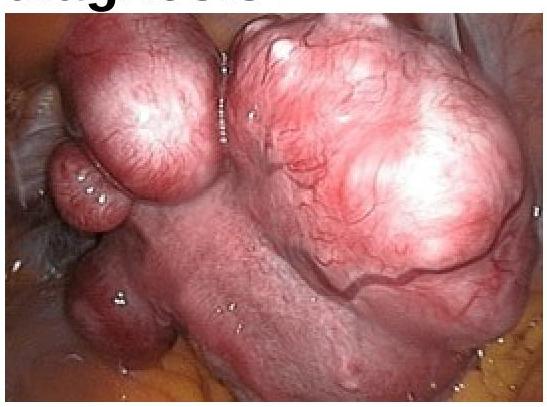
Question 1128: In a woman complaining of AUB following image was seen in endoscopic examination of uterus. What will be the diagnosis?
- A. Leiomyoma (Correct Answer)
- B. Adenomyosis
- C. Ovarian neoplasm
- D. Carcinoma of uterus
Explanation: ***Leiomyoma*** - The image shows **well-circumscribed, smooth, rounded masses protruding into the uterine cavity**, which are characteristic of **submucous (intracavitary) leiomyomas (fibroids)** seen on hysteroscopy. - Submucous leiomyomas are benign smooth muscle tumors that project into the endometrial cavity and commonly cause **abnormal uterine bleeding (AUB)** due to increased endometrial surface area, distortion of the endometrial cavity, ulceration of overlying endometrium, and interference with normal uterine contractility. - On **hysteroscopic examination**, they appear as firm, pale, smooth-surfaced masses with overlying endometrium. *Adenomyosis* - Adenomyosis involves the presence of **endometrial tissue within the myometrium**, leading to diffuse uterine enlargement. - On hysteroscopy, it may show a **globally irregular endometrial surface** with small endometrial openings or cystic spaces, but not the discrete, well-circumscribed protruding masses seen in the image. - While it can cause AUB and dysmenorrhea, the appearance is distinctly different from submucous leiomyomas. *Ovarian neoplasm* - Ovarian neoplasms originate in the **ovaries**, which are separate from the uterus. - **Hysteroscopic examination** visualizes only the **endometrial cavity** and cannot directly visualize ovarian pathology. - Ovarian masses do not protrude into the uterine cavity. *Carcinoma of uterus* - Endometrial carcinoma typically presents on hysteroscopy as **irregular, friable, ulcerative, or fungating lesions** with abnormal vascularity and易出血 (easy bleeding). - The **smooth, well-defined, and rounded appearance** with intact overlying mucosa in the image is characteristic of benign leiomyomas, not malignant growths. - Uterine sarcomas are rare and would show more irregular, infiltrative features rather than well-circumscribed masses.
Question 1129: What type of uterine anomaly is shown in this X-ray HSG image?
- A. Septate uterus
- B. Uterus didelphys
- C. Unicornuate uterus (Correct Answer)
- D. Bicornuate uterus
Explanation: ***Unicornuate uterus*** - The image shows a single, elongated uterine horn with a single fallopian tube arising from it, consistent with a **unicornuate uterus**. - This congenital anomaly results from the **failure of one Müllerian duct to develop**, leading to an abnormally shaped uterus. *Septate uterus* - A **septate uterus** would show a normal uterine fundus with an internal septum dividing the uterine cavity. - This image clearly depicts only **one rudimentary horn** and no visible septum. *Uterus didelphys* - **Uterus didelphys** involves two completely separate uteri, each with its own cervix and vagina. - The image does not show evidence of a **second, separate uterine structure**. *Bicornuate uterus* - A **bicornuate uterus** is characterized by two distinct uterine horns, which fuse at the cervix or lower uterine segment, creating a heart-shaped appearance of the fundus. - The image shows a **single, long horn** rather than two distinct horns.
Question 1130: Long-standing pelvic inflammatory disease (PID) may lead to which of the following complications?
- A. Uterine polyposis
- B. Hydrosalpinx (Correct Answer)
- C. Endometriosis
- D. Asherman syndrome
Explanation: ***Hydrosalpinx*** - **Hydrosalpinx** is a condition where the fallopian tube is blocked and filled with serous fluid, representing the **end-stage of chronic pelvic inflammatory disease (PID)**. - Chronic inflammation from **repeated or inadequately treated PID** causes damage to the tubal epithelium, loss of fimbrial function, and **adhesions that seal the distal end of the tube**. - This leads to accumulation of sterile transudate within the obstructed tube, creating a **fluid-filled, dilated fallopian tube**. - It is a major cause of **tubal factor infertility** and increased risk of **ectopic pregnancy**. - Classic imaging finding: **sausage-shaped cystic structure** on ultrasound. *Uterine polyposis* - **Endometrial polyps** are benign growths arising from the endometrium, typically associated with **unopposed estrogen stimulation** or hormonal imbalances. - They are **not a complication of chronic PID** but rather a proliferative endometrial disorder. - Common causes include obesity, tamoxifen use, and perimenopause. *Asherman syndrome* - **Asherman syndrome** involves **intrauterine adhesions** (synechiae) causing partial or complete obliteration of the uterine cavity. - It typically results from **endometrial trauma** following procedures like **D&C (dilatation and curettage)**, particularly post-abortion or postpartum curettage. - While PID can cause adhesions, Asherman syndrome specifically refers to **intrauterine** adhesions, not a typical sequela of chronic PID, which primarily affects the **tubes and ovaries**. *Endometriosis* - **Endometriosis** is the presence of **endometrial tissue outside the uterine cavity**, most commonly on ovaries, pelvic peritoneum, and uterosacral ligaments. - It is thought to result from **retrograde menstruation** (Sampson's theory) and genetic/immune factors. - It is **not caused by PID** but is a distinct pathological entity with different etiology and pathophysiology.
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Start For Free