
Cardiology — MCQs

On this page
A healthy middle-aged man who became emotionally upset during an argument with his brother suddenly developed chest pain and collapsed. He was declared dead upon arrival at the hospital. What is the most likely diagnosis?
In which condition are epsilon waves observed on an ECG?
Which of the following is the most appropriate true statement regarding ostium primum atrial septal defect (ASD)?
Which is not a major criterion of Jones in rheumatic fever?
A 4-year-old girl is brought to the pediatrician's office, where her father reports that she suddenly became pale and stopped running while playfully chasing her and her pet Chihuahua. After 30 minutes, she was no longer pale and wanted to resume the game. She has never had a previous episode and has never been cyanotic. Her physical examination was normal, as were her chest x-ray and echocardiogram. An ECG shows a specific pattern indicating which of the following?
A lady presents with grade 3 dyspnea, severe mitral stenosis, and atrial fibrillation, with an increased ventricular rate and a clot in the left atrium. Which of the following should not be done?
Where are venous emboli most often lodged?
Straight back syndrome is associated with?
What is the best drug for managing atrial flutter with a 4:1 block?
What does Harvey's sign indicate?
Cardiology Indian Medical PG Practice Questions and MCQs
Question 1591: A healthy middle-aged man who became emotionally upset during an argument with his brother suddenly developed chest pain and collapsed. He was declared dead upon arrival at the hospital. What is the most likely diagnosis?
- A. Takotsubo cardiomyopathy (Correct Answer)
- B. Dilated cardiomyopathy
- C. Chronic ischemic cardiomyopathy
- D. Arrhythmogenic right ventricle dysplasia
Explanation: ***Takotsubo cardiomyopathy*** - Presents with sudden **chest pain** and collapse following **severe emotional stress**, mimicking a myocardial infarction but often without significant coronary artery disease. - It involves dramatic and transient left ventricular systolic dysfunction, often described as **apical ballooning**, that can lead to acute heart failure and sudden death. *Dilated cardiomyopathy* - Typically presents with **progressive heart failure symptoms** such as dyspnea and fatigue, not sudden collapse after acute emotional stress. - It is characterized by **ventricular dilation** and impaired systolic function, developing over time from various causes. *Arrhythmogenic right ventricle dysplasia* - This condition primarily affects the **right ventricle**, leading to fibrofatty replacement of myocardial tissue and increasing the risk of **ventricular arrhythmias** and sudden cardiac death, especially during exertion. - The presentation of sudden collapse after emotional stress, without prior athletic activity, makes it less likely than Takotsubo cardiomyopathy. *Chronic ischemic cardiomyopathy* - This condition results from **long-standing coronary artery disease**, leading to **myocardial remodeling**, reduced systolic function, and chronic heart failure. - While it can cause sudden cardiac death due to arrhythmias, the acute onset after emotional upset in an otherwise healthy individual is less typical for a chronic process [1].
Question 1592: In which condition are epsilon waves observed on an ECG?
- A. Hypothermia
- B. RV dysplasia (Correct Answer)
- C. Takotsubo cardiomyopathy
- D. None of the options
Explanation: RV dysplasia - **Epsilon waves** are small, positive deflections (after the QRS complex) seen on an ECG, pathognomonic for **Arrhythmogenic Right Ventricular Dysplasia (ARVD)**. - ARVD is a genetic disorder where the muscle tissue of the right ventricle is replaced by **fibrofatty tissue**, leading to arrhythmias. *Hypothermia* - Hypothermia is associated with **Osborn waves** (J waves), which are positive deflections at the QRS-ST junction, not epsilon waves. - Other ECG changes in hypothermia include **bradycardia**, prolongation of PR, QRS, and QT intervals. *Takotsubo cardiomyopathy* - This condition typically presents with **ST-segment elevation** and T-wave inversions, mimicking an acute myocardial infarction, but lacks coronary artery disease. - It is characterized by **transient apical ballooning** of the left ventricle, usually triggered by severe emotional or physical stress. *None of the options* - This option is incorrect because **RV dysplasia** specifically features epsilon waves, making it a correct choice. - Epsilon waves are a distinct and recognizable ECG finding associated with this particular cardiac condition.
