
Infectious Diseases — MCQs

On this page
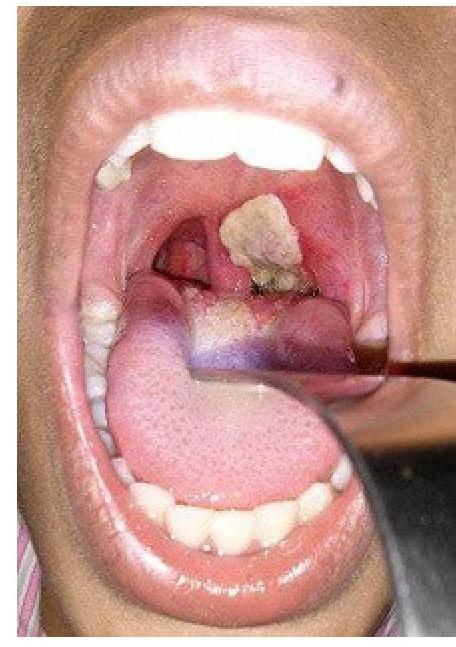
A patient presents with hoarseness of voice and a clinical condition as shown in the image. Identify the lesion:
Which virus is typically associated with serpiginous ulcers in the distal esophagus?
Which of the following conditions is least associated with HIV infection?
What are the essential major blood culture criteria for diagnosing infective endocarditis?
Punched out ulcers in the esophagus are most commonly associated with which of the following conditions?
After 4 months of renal transplantation, which infection is most likely to develop?
A patient complains about painful blisters around the angle of mouth, identify the pathogen
Which condition is most commonly associated with cryoglobulinemia?
Which is not included in AIDS related complex?
A boy presented with multiple non suppurative osteomyelitis with sickle cell anaemia. What will be the causative organism?
Infectious Diseases Indian Medical PG Practice Questions and MCQs
Question 1181: A patient presents with hoarseness of voice and a clinical condition as shown in the image. Identify the lesion:
- A. Diphtheria (Correct Answer)
- B. Follicular tonsillitis
- C. Aphthous ulcer
- D. Membranous tonsillitis
Explanation: ***Diphtheria*** - The image shows a **thick, grayish-white pseudomembrane** covering the tonsils and likely extending to other parts of the pharynx, which is a classic sign of diphtheria. - **Hoarseness** indicates laryngeal involvement, a severe complication of diphtheria due to pseudomembrane formation extending to the larynx, potentially causing airway obstruction. *Follicular tonsillitis* - This condition presents with **pus-filled follicles** or spots on the tonsils, which are typically yellow or white, rather than a confluent membrane. - While it causes throat pain and fever, it generally does not lead to the formation of a **firm, adherent pseudomembrane** or significant hoarseness from laryngeal obstruction as seen in diphtheria. *Aphthous ulcer* - An aphthous ulcer is a **small, painful, shallow sore** with a white or yellowish center and a red border, typically found on the non-keratinized oral mucosa. - It does not present as a widespread, thick membranous lesion covering the tonsils and causing hoarseness. *Membranous tonsillitis* - While "membranous tonsillitis" describes the presence of a membrane on the tonsils, this term is often used generally. However, the specific characteristics in the image (thick, grayish, adherent membrane with severe symptoms like hoarseness) are pathognomonic for **diphtheria**. - Other causes of membranous tonsillitis, such as infectious mononucleosis, typically present with a less adherent membrane and often lack the severe systemic toxicity and potential for rapid airway compromise seen in diphtheria.
Question 1182: Which virus is typically associated with serpiginous ulcers in the distal esophagus?
- A. CMV (Correct Answer)
- B. Herpes
- C. Pill
- D. Corrosive
Explanation: CMV - Serpiginous ulcers in the distal esophagus are indicative of **cytomegalovirus (CMV) esophagitis**, especially in immunocompromised patients. - CMV infection can lead to **ulcerative lesions** that have a characteristic serpentine appearance, differentiating it from other causes. *Pill* - Pill-induced esophagitis generally results in **localized ulcers** rather than serpiginous ones and is often associated with the use of certain medications. - Symptoms typically include **dysphagia** and **odynophagia**, without the characteristic serpentine ulcer morphology. *Corrosive* - Corrosive injuries from chemicals present as **burn-like lesions** and strictures rather than serpiginous ulcers; the morphology is quite distinct. - These injuries usually occur due to ingestion of strong acids or alkalis, leading to **necrosis**, and don't show typical serpiginous ulceration. *Herpes* - Herpes simplex virus usually causes **multiple shallow ulcers** rather than deep, serpiginous ulcers, and is more commonly observed in the form of **vesicular lesions**. - Typically it presents with fever and significant **pain**, which is not the primary characteristic of CMV esophagitis.
