
Clinical Manifestations and Presentation of Diseases — MCQs

On this page
Which parameter is the most definitive in ruling out malnutrition?
Which of the following conditions is NOT typically associated with low glucose levels in pleural fluid?
A female patient of 26 years, presents with oral ulcers, photosensitivity and skin malar rash in face sparing the nasolabial folds of both side.
Identify the condition given in the image below?

Casal's necklace is associated with the deficiency of:
Which of the following exocrine glandular ducts are not obstructed in cystic fibrosis?
What is the most common cause of delirium?
A 50 year old male presents with fever and malaise for 4 months and pain in the knees and ankles. Blood tests are normal apart from a raised ESR. Chest x-ray shows bilateral hilar adenopathy and pulmonary infiltrates most severe in the upper and mid zones. Mantoux test is negative. What is the most likely diagnosis?
Bilateral parotid enlargement occurs in all, Except:
Crush Syndrome is associated with all of the following features except -
Clinical Manifestations and Presentation of Diseases Indian Medical PG Practice Questions and MCQs
Question 251: Which parameter is the most definitive in ruling out malnutrition?
- A. Edema
- B. Skinfold thickness
- C. Normal ECF volume
- D. Normal lean body mass (Correct Answer)
Explanation: ***Normal lean body mass*** - Maintaining **normal lean body mass** is the most definitive indicator that the body has sufficient protein stores and energy reserves, effectively ruling out significant malnutrition [3]. - Malnutrition, particularly **protein-energy malnutrition**, directly leads to the depletion of muscle and fat stores, which is reflected in reduced lean body mass [3]. *Edema* - **Edema** can be a sign of malnutrition (e.g., kwashiorkor due to severe protein deficiency), but its absence does not definitively rule out malnutrition as other forms exist without it [1], [3]. - Edema can also be caused by various other conditions such as **heart failure**, **kidney disease**, or **liver disease**, making it a non-specific indicator for ruling out malnutrition. *Skinfold thickness* - **Skinfold thickness** measures subcutaneous fat, which can be low in malnutrition, but it does not fully assess protein stores or visceral fat, making it less definitive. - While a low skinfold thickness suggests **fat depletion**, a normal reading could still coexist with protein malnutrition if fat stores have been relatively preserved [2]. *Normal ECF volume* - **Normal extracellular fluid (ECF) volume** is not a primary or definitive parameter for ruling out malnutrition. - Malnutrition can affect fluid balance, but ECF volume is influenced by many factors unrelated to nutritional status, such as **renal function** and **hydration status**.
Question 252: Which of the following conditions is NOT typically associated with low glucose levels in pleural fluid?
- A. Malignant pleural effusion
- B. Rheumatoid arthritis
- C. Empyema
- D. Dressler's syndrome (Correct Answer)
Explanation: ***Dressler's syndrome*** - Also known as post-myocardial infarction syndrome, is an **inflammatory reaction** that typically presents with a **transudative pleural effusion**. - Pleural fluid analysis in Dressler's syndrome usually shows n**ormal or slightly elevated glucose levels**, as inflammation is not severe enough to cause significant glucose consumption by metabolic activity in the pleural space. *Empyema* - Characterized by significant **bacterial activity** within the pleural space, leading to a high metabolic demand. - Bacteria and inflammatory cells consume glucose, resulting in **very low pleural fluid glucose levels**. *Malignant pleural effusion* - Malignant cells within the pleural space have a high metabolic rate and consume glucose. - This often leads to **low pleural fluid glucose levels**, especially in extensive or rapidly growing malignancies. *Rheumatoid arthritis* - Pleural effusions associated with **rheumatoid arthritis** often present with very low glucose levels. - This is due to the presence of numerous **inflammatory cells** and high metabolic activity within the inflamed pleura.
Question 253: A female patient of 26 years, presents with oral ulcers, photosensitivity and skin malar rash in face sparing the nasolabial folds of both side.
