
Gynecological Disorders — MCQs

On this page
Where are Gartner's cysts typically located?
What factor is associated with decreased success in the medical management of ectopic pregnancy?
What is the treatment of choice for a Bartholin cyst?
In your STI clinic, standardized treatment kits are available for different conditions based on clinical presentation and likely pathogens. A 22-year-old female comes to the STI clinic with minimal vaginal discharge. On speculum examination, erosions are seen on the cervix. Which of the following treatment kit should be given to this patient?
A 16-year-old girl presents with cyclical pelvic pain every month. She has not achieved menarche yet. On examination, a suprapubic bulge can be seen in the lower abdomen. PR examination reveals a bulging swelling in the anterior aspect. What is the most likely diagnosis?
A woman comes with complaints of pain and swelling in the perineal area. She also has complaints of difficulty in walking and sitting. She gives a history of multiple sexual partners. On examination, a tender swelling is seen with redness on the labia. What is the most likely diagnosis?
Identify the type of hymen.
A mother brought her 16-year-old daughter to Gynaecology OPD with a complaint of not attending menarche. She gives a history of cyclic abdominal pain. On further examination, a midline abdominal swelling is seen. Per rectal examination reveals a bulging mass in the vaginal area. Which of the following can be most commonly seen?
A 30-year-old woman presents with complaints of dysmenorrhea and dyspareunia, accompanied by chronic pelvic pain. She undergoes a hysterectomy. Based on the cut section of the hysterectomy specimen provided, identify the condition.
A sexually active female presenting with profuse frothy foul-smelling discharge with intense itching. Strawberry cervix revealed on examination. What will be the diagnosis?
Gynecological Disorders Indian Medical PG Practice Questions and MCQs
Question 1111: Where are Gartner's cysts typically located?
- A. Anterolateral vaginal wall (Correct Answer)
- B. Anterolateral cervix
- C. Posterolateral vaginal wall
- D. Posterolateral cervix
Explanation: ***Anterolateral vaginal wall*** - **Gartner's cysts** are remnants of the **mesonephric (Wolffian) duct**. - These ducts primarily run along the **anterolateral vaginal wall**, which is their typical location. *Anterolateral cervix* - While located in the gynecological tract, the **cervix** is not the primary site for remnants of the **mesonephric duct**. - Cysts in this area are more commonly **Nabothian cysts**, which are retention cysts of cervical glands. *Posterolateral vaginal wall* - The **mesonephric duct** remnants, from which Gartner's cysts arise, typically course along the **anterior** rather than the posterior vaginal wall. - Cysts in the posterolateral wall are more likely to be **inclusion cysts** or related to the **Bartholin's glands**. *Posterolateral cervix* - Similar to the anterolateral cervix, this location is not typical for **Gartner's cysts**. - Cysts found here are likely to have a different embryological origin or pathological basis.
Question 1112: What factor is associated with decreased success in the medical management of ectopic pregnancy?
- A. Gestational sac > 3cm
- B. Beta HCG > 5000 IU/L (Correct Answer)
- C. Duration of gestation > 5 weeks
- D. Cardiac activity absent
Explanation: ***Beta HCG > 5000 IU/L*** - A **beta-hCG level greater than 5000 IU/L** is a well-established **relative contraindication** for medical management with methotrexate. - High beta-hCG levels indicate a **larger ectopic mass with higher metabolic activity**, which significantly increases the risk of **treatment failure** and need for surgical intervention. - Most protocols recommend **surgical management** when beta-hCG exceeds 5000 IU/L due to decreased success rates with methotrexate. *Gestational sac > 3cm* - While a **large ectopic mass** (typically > 3.5-4 cm) is associated with lower success rates, the cutoff varies across guidelines. - Ectopic mass size is a relative contraindication, but **beta-hCG level** is a more standardized and objectively measurable criterion used in clinical protocols. *Duration of gestation > 5 weeks* - The **duration of gestation alone** is not a primary determinant of medical management success. - Other factors like **beta-hCG levels, mass size, and cardiac activity** are more critical in determining suitability for medical management. *Cardiac activity absent* - **Absence of cardiac activity** is actually a **favorable prognostic factor** for medical management, indicating a non-viable pregnancy with lower metabolic activity. - Medical management is often **contraindicated** when **fetal cardiac activity is present**, as it indicates a more viable and metabolically active pregnancy with higher failure risk.
Question 1113: What is the treatment of choice for a Bartholin cyst?