Question 1183: Which of the following conditions is least associated with HIV infection?
- A. Kaposi sarcoma
- B. Oesophageal candidiasis
- C. Primary CNS lymphoma
- D. Tertiary syphilis (Correct Answer)
Explanation: ***Tertiary syphilis*** - While syphilis can be more aggressive in HIV-positive individuals, **tertiary syphilis** (e.g., gummas, neurosyphilis, cardiovascular syphilis) is not specifically or exclusively associated with HIV infection itself, but rather the untreated progression of syphilis within an immunocompromised host [1]. - The other conditions listed are **AIDS-defining illnesses** or strongly associated with the severe immunodeficiency caused by HIV [1]. *Oesophageal candidiasis* - This is an **AIDS-defining illness**, indicating severe immunosuppression in HIV-positive individuals [1]. - It results from an overgrowth of *Candida albicans* due to a compromised immune system [1]. *Kaposi sarcoma* - This is a cancer caused by **human herpesvirus 8 (HHV-8)**, and its incidence is significantly increased in HIV-infected individuals, leading to its classification as an **AIDS-defining illness** [1]. - It presents as vascular lesions on the skin, mucous membranes, lymph nodes, or internal organs [1]. *Primary CNS lymphoma* - This is another **AIDS-defining illness** that occurs with increased frequency in HIV-positive individuals, particularly those with advanced immunosuppression [1]. - It is often associated with the **Epstein-Barr virus (EBV)** in this population [1].
Question 1184: What are the essential major blood culture criteria for diagnosing infective endocarditis?
- A. Single positive culture of Coxiella burnetii (Correct Answer)
- B. Single positive culture of Corynebacterium species
- C. Both HACEK and Coxiella cultures
- D. Single positive culture of HACEK group
Explanation: ***Single positive culture of Coxiella burnetii*** - A single positive blood culture for **Coxiella burnetii** or **anti-phase I IgG antibody titer > 1:800** is considered a major criterion for infective endocarditis due to its highly pathogenic nature in this context [1], [2]. - This organism is a known cause of **culture-negative endocarditis**, and specific serology or molecular tests are often required for diagnosis [1]. *Single positive culture of Corynebacterium species* - **Corynebacterium species** are often considered **contaminants** in blood cultures, especially *Corynebacterium jeikeium*, and typically require multiple positive cultures, often from different sites, to be considered significant pathogens for infective endocarditis [2]. - A single positive culture of these organisms alone is generally insufficient to meet major diagnostic criteria for endocarditis [2]. *Both HACEK and Coxiella cultures* - While both **HACEK organisms** and **Coxiella burnetii** can cause endocarditis, the combination of both is not a specific major criterion in itself. - The diagnostic criteria address each organism individually [2]. *Single positive culture of HACEK group* - **HACEK organisms** (**H**aemophilus, **A**ggregatibacter, **C**ardiobacterium, **E**ikenella, **K**ingella) are well-known causes of endocarditis, but usually require **two separate positive blood cultures** for infective endocarditis major criteria [2]. - A single positive culture of a HACEK organism is typically classified as a minor criterion unless other supporting evidence is present.
Question 1185: Punched out ulcers in the esophagus are most commonly associated with which of the following conditions?