- A. Sturge weber syndrome
- B. Dermatitis
- C. Psoriasis
- D. SLE (Correct Answer)
Explanation: ***SLE*** - The combination of **oral ulcers**, **photosensitivity**, and a **malar rash** that spares the nasolabial folds is highly characteristic of **Systemic Lupus Erythematosus (SLE)** [1]. - SLE is an autoimmune disease with diverse clinical manifestations involving multiple organ systems. *Sturge weber syndrome* - This is a neurocutaneous disorder characterized by a **port-wine stain** (nevus flammeus) typically on the face, neurological abnormalities like seizures, and ocular involvement. - It does not present with oral ulcers or photosensitivity as primary features. *Dermatitis* - **Dermatitis** is a general term for skin inflammation, often presenting with redness, itching, and sometimes blisters. - It does not typically involve the specific constellation of oral ulcers, photosensitivity, and a malar rash that spares nasolabial folds. *Psoriasis* - **Psoriasis** is a chronic autoimmune disease primarily affecting the skin, characterized by red, scaly patches (plaques) [2]. - While it can cause nail changes and sometimes joint pain, it does not present with photosensitivity, oral ulcers, or the characteristic malar rash described.
Question 254: Identify the condition given in the image below?
- A. Chronic lymphedema (Correct Answer)
- B. Cushing syndrome
- C. Osteoporosis
- D. None of the options
Explanation: ***Chronic lymphedema*** - The image shows a **swollen foot** with **thickened, dry, and hyperkeratotic skin**, and **deep skin folds**, particularly between the toes. This is characteristic of **chronic lymphedema** due to impaired lymphatic drainage. - The presence of the **Stemmer's sign** (inability to pinch and lift the skin at the base of the second toe) is a common finding in lymphedema, which can be inferred from the overall appearance of the toes. *Cushing syndrome* - Cushing syndrome is characterized by **central obesity**, **moon facies**, **buffalo hump**, and **thin, fragile skin** with **striae**, not typically severe localized edema and skin changes as seen in the image. - While fluid retention can occur, it does not manifest as the characteristic cutaneous changes of chronic lymphedema. *Osteoporosis* - Osteoporosis is a condition of **decreased bone density**, making bones fragile and prone to fractures. - It does not present with visible skin changes or edema as depicted in the image. *None of the options* - The image clearly shows severe manifestations identifiable as **chronic lymphedema**, therefore one of the provided options is correct.
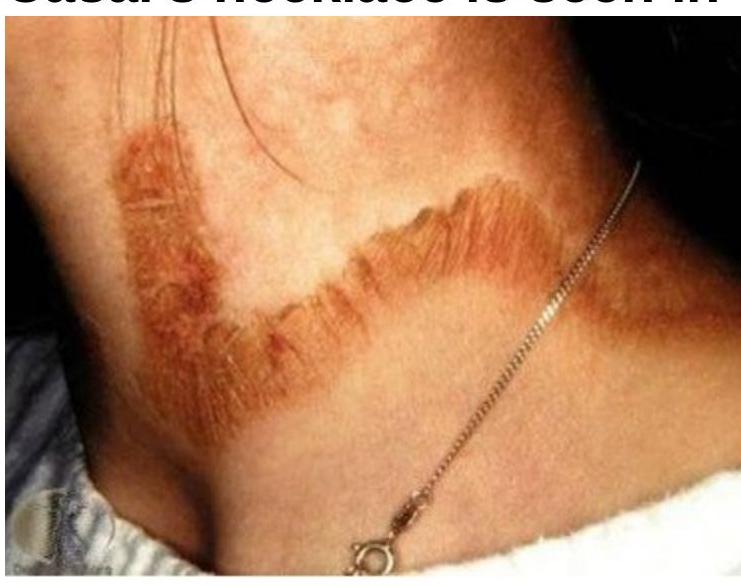
Question 255: Casal's necklace is associated with the deficiency of:
- A. Deficiency of Vitamin A
- B. Deficiency of Iron
- C. Deficiency of Vitamin B12
- D. Deficiency of Niacin (Vitamin B3) (Correct Answer)
Explanation: ***Deficiency of Niacin (Vitamin B3)*** - **Casal's necklace** is a characteristic dermatological manifestation of **pellagra**, which is caused by **niacin (Vitamin B3) deficiency**. - It presents as a **symmetrical, photosensitive dermatitis** on the neck and other sun-exposed areas, resembling a necklace. *Deficiency of Vitamin A* - Vitamin A deficiency primarily affects **vision**, leading to **night blindness** and **xerophthalmia**. - It can also cause follicular **hyperkeratosis** (dry, rough skin), but not the distinct 'necklace' pattern seen in pellagra. *Deficiency of Iron* - Iron deficiency typically causes **anemia**, leading to symptoms like **fatigue**, **pallor**, and **koilonychia** (spoon-shaped nails). - It does not directly cause skin lesions like Casal's necklace. *Deficiency of Vitamin B12* - Vitamin B12 deficiency is associated with **megaloblastic anemia** and **neurological symptoms** (e.g., peripheral neuropathy, cognitive impairment). - While it can cause **hyperpigmentation** in some cases, it does not specifically manifest as Casal's necklace.