Question 1593: Which of the following is the most appropriate true statement regarding ostium primum atrial septal defect (ASD)?
- A. Results in right axis deviation (RAD) on the ECG
- B. Is associated with Holt-Oram syndrome
- C. Is less common than secundum ASD
- D. Is unlikely to close spontaneously (Correct Answer)
Explanation: Current guidelines indicate that **ostium primum ASDs** are structural defects involving the **atrial septum** adjacent to the **AV valves** and are not amenable to spontaneous closure [1]. Their location near the **crux of the heart** and association with **cleft mitral valves** makes them more complex and less likely to resolve naturally compared to secundum ASDs. **Ostium primum ASDs** typically cause a **left axis deviation (LAD)** on the ECG due to an associated defect in the **atrioventricular (AV) conduction system**, leading to uncoordinated ventricular depolarization. **Right axis deviation (RAD)** is more commonly seen in **large secundum ASDs** with significant left-to-right shunting and resultant **pulmonary hypertension**. **Holt-Oram syndrome** is primarily associated with **secundum ASDs**, not ostium primum ASDs. Genetic or chromosomal abnormalities, such as Down's syndrome, are also known to cause septal defects [2]. **Ostium primum ASDs** account for about **15-20%** of all ASDs. **Secundum ASDs** are the most common type, typically involving the fossa ovalis, making up approximately **70-75%** of all atrial septal defects [1].
Question 1594: Which is not a major criterion of Jones in rheumatic fever?
- A. Pancarditis
- B. Chorea
- C. Elevated ESR (Correct Answer)
- D. Arthritis
Explanation: Elevated ESR - While an **elevated ESR** (erythrocyte sedimentation rate) is a common finding in acute rheumatic fever, it is considered a **minor criterion** in the modified Jones criteria due to its non-specificity. - Minor criteria include fever, arthralgia, elevated acute phase reactants (ESR, CRP), and prolonged PR interval on ECG. *Pancarditis* - **Pancarditis** (inflammation of all layers of the heart) is a **major criterion** and the most serious manifestation of rheumatic fever, as it can lead to permanent heart damage [1]. - It includes pericarditis, myocarditis, and endocarditis, often resulting in **valvulitis** [1]. *Arthritis* - **Arthritis**, typically a **migratory polyarthritis** affecting large joints, is a **major criterion** of Jones. - The pain is often disproportionately severe compared to the findings, hence the term "pain that flies from joint to joint." *Chorea* - **Sydenham's chorea** (St. Vitus' dance), characterized by rapid, purposeless involuntary movements, is a **major criterion** [1]. - It often appears later in the course of the disease and can be the sole manifestation of rheumatic fever [1].
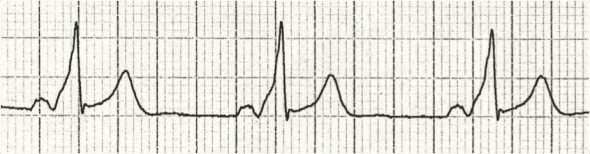
Question 1595: A 4-year-old girl is brought to the pediatrician's office, where her father reports that she suddenly became pale and stopped running while playfully chasing her and her pet Chihuahua. After 30 minutes, she was no longer pale and wanted to resume the game. She has never had a previous episode and has never been cyanotic. Her physical examination was normal, as were her chest x-ray and echocardiogram. An ECG shows a specific pattern indicating which of the following?