- A. Aspiration
- B. Observe
- C. Curettage and closure
- D. Marsupialization (Correct Answer)
Explanation: ***Marsupialization*** - **Marsupialization** is the gold standard for Bartholin cysts because it creates a permanent opening for drainage, preventing recurrence. - This procedure involves incising the cyst, draining its contents, and then suturing the cyst walls to the surrounding skin, forming a **self-draining pouch**. *Aspiration* - **Aspiration** is generally not recommended as a primary treatment because it offers only temporary relief and has a high rate of recurrence. - The cyst will likely refill without a permanent drainage pathway, making it an ineffective long-term solution. *Observe* - **Observation** is only appropriate for very small, asymptomatic cysts that do not cause any discomfort or pain. - For symptomatic cysts, intervention is necessary to alleviate symptoms and prevent complications like infection. *Curettage and closure* - **Curettage and closure** is not a standard treatment for Bartholin cysts and would likely lead to immediate recurrence. - Simply excising the cyst without creating a new drainage duct for the Bartholin gland would result in the gland's continued blockage and cyst formation.
Question 1114: In your STI clinic, standardized treatment kits are available for different conditions based on clinical presentation and likely pathogens. A 22-year-old female comes to the STI clinic with minimal vaginal discharge. On speculum examination, erosions are seen on the cervix. Which of the following treatment kit should be given to this patient?
- A. Green
- B. Red
- C. Grey (Correct Answer)
- D. Yellow
Explanation: ***Grey*** - A grey kit is indicated for **vaginal discharge** with associated **cervical erosions**, suggesting a treatable bacterial STI like gonorrhea or chlamydia. This kit typically contains antibiotics effective against these pathogens. - The presence of **minimal vaginal discharge** combined with **cervical erosions** points towards cervicitis, for which the grey kit is specifically designed. *Green* - The green kit is typically for the treatment of **vaginal discharge** without specific signs of cervicitis, often targeting common causes like **bacterial vaginosis** or **trichomoniasis**. - It would not specifically address the **cervical erosions** seen in this patient, which are more indicative of cervicitis. *Red* - The red kit is generally used for the treatment of **genital ulcers**, which are typically caused by **herpes simplex virus** or **syphilis**. - While there are erosions, the primary complaint is discharge, and erosions are not typically the sole indicator for a "genital ulcer" kit. *Yellow* - The yellow kit is often designated for **urethral discharge** in males, addressing conditions like **gonorrhea** or **chlamydia** when presenting as urethritis. - This patient is female and presents with **vaginal discharge** and **cervical erosions**, making the yellow kit inappropriate.
Question 1115: A 16-year-old girl presents with cyclical pelvic pain every month. She has not achieved menarche yet. On examination, a suprapubic bulge can be seen in the lower abdomen. PR examination reveals a bulging swelling in the anterior aspect. What is the most likely diagnosis?
- A. Transverse vaginal septum
- B. Vaginal atresia
- C. Imperforate hymen (Correct Answer)
- D. Cervical agenesis
Explanation: ***Imperforate hymen*** - The combination of **cyclical pelvic pain** without menarche (primary amenorrhea) and a **suprapubic bulge** with **bulging swelling on PR examination** strongly suggests an imperforate hymen. - This condition leads to the **accumulation of menstrual blood (hematocolpos)**, causing the observed swelling and pain. - Imperforate hymen is the **most distal obstruction** of the female genital tract, presenting with a characteristic **bulging membrane at the vaginal opening**. *Transverse vaginal septum* - This condition also causes **primary amenorrhea** and **hematocolpos** leading to cyclical pain. - However, a transverse vaginal septum is located **higher in the vagina** (not at the introitus) and would not typically present with such an obvious **bulging swelling on examination** at the vaginal opening. *Vaginal atresia* - **Vaginal atresia** involves the complete or partial absence of the vagina, which would prevent menarche and cause cyclical pain. - While it results in hematocolpos (if the uterus is present), the presentation differs from the classic **bulging membrane** seen with imperforate hymen. *Cervical agenesis* - **Cervical agenesis** is the congenital absence or incomplete formation of the cervix, leading to **primary amenorrhea** and severe cyclical pain due to retained menstrual blood in the uterus (**hematometra**). - This condition would not present with a **bulging mass on PR examination** at the vaginal level, but rather with an enlarged uterus above, as the obstruction is at the cervical level, not at the vaginal outlet.
Question 1116: A woman comes with complaints of pain and swelling in the perineal area. She also has complaints of difficulty in walking and sitting. She gives a history of multiple sexual partners. On examination, a tender swelling is seen with redness on the labia. What is the most likely diagnosis?
