INI-CET 2015 — Pathology
4 Previous Year Questions with Answers & Explanations
In a patient, Mitral valve vegetations are seen along the lines of closure along with fusion of commissures. What is the likely diagnosis?

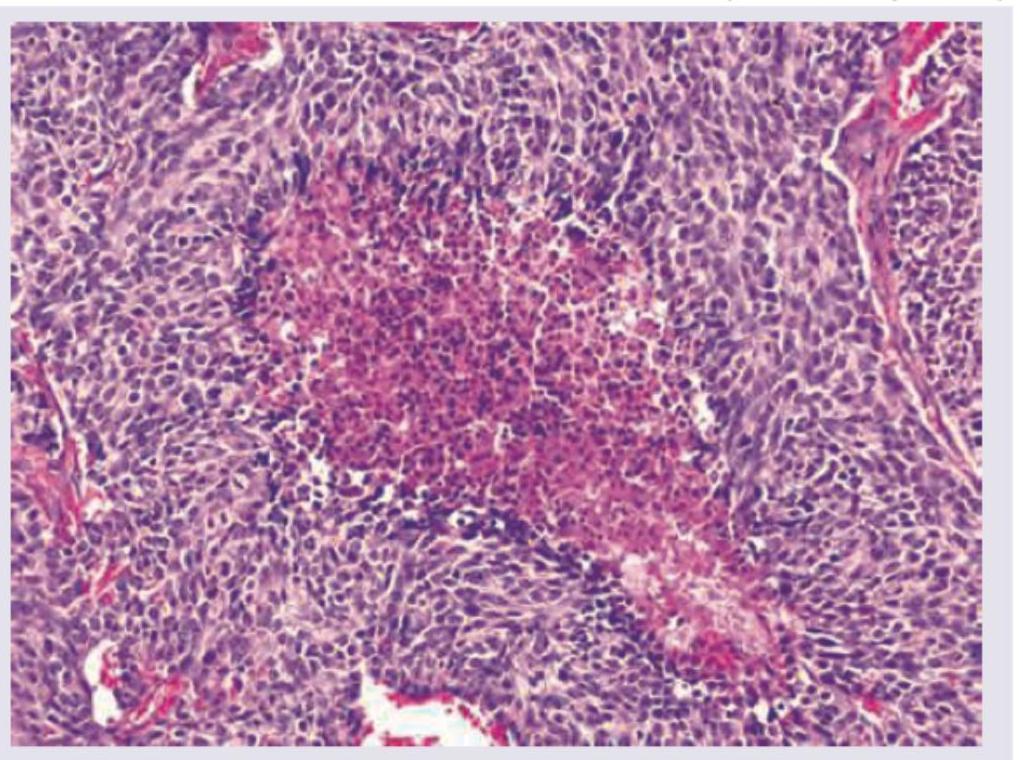
A 55-year-old male patient presented with a 4 month history of cough and hemoptysis. Bronchoscopy revealed an intrabronchial polyp. Biopsy from the polyp showed small cells with salt and pepper chromatin, with microscopic necrosis and 5 mitotic figures per 10 high power fields as shown below. Chromogranin staining was positive. What is the diagnosis and grade of the lesion?
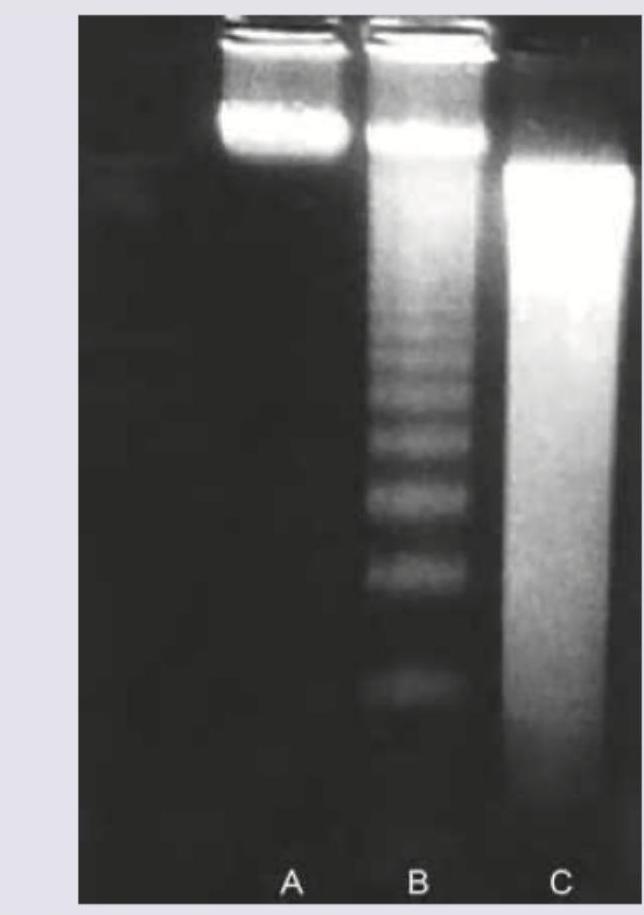
Agarose gel electrophoresis from DNA of a population of cells as seen under ultraviolet light is shown below. What is the correct explanation for the finding seen in the band labeled as "C"?