- A. Paroxysmal ventricular tachycardia
- B. Wolff-Parkinson-White syndrome (Correct Answer)
- C. Stokes-Adams syndrome
- D. Paroxysmal supraventricular tachycardia
Explanation: ***Wolff-Parkinson-White syndrome*** - The ECG shows a **short PR interval** and a **delta wave** (slurring of the initial upstroke of the QRS complex), which are classic signs of **pre-excitation** seen in Wolff-Parkinson-White (WPW) syndrome. - The child's symptoms of sudden pallor and stopping activity, followed by spontaneous recovery, suggest a brief episode of **tachycardia** due to WPW, which can cause symptoms stemming from reduced cardiac output. *Paroxysmal ventricular tachycardia* - **Ventricular tachycardia** is characterized by wide, bizarre QRS complexes originating from the ventricles, often without a preceding P wave, which is not clearly depicted in the provided ECG. - While it can cause sudden symptoms like pallor due to reduced cardiac output, the distinctive **delta wave** and **short PR interval** seen in the ECG point away from primary VT and towards pre-excitation. *Stokes-Adams syndrome* - This syndrome involves recurrent episodes of **syncope** due to a transient **heart block** or **bradyarrhythmia**, leading to a sudden decrease in cerebral perfusion. - The ECG in Stokes-Adams syndrome would typically show evidence of severe bradycardia or asystole during an event, which is not consistent with the depicted ECG or the likely tachyarrhythmic nature of the symptoms. *Paroxysmal supraventricular tachycardia* - While **paroxysmal supraventricular tachycardia (PSVT)** is common in children and can cause symptoms like pallor, the ECG would typically show a **narrow QRS complex tachycardia** with absent or abnormal P waves, but **lacks the delta wave and short PR interval** characteristic of WPW. - WPW syndrome is a common cause of PSVT in children, but the ECG findings specifically indicate the underlying Wolff-Parkinson-White pattern, rather than just the generic PSVT.
Question 1596: A lady presents with grade 3 dyspnea, severe mitral stenosis, and atrial fibrillation, with an increased ventricular rate and a clot in the left atrium. Which of the following should not be done?
- A. Rate control with diltiazem
- B. Warfarin therapy
- C. Open mitral commissurotomy and removal of clot
- D. Electrical cardioversion (Correct Answer)
Explanation: ***Electrical cardioversion*** - Due to the presence of a **left atrial clot**, electrical cardioversion is contraindicated as it carries a high risk of **systemic embolism** if the clot dislodges. - Cardioversion should only be considered after **anticoagulation** and confirmation that no left atrial clot is present, typically via transesophageal echocardiography (TEE). *Rate control with diltiazem* - **Diltiazem** is a calcium channel blocker commonly used for **rate control in atrial fibrillation** by slowing AV nodal conduction [1]. - While rate control is important in this patient, especially with severe mitral stenosis, it does not directly address the immediate high risk of **embolism** from the clot [2]. *Warfarin therapy* - **Warfarin** is indicated for **anticoagulation** to prevent further clot formation and reduce the risk of embolism in patients with atrial fibrillation and a documented left atrial clot [2]. - However, warfarin itself will not acutely resolve an existing clot or address the immediate hemodynamic issues, and it requires a therapeutic INR before interventions like cardioversion can be considered. *Open mitral commissurotomy and removal of clot* - **Open mitral commissurotomy** is a surgical procedure to address severe mitral stenosis and can simultaneously allow for direct removal of a **left atrial clot**. - While this is a definitive treatment for both the stenosis and the clot, it is an invasive surgical option and not something to "not be done" if indicated, although risks need to be weighed.
Question 1597: Where are venous emboli most often lodged?
- A. Lungs (Correct Answer)
- B. Kidneys
- C. Intestinal veins
- D. Coronary arteries
Explanation: ***Lungs*** - **Venous emboli** are primarily lodged in the **pulmonary arteries**, causing **pulmonary embolism** [1]. - This occurs due to **deep vein thrombosis (DVT)** where clots travel to the lungs via the venous system [1]. *Heart* - While the heart can be affected by emboli, it usually deals with **arterial embolism** stemming from **atrial fibrillation** or other cardiac conditions. - Venous emboli typically bypass the heart before reaching the lungs; they do not lodge here. *Intestines* - Emboli can affect the intestines but they usually arise from **arterial sources**, leading to **ischemic bowel**. - The intestines are generally not a common site for venous emboli to lodge. *Kidneys* - Kidney emboli often result from **arterial occlusion**, particularly in conditions like **renal artery stenosis**. - Venous emboli do not typically impact the kidneys, as they move toward the pulmonary circulation.