Question 256: Which of the following exocrine glandular ducts are not obstructed in cystic fibrosis?
- A. Pancreas
- B. Lung
- C. Sweat gland (Correct Answer)
- D. None of the options
Explanation: ***Sweat gland*** - In cystic fibrosis, the **CFTR protein** in sweat glands is defective, leading to **impaired chloride reabsorption** and excessively salty sweat [1]. - This defect causes dysfunctional sweat production but **does not result in obstruction** of the sweat gland ducts, which continue to secrete. *Pancreas* - The **exocrine pancreatic ducts** are frequently obstructed in cystic fibrosis due to the production of **thick, sticky mucus**. - This obstruction leads to maldigestion and **pancreatic insufficiency**, requiring enzyme replacement therapy. *Lung* - **Bronchial ducts** and airways in the lungs are severely affected by the accumulation of **viscous mucus**, leading to chronic obstruction [1]. - This obstruction impairs mucociliary clearance, making patients susceptible to recurrent **pulmonary infections** and progressive lung damage [1], [2]. *None of the options* - This option is incorrect because sweat glands are indeed not obstructed, making option C the appropriate answer.
Question 257: What is the most common cause of delirium?
- A. Infection (Correct Answer)
- B. Liver failure
- C. Belladonna poisoning
- D. None of the options
Explanation: ***Infection*** - **Infections**, particularly urinary tract infections (UTIs) or pneumonia, are a very common and often reversible cause of **delirium**, especially in elderly or immunocompromised patients [1]. - The systemic inflammatory response to infection can lead to neuroinflammation and direct effects on brain function, manifesting as acute changes in attention and cognition. *Liver failure* - While **liver failure** can cause **hepatic encephalopathy**, which presents with altered mental status, it typically has a more gradual onset and a different neurochemical profile than acute delirium caused by infection. - Hepatic encephalopathy is characterized by abnormal ammonia metabolism and often includes motor signs like **asterixis**, which are not universally present in delirium from infection. *Belladonna poisoning* - **Belladonna poisoning** (due to **anticholinergic toxicity**) can cause **delirium**, along with a constellation of symptoms like dilated pupils, dry mouth, and tachycardia. - However, it is a specific toxicological cause and not as broad or commonly encountered as infection as a general cause of new-onset delirium in hospitalized or elderly populations. *None of the options* - This option is incorrect because **infection** is indeed a very common and recognized cause of delirium [1].
Question 258: A 50 year old male presents with fever and malaise for 4 months and pain in the knees and ankles. Blood tests are normal apart from a raised ESR. Chest x-ray shows bilateral hilar adenopathy and pulmonary infiltrates most severe in the upper and mid zones. Mantoux test is negative. What is the most likely diagnosis?
