
Infectious Diseases — MCQs

On this page
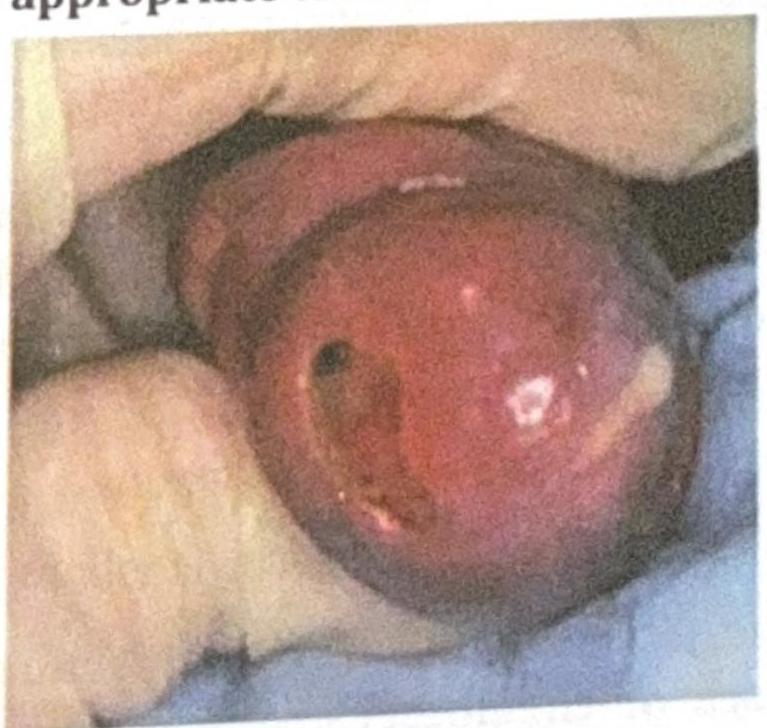
An adult man presents with the clinical condition shown in the image, and a Gram stain reveals Gram-negative diplococci. What is the most appropriate treatment?
A 25-year-old woman with HIV (CD4 count 320/μL) presents with vulvar ulceration for 3 weeks. Initial testing for HSV, syphilis, and chancroid is negative. Empiric treatment for these conditions does not improve the lesion. Biopsy shows a dense lymphoplasmacytic infiltrate with CMV inclusions. What is the most appropriate management?
A 28-year-old man presents with recurrent urethritis despite appropriate treatment for gonorrhea and chlamydia. NAAT tests for both are negative. He reports adherence to therapy and denies reexposure. What is the most appropriate next step?
Which of the following best predicts the need for lumbar puncture in a patient with syphilis?
A 30-year-old woman presents with dysuria, urinary frequency, and lower abdominal pain for 3 days. She has a new sexual partner. On examination, she has suprapubic tenderness but no cervical motion tenderness or vaginal discharge. Urine dipstick shows positive leukocyte esterase but negative nitrites. Microscopy reveals numerous WBCs but no bacteria. What is the most likely diagnosis and appropriate management?
A 27-year-old HIV-positive man (CD4 count 250/μL) presents with a 2-month history of perianal ulcer that is painless, clean-based, and indurated. Dark field microscopy and PCR for HSV are negative. VDRL is 1:64, and TPHA is positive. Lumbar puncture shows 30 WBCs (predominantly lymphocytes) and CSF-VDRL is reactive. Despite receiving standard benzathine penicillin therapy 2 weeks ago, the ulcer persists unchanged. What is the most appropriate next step?
A 22-year-old man presents with urethral discharge and dysuria for 3 days. Gram stain shows intracellular gram-negative diplococci. Two weeks after appropriate treatment, he returns with similar symptoms. Repeat testing shows no organisms on Gram stain but leukocytes are present. What is the most likely explanation?
How does HIV infection alter the natural history of syphilis?
A patient living with HIV presents with foulsmelling stools. Microscopic examination of the stool reveals no cysts or ova, but a 200-micrometer larva is observed. What is the most likely pathogen?
A farmer presents with severe leg pain, fever, chills, retro-orbital pain, and bilateral conjunctival suffusion. What is the most likely diagnosis?
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app