
Gynaecology

On this page
Recognising Bleeding Disorders: Foundations of Abnormal and Ectopic Bleeding
A 32-year-old woman presents with heavy periods requiring pad changes every hour, describing clots "the size of golf balls." Meanwhile, in the emergency department, a 28-year-old with 6 weeks amenorrhoea reports unilateral pelvic pain and light vaginal bleeding. These scenarios represent two critical gynaecological presentations-abnormal uterine bleeding and ectopic pregnancy -that demand systematic evaluation and timely intervention. Understanding their classifications, epidemiology, and diagnostic frameworks forms the cornerstone of competent gynaecological practice.
Abnormal Uterine Bleeding (AUB) Classification:
- PALM-COEIN system (FIGO 2011) stratifies causes into structural and non-structural:
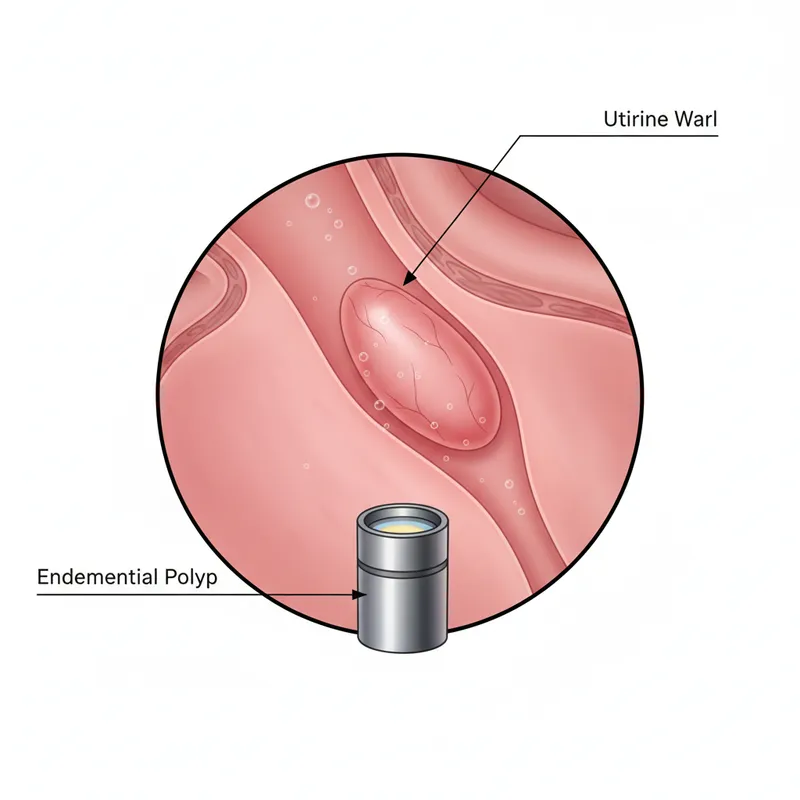
- Structural (PALM): Polyp, Adenomyosis, Leiomyoma, Malignancy
- Non-structural (COEIN): Coagulopathy, Ovulatory dysfunction, Endometrial, Iatrogenic, Not classified
- Heavy menstrual bleeding (HMB): Excessive blood loss (>80ml/cycle) interfering with quality of life
- Affects 25% of women of reproductive age
- Accounts for 20% of gynaecology referrals in UK primary care
- Intermenstrual bleeding (IMB): Bleeding between regular cycles
- Postcoital bleeding (PCB): Bleeding after sexual intercourse-requires cervical assessment
Ectopic Pregnancy Essentials:
- Definition: Pregnancy implanted outside the uterine cavity
- 95% tubal (ampulla most common site)
- Rare sites: ovarian (3%), cervical, caesarean scar, abdominal
- Epidemiology:
- Incidence 11 per 1,000 pregnancies in UK
- Leading cause of maternal death in first trimester (6% of maternal deaths)
- Recurrence risk 10-15% after one ectopic
| Parameter | AUB | Ectopic Pregnancy |
|---|---|---|
| UK Prevalence | 25% reproductive-age women | 1.1% of all pregnancies |
| Peak Age | 40-50 years (HMB) | 30-34 years |
| Emergency Risk | Anaemia, rarely life-threatening | Life-threatening rupture |
| Mortality | <0.1% | 0.2-0.5% (if ruptured) |
📌 Mnemonic for Ectopic Risk Factors: PIPES
PID, IUD, Previous ectopic, Endometriosis, Surgery (tubal)
Recognising Bleeding Disorders: Foundations of Abnormal and Ectopic Bleeding


2 - Pathophysiological Mechanisms: Why Bleeding Occurs
The mechanisms underlying abnormal bleeding diverge fundamentally between structural uterine pathology and ectopic implantation. In abnormal uterine bleeding , disrupted endometrial haemostasis results from either anatomical distortion (fibroids creating increased surface area, adenomyosis disrupting myometrial contractility) or molecular dysregulation (increased prostaglandin E2/prostacyclin ratio, impaired vasoconstriction). Anovulatory cycles-common in PCOS and perimenopause-produce unopposed oestrogen stimulation, causing irregular endometrial proliferation without progesterone-mediated stabilisation, leading to unpredictable breakthrough bleeding.
