All (1216)Anatomy (104)Anesthesiology (21)Biochemistry (179)Community Medicine (104)Dental (9)Dermatology (21)ENT (2)Forensic Medicine (41)General Medicine (2)Internal Medicine (79)Microbiology (83)Obstetrics and Gynecology (63)Ophthalmology (68)Orthopaedics (36)Pathology (82)Pediatrics (43)Pharmacology (85)Physiology (91)Psychiatry (2)Psychiatry (20)Radiology (28)Surgery (53)
Q831
Commonest ligament injured in ankle injury ?
Q832
Which of the following is NOT a symptom of carpal tunnel syndrome?
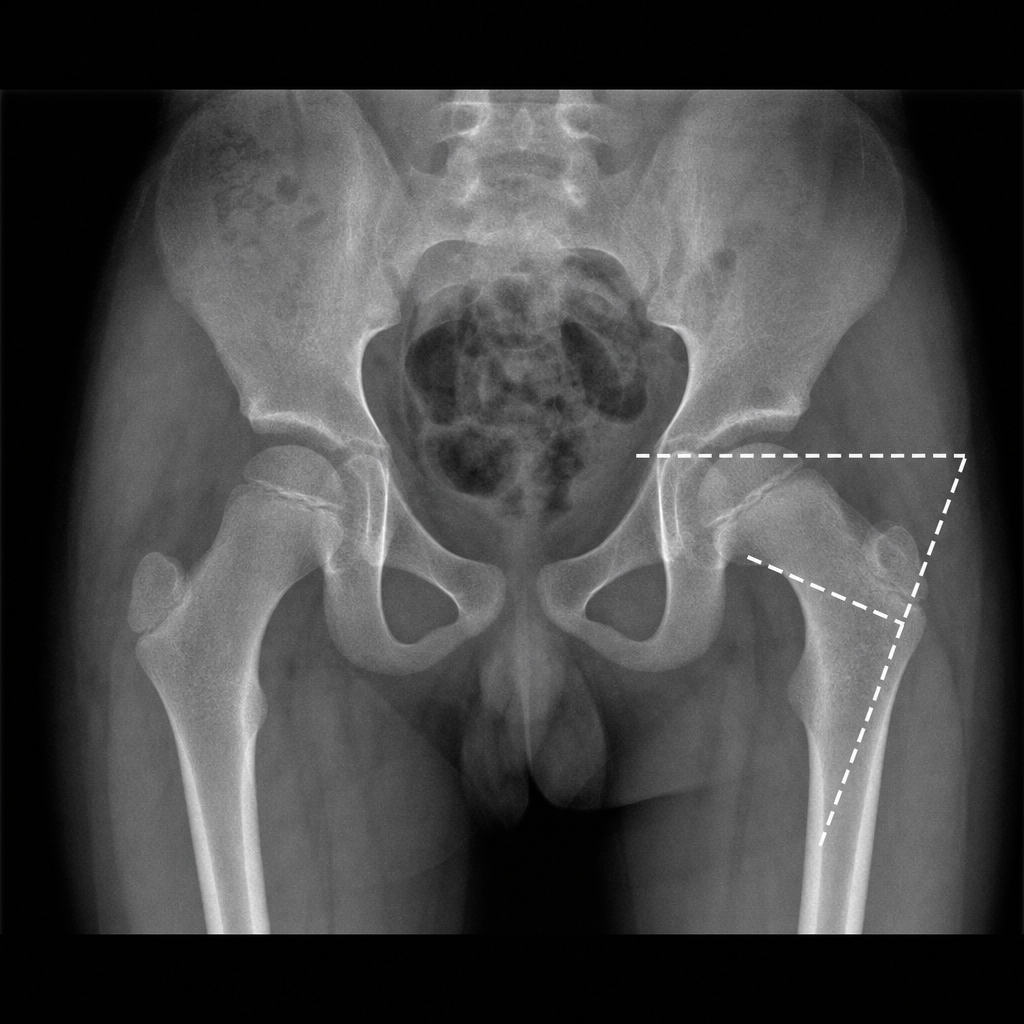
Q833
Fairbank triangle is seen in
Q834
What is the primary reason for early stabilization of a femur shaft fracture?