- A. Reflux esophagitis
- B. Herpes simplex virus (HSV)
- C. CMV (Correct Answer)
- D. Candida
Explanation: ***Oesophagitis*** - Characterized by **punched-out ulcers** in the esophagus, often related to infectious causes. - Common in patients with **immunocompromised** states, where mucosal inflammation leads to these distinctive lesions [1]. *cmv* - Typically associated with **shallow ulcers** and **larger lesions**, not specifically "punched-out" ulcers. - CMV esophagitis usually presents with **linear ulcerations** and is less common in the absence of immune deficiency [1]. *candida* - Characterized by **white plaques** or pseudomembranes rather than **punched-out ulcers**. - Common in individuals with **oral thrush** and presents as **esophageal symptoms** such as dysphagia [1]. *herpes* - Often leads to **sharp, serpiginous ulcers** that are distinct from the punched-out variety. - Typically associated with **oral lesions** and presents with acute severe pain while swallowing [1]. **References:** [1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Alimentary System Disease, pp. 347-348.
Question 1186: After 4 months of renal transplantation, which infection is most likely to develop?
- A. EBV
- B. Candida
- C. Histoplasma
- D. Cytomegalovirus (CMV) (Correct Answer)
Explanation: ***Cytomegalovirus (CMV)*** - **CMV infection** or reactivation is most common in transplant recipients between 1 and 6 months post-transplantation, often peaking around 3-4 months when immunosuppression is high [1]. - It can cause a wide range of clinical syndromes, including **fever**, **leukopenia**, **gastroenteritis**, and organ-specific disease in immunocompromised individuals [1]. *EBV* - **Epstein-Barr virus (EBV)** is primarily associated with **post-transplant lymphoproliferative disorder (PTLD)**, which tends to occur later, typically more than 6 months after transplantation, especially in pediatric recipients [1]. - While EBV can reactivate, severe clinical disease or PTLD is less likely to peak at 4 months compared to CMV [1]. *Candida* - **Candida infections** are typically **early complications** after transplantation, usually occurring within the first month [1]. - They are often related to indwelling catheters, antibiotics, and surgical anastomoses, making them less likely to be the most common infection at 4 months. *Histoplasma* - **Histoplasma capsulatum** causes **histoplasmosis**, a fungal infection prevalent in endemic areas (e.g., Ohio and Mississippi River valleys). - While possible in immunocompromised patients, it's generally an **opportunistic infection** that can occur at any time, but is less specific to the 4-month post-transplant window compared to CMV.
Question 1187: A patient complains about painful blisters around the angle of mouth, identify the pathogen
- A. Coxsackievirus
- B. Epstein-Barr Virus
- C. Varicella-Zoster Virus
- D. Herpes Simplex Virus type 1 (HSV-1) (Correct Answer)
Explanation: ***Herpes Simplex Virus type 1 (HSV-1)*** - HSV-1 is the primary cause of **oral herpes**, commonly presenting as **cold sores** or **fever blisters** around the mouth [1]. - The characteristic painful blisters at the angle of the mouth are typical of **recurrent HSV-1 infection** [1]. *Coxsackievirus* - Coxsackievirus primarily causes **hand-foot-and-mouth disease** or **herpangina**, characterized by lesions on the hands, feet, and inside the mouth/throat, not typically painful blisters around the external angle of the mouth [2]. - It often presents with a **rash** and **fever** in children [2]. *Epstein-Barr Virus* - Epstein-Barr Virus (EBV) is the causative agent of **infectious mononucleosis**, which presents with **fatigue**, **fever**, **sore throat**, and **lymphadenopathy**. - It does not typically cause painful blisters around the mouth. *Varicella-Zoster Virus* - Varicella-Zoster Virus (VZV) causes **chickenpox** (primary infection) and **shingles** (reactivation) [3]. - While shingles can cause painful blisters, it typically follows a **dermatomal distribution** and is not localized to the angle of the mouth in this manner [3].
Question 1188: Which condition is most commonly associated with cryoglobulinemia?
- A. Ovarian cancer
- B. Diabetes
- C. Leukemia
- D. Hepatitis C (Correct Answer)
Explanation: **Hepatitis C** - **Hepatitis C virus (HCV) infection** is the most common cause of mixed cryoglobulinemia, with cryoglobulins being detected in a high percentage of infected individuals. - The chronic immune stimulation caused by HCV leads to the production of **monoclonal or polyclonal immunoglobulins** (cryoglobulins) that precipitate in the cold. *Ovarian cancer* - While certain malignancies can be associated with paraneoplastic syndromes, **ovarian cancer** is not typically linked to cryoglobulinemia. - Cryoglobulinemia is more commonly associated with **lymphoproliferative disorders** or chronic infections rather than solid tumors like ovarian cancer. *Diabetes* - **Diabetes mellitus** is not directly associated with cryoglobulinemia; it is a metabolic disorder affecting glucose regulation. - Complications of diabetes include microvascular and macrovascular disease, but not primary cryoglobulin formation. *Leukemia* - Certain hematological malignancies, particularly **lymphoproliferative disorders like Waldenström macroglobulinemia or multiple myeloma**, can be associated with cryoglobulinemia. - However, **leukemia** (especially acute forms) is less commonly linked to cryoglobulinemia than chronic infections like hepatitis C or certain B-cell lymphomas.