- A. Chlamydial infection
- B. Bartholin abscess (Correct Answer)
- C. Genital Tuberculosis
- D. Herpes infection
Explanation: ***Bartholin abscess*** - The presentation of **painful, tender swelling with redness** on the labia, especially causing difficulty in walking and sitting, is classic for a **Bartholin gland abscess**. - **Multiple sexual partners** can increase the risk of infection leading to abscess formation due to bacterial contamination. *Chlamydial infection* - While Chlamydia is a sexually transmitted infection, it typically manifests as **cervicitis**, **urethritis**, or pelvic inflammatory disease, often with a discharge. - It does not directly cause an acute, localized labial abscess as described. *Genital Tuberculosis* - Genital tuberculosis is a **chronic condition** that usually presents with menstrual irregularities, infertility, or chronic pelvic pain. - It rarely causes an acute, tender labial swelling or abscess. *Herpes infection* - Genital herpes presents with **painful vesicles or ulcers** on the genitalia, often associated with a prodrome of itching or tingling. - It does not typically cause a single, large, tender, and red fluctuant swelling indicative of an abscess.
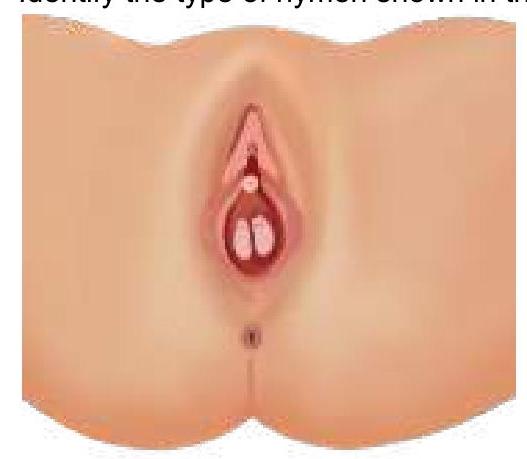
Question 1117: Identify the type of hymen.
- A. Imperforate hymen
- B. Semilunar hymen
- C. Septate hymen (Correct Answer)
- D. Annular hymen
Explanation: ***Septate hymen*** - The image clearly displays a **band of tissue** running across the hymenal opening, dividing it into two smaller openings, which is characteristic of a **septate hymen**. - This type of hymen can sometimes interfere with menstruation or intercourse and may require surgical correction. *Imperforate hymen* - An **imperforate hymen** completely covers the vaginal opening, with no perforations for menstrual flow. - This typically presents at menarche with **abdominal pain** and a bulging hymen due to retained menstrual blood (hematocolpos). *Semilunar hymen* - A **semilunar hymen** is incomplete, forming a crescent shape at the posterior aspect of the vaginal opening. - This is a common and normal variant, usually not causing any clinical issues. *Annular hymen* - An **annular hymen** is characterized by a circular opening in the center, encircled by hymenal tissue, appearing like a ring. - This is a common hymenal configuration and usually allows for normal menstrual flow.
Question 1118: A mother brought her 16-year-old daughter to Gynaecology OPD with a complaint of not attending menarche. She gives a history of cyclic abdominal pain. On further examination, a midline abdominal swelling is seen. Per rectal examination reveals a bulging mass in the vaginal area. Which of the following can be most commonly seen?
- A. Congenital obstruction of the vaginal opening due to hymenal anomaly. (Correct Answer)
- B. Congenital transverse partition in the vaginal canal.
- C. Congenital absence of uterus and upper vagina.
- D. Absence of vaginal development.
Explanation: ***Congenital obstruction of the vaginal opening due to hymenal anomaly*** - This is the most common cause of **congenital vaginal outflow obstruction** presenting in adolescent girls - The classic triad of **primary amenorrhea**, **cyclic abdominal pain**, and **palpable pelvic/abdominal mass** points to **imperforate hymen with hematocolpos** - The **bulging mass on per rectal examination** is pathognomonic, representing accumulated menstrual blood distending the vagina - Cyclic pain occurs due to uterine contractions against the obstruction during attempted menstruation - Treatment involves **cruciate incision of the hymen** to release the accumulated blood *Congenital transverse partition in the vaginal canal* - Transverse vaginal septum can present similarly but is **much less common** than imperforate hymen - The septum is typically located at the **junction of upper and middle third** of the vagina - The bulging mass on per rectal examination is **more characteristic of distal obstruction** (imperforate hymen) rather than a mid-vaginal septum - Would require **surgical excision** rather than simple cruciate incision *Congenital absence of uterus and upper vagina* - **Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome** presents with primary amenorrhea but **NO cyclic pain** - Absence of functional uterus means **no menstrual blood production**, hence no hematocolpos or bulging mass - Patients have normal ovaries and secondary sexual characteristics but absent uterus and upper 2/3 of vagina - Per rectal examination would reveal **absent uterus**, not a bulging mass *Absence of vaginal development* - **Vaginal agenesis** is usually part of MRKH syndrome spectrum - Would **NOT present with cyclic abdominal pain** as there is no functional endometrium to shed - **No accumulation of menstrual blood** occurs, so no palpable mass or vaginal bulging - The presence of cyclic symptoms indicates a **patent uterus with obstructed outflow**, ruling out this diagnosis
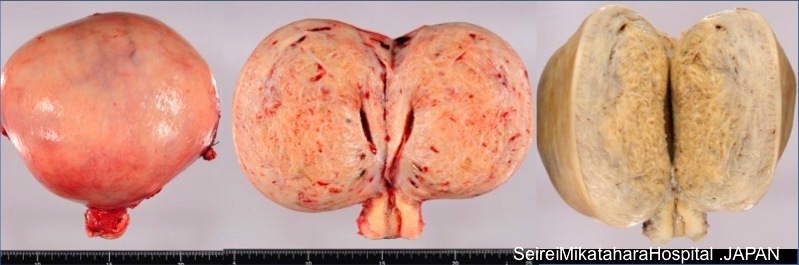
Question 1119: A 30-year-old woman presents with complaints of dysmenorrhea and dyspareunia, accompanied by chronic pelvic pain. She undergoes a hysterectomy. Based on the cut section of the hysterectomy specimen provided, identify the condition.