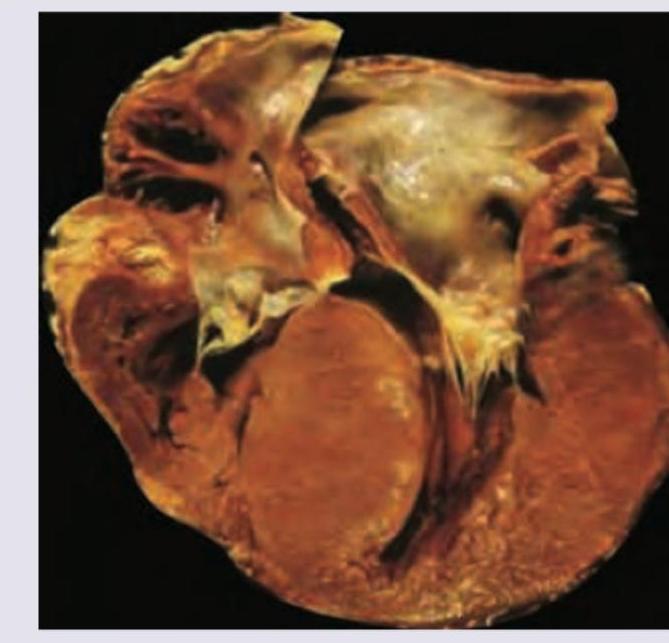
An athlete collapsed suddenly during exercise and died on the field. Postmortem heart is shown in the figure. There is family history of heart disease. What is the diagnosis?
INI-CET 2015 - Pathology INI-CET Practice Questions and MCQs
Question 1: In a patient, Mitral valve vegetations are seen along the lines of closure along with fusion of commissures. What is the likely diagnosis?
- A. Libman-Sacks endocarditis
- B. Marantic endocarditis
- C. Bacterial endocarditis
- D. Rheumatic endocarditis (Correct Answer)
Explanation: ***Rheumatic endocarditis*** - **Rheumatic fever** is a common cause of **mitral valve disease**, leading to **vegetations along the lines of closure** [2] and characteristic **fusion of commissures** [1]. - This chronic inflammation results in **fibrosis** and **calcification**, causing **mitral stenosis** [3] or regurgitation. *Libman-Sacks endocarditis* - Characterized by **sterile vegetations** typically found on **both sides of the valve leaflets** (atrial and ventricular surfaces) [2], often associated with **Systemic Lupus Erythematosus (SLE)**. - It does not typically cause **commissural fusion** or significant valvular stenosis. *Marantic endocarditis* - Also known as **nonbacterial thrombotic endocarditis (NBTE)**, it involves **sterile vegetations** composed of fibrin and platelets, usually found on the **lines of closure** [2]. - It is associated with **debilitating illnesses** like cancer or sepsis, but **does not cause commissural fusion**. *Bacterial endocarditis* - Involves **large, destructive vegetations** that can be found on any part of the valve [2], often associated with **valve destruction**, **abscess formation**, and **septic emboli**. - While it causes vegetations, it typically **does not lead to commissural fusion** as a primary feature; fusion is more characteristic of chronic rheumatic heart disease. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Heart, pp. 566-567. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Heart, p. 568. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Cardiovascular Disease, pp. 293-294.
Question 2: A 55-year-old male patient presented with a 4 month history of cough and hemoptysis. Bronchoscopy revealed an intrabronchial polyp. Biopsy from the polyp showed small cells with salt and pepper chromatin, with microscopic necrosis and 5 mitotic figures per 10 high power fields as shown below. Chromogranin staining was positive. What is the diagnosis and grade of the lesion?