Question 1189: Which is not included in AIDS related complex?
- A. Recurrent genital candidiasis
- B. Generalised lymphadenopathy
- C. Chronic diarrhea
- D. Ectopic pregnancy (Correct Answer)
Explanation: ***Ectopic pregnancy*** - **Ectopic pregnancy** is a gynecological condition related to reproductive health and is **not a direct manifestation** of HIV infection or one of the opportunistic infections/conditions characteristic of AIDS-related complex. - While HIV can affect overall health during pregnancy, an ectopic pregnancy itself is a different medical issue. *Recurrent genital candidiasis* - **Recurrent genital candidiasis** can be a sign of **diminished immune function** in HIV-positive women [1]. - It is often considered an AIDS-defining condition or a common opportunistic infection seen in the progression of HIV to AIDS-related complex [1]. *Generalised lymphadenopathy* - **Generalized lymphadenopathy**, specifically **persistent generalized lymphadenopathy (PGL)**, is a common early manifestation of HIV infection [1]. - It reflects ongoing immune activation and is part of the spectrum of conditions included in AIDS-related complex [1]. *Chronic diarrhea* - **Chronic diarrhea** (lasting more than one month) is a frequent and significant symptom in individuals with HIV infection, particularly as the disease progresses [1]. - It can be caused by various opportunistic infections or directly by HIV, and is a component of AIDS-related complex or AIDS-defining illness [1].
Question 1190: A boy presented with multiple non suppurative osteomyelitis with sickle cell anaemia. What will be the causative organism?
- A. Salmonella (Correct Answer)
- B. H. influenzae
- C. Enterobacter species
- D. Staphylococcus aureus
Explanation: ***Salmonella*** - **Salmonella species** are a well-known cause of **osteomyelitis** in patients with **sickle cell anemia**, due to factors like gut mucosal damage and functional asplenia. [1] - The unique pathophysiology of sickle cell disease, including areas of bone infarction and compromised reticulendothelial system function, predisposes these patients to **Salmonella infections**. [1] *Staphylococcus aureus* - While **Staphylococcus aureus** is the most common cause of osteomyelitis in the general population, it is less likely to be the causative organism in patients with **sickle cell anemia** compared to Salmonella. - Its presence usually indicates other predisposing factors like trauma or prosthetic devices. *H. influenzae* - **Haemophilus influenzae** was a common cause of osteomyelitis in children before widespread vaccination but is now rare, especially with routine immunizations. - It is not specifically associated with a higher risk in patients with **sickle cell disease** for osteomyelitis compared to other pathogens. *Enterobacter species* - **Enterobacter species** can cause osteomyelitis, particularly in immunocompromised individuals or following surgery, but they are not uniquely associated with **sickle cell anemia** as a primary cause compared to Salmonella. - Their involvement in non-suppurative osteomyelitis in this specific patient population is less common.
Practice by Chapter
Principles of Antimicrobial Therapy
Practice Questions
Fever of Unknown Origin
Practice Questions
HIV/AIDS and Related Infections
Practice Questions
Tuberculosis and Mycobacterial Diseases
Practice Questions
Tropical and Parasitic Infections
Practice Questions
Viral Infections (Hepatitis, Herpes, etc.)
Practice Questions
Healthcare-Associated Infections
Practice Questions
Fungal Infections
Practice Questions
Sepsis and Septic Shock
Practice Questions
Infection in Immunocompromised Hosts
Practice Questions
Emerging and Re-emerging Infections
Practice Questions
Antimicrobial Resistance
Practice Questions
Vaccination Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Start For Free