- A. Adenomyosis (Correct Answer)
- B. Endometrial hyperplasia
- C. Uterine leiomyoma
- D. Endometriosis
Explanation: ***Adenomyosis*** - The image depicts a **thickened uterine wall** with poorly demarcated, **whorled or trabeculated areas** within the myometrium, often containing small blood or fluid-filled cysts, which are characteristic macroscopic findings in adenomyosis. - The clinical presentation of **dysmenorrhea**, **dyspareunia**, and **chronic pelvic pain** is highly consistent with adenomyosis, where endometrial tissue invades the muscular wall of the uterus. - The diffuse involvement of the myometrium without discrete masses is pathognomonic for adenomyosis. *Endometrial hyperplasia* - Endometrial hyperplasia involves **excessive proliferation of endometrial glands** and stroma within the endometrial cavity, not invasion into the myometrium. - It typically presents with **abnormal uterine bleeding** rather than the dysmenorrhea and pelvic pain seen here. - The cut section would show a **thickened endometrium** rather than myometrial involvement. *Uterine leiomyoma* - Uterine leiomyomas (fibroids) are benign smooth muscle tumors that present as **discrete, well-demarcated, firm, rubbery masses** within or protruding from the myometrium. - The macroscopic appearance in the image, characterized by a diffuse, poorly circumscribed involvement of the myometrial wall, is inconsistent with leiomyoma. - Leiomyomas have a **whorled, white-tan cut surface** that is sharply demarcated from surrounding tissue. *Endometriosis* - Endometriosis involves the presence of **endometrial tissue outside the uterus**, such as on the ovaries, peritoneum, or other pelvic organs. - While it can cause similar symptoms (dysmenorrhea, dyspareunia, chronic pelvic pain), the image provided shows the **cut section of a hysterectomy specimen**, indicating a condition *within* the uterine wall, not external implants. - Endometriosis would not show the characteristic myometrial thickening and trabeculation seen in adenomyosis.
Question 1120: A sexually active female presenting with profuse frothy foul-smelling discharge with intense itching. Strawberry cervix revealed on examination. What will be the diagnosis?
- A. Trichomonas vaginalis (Correct Answer)
- B. Bacterial vaginosis
- C. Candidiasis
- D. None of the options
Explanation: **Trichomonas vaginalis** - The classic presentation of **profuse, frothy, foul-smelling vaginal discharge** with **intense itching** and the presence of a **strawberry cervix** are highly characteristic of a *Trichomonas vaginalis* infection. - *Trichomonas vaginalis* is a **motile protozoan** and a common sexually transmitted infection. *Bacterial vaginosis* - While bacterial vaginosis (BV) causes a **foul-smelling discharge** (often described as "fishy"), it is typically **thin and grayish-white**, not frothy, and does not cause a strawberry cervix. - BV is caused by an **overgrowth of anaerobic bacteria** and a decrease in lactobacilli, leading to an elevated vaginal pH. *Candidiasis* - Candidiasis (yeast infection) presents with a **thick, white, "cottage cheese-like" discharge** and intense itching, but the discharge is usually odorless and it does not cause a frothy discharge or strawberry cervix. - It is caused by an **overgrowth of *Candida* species**, primarily *Candida albicans*, and is not typically sexually transmitted. *None of the options* - Given the classic constellation of symptoms and definitive signs, a specific diagnosis can be made, making this option incorrect.
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Start For Free