- A. Carcinoid grade 1
- B. Small cell carcinoma grade IV
- C. Large cell neuroendocrine carcinoma grade IV
- D. Atypical carcinoid grade 2 (Correct Answer)
Explanation: ***Atypical carcinoid grade 2*** - The presence of **salt and pepper chromatin**, **microscopic necrosis**, and **5 mitotic figures per 10 high power fields** are characteristic features of an **atypical carcinoid tumor** [1]. - **Positive chromogranin staining** confirms neuroendocrine differentiation, and the mitotic rate coupled with necrosis indicates a Grade 2 (atypical) carcinoid based on WHO classification [1]. *Carcinoid grade 1* - A typical carcinoid (Grade 1) would show **no necrosis** and a mitotic count of **less than 2 mitoses per 10 high power fields**, which contradicts the findings [1]. - While it features **salt and pepper chromatin** and positive neuroendocrine markers, the higher mitotic activity and necrosis exclude a typical carcinoid. *Small cell carcinoma grade IV* - **Small cell carcinoma** typically presents with extensive necrosis, very high mitotic activity (often >10 mitoses/10 HPF), and a more **scanty cytoplasm** than seen here, and often **crush artifact** [2]. - Although it is a high-grade neuroendocrine tumor, the described features (only 5 mitoses/10HPF, "salt and pepper chromatin" is less typical for SCLC which has more uniform nuclei, and distinct necrosis without widespread crush artifact) are more consistent with an atypical carcinoid [1], [2]. *Large cell neuroendocrine carcinoma grade IV* - **Large cell neuroendocrine carcinoma** (LCNEC) is characterized by **large cells** with prominent nucleoli, high mitotic counts (often >10-11 mitoses/10HPF), and extensive necrosis [2]. - The "small cells" and **salt and pepper chromatin** described in the biopsy are inconsistent with the large cell morphology of LCNEC. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lung, pp. 725-727. [2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Respiratory Tract Disease, pp. 337-338.
Question 3: Agarose gel electrophoresis from DNA of a population of cells as seen under ultraviolet light is shown below. What is the correct explanation for the finding seen in the band labeled as "C"?
- A. Predominantly necrotic cells
- B. Mixed population of normal and apoptotic cells
- C. A population of viable cells
- D. Apoptotic cells (Correct Answer)
Explanation: ***Apoptotic cells*** - Band C shows a characteristic **DNA ladder pattern** with discrete bands representing fragmentation into nucleosome-sized units (multiples of ~180-200 base pairs), which is pathognomonic of **apoptosis**. [1] - During apoptosis, **endonucleases** cleave DNA at internucleosomal linker regions, creating uniform fragments that migrate as distinct bands on agarose gel electrophoresis. *Predominantly necrotic cells* - **Necrotic cell DNA** undergoes random, non-specific degradation by cellular enzymes, resulting in a continuous **smear pattern** rather than discrete bands. - The **smear appearance** reflects DNA fragments of varying sizes distributed throughout the gel, unlike the organized pattern seen in band C. *Mixed population of normal and apoptotic cells* - A mixed population would show both **intact high molecular weight DNA** (remaining near the gel origin) and the **apoptotic ladder pattern** superimposed. - Band C displays a pure ladder pattern without evidence of intact DNA, indicating a homogeneous apoptotic population. *A population of viable cells* - **Viable cells** maintain intact genomic DNA that remains as a single **high molecular weight band** near the top of the gel. - The **fragmented ladder pattern** in band C is incompatible with viable cell DNA, which should show minimal degradation. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Cellular Responses to Stress and Toxic Insults: Adaptation, Injury, and Death, pp. 63-64.
Question 4: An athlete collapsed suddenly during exercise and died on the field. Postmortem heart is shown in the figure. There is family history of heart disease. What is the diagnosis?
- A. Hypertrophic cardiomyopathy (Correct Answer)
- B. Mitral regurgitation
- C. Mitral stenosis
- D. Aortic stenosis with left ventricular hypertrophy
Explanation: ***Hypertrophic cardiomyopathy*** - **Sudden cardiac death** in young athletes, especially with a family history, is a classic presentation of **hypertrophic cardiomyopathy (HCM)** [2][3]. - Postmortem examination typically reveals **asymmetric septal hypertrophy** and **myocardial fiber disarray**, which are characteristic of HCM [1]. *Mitral regurgitation* - While mitral regurgitation can lead to heart failure, it is less commonly associated with **sudden death in athletes** without prior symptoms. - The primary finding would be **valvular abnormalities** and **left atrial/ventricular dilation**, not typically isolated hypertrophy. *Mitral stenosis* - Mitral stenosis primarily causes **left atrial enlargement** and **pulmonary hypertension**, leading to symptoms like dyspnea and fatigue. - It is not a common cause of **sudden cardiac death** in athletes and would not typically present with the gross hypertrophy seen in HCM. *Aortic stenosis with left ventricular hypertrophy* - Aortic stenosis can cause **left ventricular hypertrophy** due to increased pressure overload. - However, sudden death in athletes due to aortic stenosis is less common than HCM, and the hypertrophy in aortic stenosis is typically **concentric** and symmetrical, unlike the asymmetric hypertrophy often seen in HCM [1]. **References:** [1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Heart, pp. 577-578. [2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Heart, pp. 576-577. [3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Cardiovascular Disease, pp. 303-304.