- A. Tuberculosis
- B. Sarcoidosis (Correct Answer)
- C. Asbestosis
- D. Berylliosis
Explanation: ***Sarcoidosis*** - The constellation of **bilateral hilar adenopathy**, pulmonary infiltrates (especially in upper/mid zones), **arthralgia** (knees and ankles), and a **negative Mantoux test** in a patient with unexplained fever and malaise is highly suggestive of sarcoidosis [1]. - A **raised ESR** is a non-specific inflammatory marker often seen in sarcoidosis. *Tuberculosis* - While tuberculosis can cause fever, malaise, pulmonary infiltrates, and elevated ESR, a **negative Mantoux test** makes primary or active tuberculosis less likely in an immunocompetent individual. - **Bilateral hilar adenopathy** is also less typical of primary pulmonary tuberculosis compared to sarcoidosis. *Asbestosis* - This is an **occupational lung disease** caused by asbestos exposure, primarily presenting with **progressive dyspnea** and **restrictive lung disease**. - It characteristically involves the **lower lobes**, causes **pleural plaques**, and is not typically associated with acute arthralgia, fever, or prominent hilar adenopathy. *Berylliosis* - This is another **occupational lung disease** resulting from beryllium exposure, often mimicking sarcoidosis both clinically and pathologically [2]. - However, without a history of **beryllium exposure** and given the classic presentation, sarcoidosis is a more prevalent default diagnosis [2].
Question 259: Bilateral parotid enlargement occurs in all, Except:
- A. HIV
- B. SLE
- C. Chronic pancreatitis (Correct Answer)
- D. Mumps
Explanation: ***SLE*** - **Systemic Lupus Erythematosus (SLE)** typically does not present with **bilateral parotid enlargement**, which is more characteristic of other conditions. - Salivary gland involvement in SLE is less prevalent and usually not the primary clinical feature associated with the disease. *HIV* - **HIV** infection can lead to **bilateral parotid enlargement** due to associated conditions such as lymphadenopathy and infections like **salivary gland infections**. [1] - **Lymphoid tissue** hyperplasia in response to HIV is another factor contributing to this enlargement. *Sjogren's syndrome* - **Sjogren's syndrome** is a common cause of **bilateral parotid enlargement** due to inflammatory infiltrates affecting the salivary glands. - Patients typically experience **xerostomia** (dry mouth) and **xerophthalmia** (dry eyes) alongside gland enlargement [2]. *Chronic pancreatitis* - Patients with **chronic pancreatitis** may develop **bilateral parotid enlargement** due to associated changes such as **sialadenosis** from malnutrition and electrolyte imbalances. - The enlargement occurs as a **compensatory mechanism** related to the pancreatic pathology affecting nearby structures.
Question 260: Crush Syndrome is associated with all of the following features except -
- A. Hypercalcemia (Correct Answer)
- B. Hypocalcemia
- C. Hyperkalemia
- D. Increased serum creatinine
Explanation: ***Hypercalcemia*** - Crush syndrome involves massive **muscle damage** leading to the release of intracellular contents, but hypercalcemia is not typically seen acutely. - While skeletal muscle contains calcium, its release, if any, is usually outweighed by other electrolyte shifts and renal dysfunction, often leading to **hypocalcemia** due to calcium binding to damaged tissues and phosphate. *Hypocalcemia* - This is a common feature of **crush syndrome** because calcium ions move into damaged cells and bind to free fatty acids and damaged tissue. - The elevated **phosphate levels** released from damaged cells can also bind to circulating calcium, further reducing serum calcium. *Hyperkalemia* - One of the most dangerous complications of **crush syndrome**, resulting from the massive release of **intracellular potassium** from damaged muscle cells. - Can lead to **life-threatening arrhythmias** if not promptly managed. *Increased serum creatinine* - Damaged muscle releases large amounts of **creatinine**, which is a byproduct of muscle metabolism; this, along with **myoglobin** (leading to acute kidney injury), causes a significant increase in serum creatinine levels. - **Acute kidney injury** due to rhabdomyolysis is a hallmark of crush syndrome, leading to impaired clearance of waste products.
Practice by Chapter
Approach to Common Symptoms (Fever, Pain, Fatigue)
Practice Questions
Constitutional Symptoms and Their Differential Diagnosis
Practice Questions
Syncope and Presyncope
Practice Questions
Dizziness and Vertigo
Practice Questions
Dyspnea and Respiratory Distress
Practice Questions
Chest Pain Evaluation
Practice Questions
Abdominal Pain Assessment
Practice Questions
Headache Classification and Management
Practice Questions
Weight Loss and Cachexia
Practice Questions
Edema and Fluid Retention
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Start For Free