Question 1598: Straight back syndrome is associated with?
- A. Osteopetrosis
- B. Mitral valve prolapse (Correct Answer)
- C. Cor-triatriatum
- D. Ankylosing spondylitis
Explanation: ***Mitral valve prolapse*** - **Straight back syndrome** refers to a reduction in the normal thoracic kyphosis, which can decrease the **anteroposterior diameter** of the chest. - This flattened chest can compress the heart, particularly the **mitral valve**, leading to auscultatory findings suggestive of prolapse, even in the absence of true valvular dysfunction. *Ankylosing spondylitis* - This is a chronic inflammatory disease primarily affecting the **axial skeleton**, leading to spinal fusion and stiffness, which is distinct from a flattened thoracic spine. - While it affects the spine, it causes an abnormal **kyphosis or lordosis** rather than a simply straightened back that predisposes to cardiac compression. *Osteopetrosis* - This is a rare genetic disorder characterized by abnormally dense bones due to a defect in **osteoclast function**. - Its musculoskeletal manifestations involve increased bone fragility and hematological issues, not a specific spinal curvature anomaly like straight back syndrome. *Cor-triatriatum* - This is a rare congenital heart defect where the **left atrium (cor triatriatum sinistrum)** or, less commonly, the **right atrium (cor triatriatum dextrum)** is divided by a fibromuscular membrane. - It is a primary cardiac structural anomaly and has no association with musculoskeletal conditions such as straight back syndrome.
Question 1599: What is the best drug for managing atrial flutter with a 4:1 block?
- A. Esmolol
- B. Amiodarone (Correct Answer)
- C. Vernakalant
- D. Lignocaine
Explanation: ***Amiodarone*** - **Amiodarone** is an effective antiarrhythmic drug for managing **atrial flutter** by controlling ventricular rate and potentially restoring sinus rhythm. - Its broad spectrum of action, including effects on potassium, sodium, and calcium channels, makes it suitable for various supraventricular and ventricular arrhythmias. *Esmolol* - **Esmolol** is a **beta-blocker** primarily used for rapid heart rate control in acute settings due to its short half-life. - While it can control ventricular rate in **atrial flutter**, it does not typically convert the rhythm to sinus [1]. *Vernakalant* - **Vernakalant** is an **antiarrhythmic drug** specifically approved for the rapid conversion of recent-onset atrial fibrillation to sinus rhythm. - It is not indicated for **atrial flutter** or for managing chronic arrhythmias. *Lignocaine* - **Lignocaine** (Lidocaine) is a **Class Ib antiarrhythmic drug** primarily used for **ventricular arrhythmias**. - It is generally ineffective for **supraventricular arrhythmias** like atrial flutter.
Question 1600: What does Harvey's sign indicate?
- A. Transmitted pressure wave on coughing in an artery
- B. Indicates venous filling after emptying a vein (Correct Answer)
- C. Loss of hair from eyebrows
- D. None of the options
Explanation: ***Indicates venous filling after emptying a vein*** - **Harvey's sign**, also known as the **Trendelenburg test (modified)** or **Brodie-Trendelenburg test**, assesses the competence of venous valves in the legs [1]. - It involves emptying the superficial veins by elevating the leg and then observing for rapid venous filling after the patient stands, indicating **venous reflux** due to incompetent valves [1]. *Transmitted pressure wave on coughing in an artery* - This description typically relates to signs of a **patent ductus arteriosus** (a thrill or murmur) or **aneurysms**, where a cough can transmit a palpable impulse. - It is not associated with Harvey's sign or the assessment of venous valve competency [1]. *Loss of hair from eyebrows* - **Madarosis**, specifically loss of hair from the outer third of the eyebrows, is a classic sign of **hypothyroidism** (also known as Hertoghe's sign). - This symptom is entirely unrelated to Harvey's sign, which is a clinical maneuver for evaluating venous function. *None of the options* - This option is incorrect because the second option accurately describes Harvey's sign (or a related clinical maneuver for assessing venous competence).
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Start For Free