AUB Mechanistic Pathways:
- Structural causes:
- Fibroids: Distort endometrial vasculature, increase surface area (submucosal worst)
- Adenomyosis: Ectopic endometrial glands in myometrium → impaired uterine contractility
- Polyps: Localised endometrial overgrowth with fragile vasculature
- Coagulopathy (13% of HMB):
- Von Willebrand disease most common (1% population prevalence)
- Platelet dysfunction, factor deficiencies
- Endometrial dysfunction:
- Altered prostaglandin ratios (↑ PGE2:PGF2α)
- Increased fibrinolysis (elevated tissue plasminogen activator)
- Impaired vasoconstriction
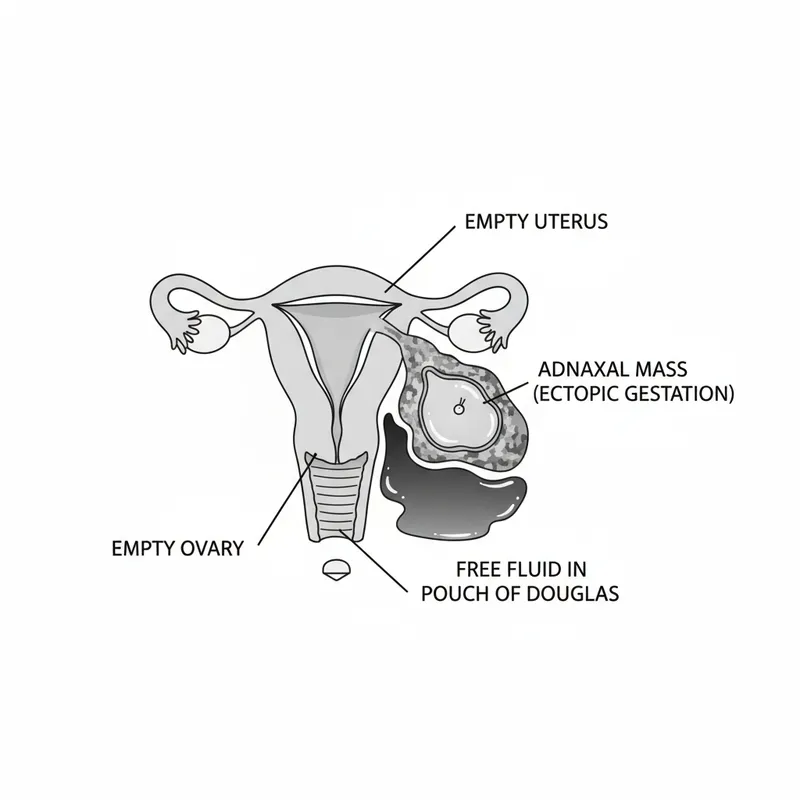
Ectopic Pregnancy Pathophysiology:
In ectopic pregnancy , impaired tubal transport allows blastocyst implantation in the fallopian tube. Risk factors-previous PID causing tubal scarring, endometriosis creating inflammatory milieu, tubal surgery disrupting ciliary function-all compromise the tube's ability to propel the embryo uterine-ward. The trophoblast invades the tubal wall, eroding blood vessels and causing bleeding into the peritoneal cavity. Unlike the muscular uterus, the thin-walled tube cannot accommodate growing gestational tissue, leading to rupture typically at 6-8 weeks gestation when β-hCG reaches 3,000-5,000 IU/L.
| Mechanism | Clinical Consequence | Investigation Marker |
|---|---|---|
| Unopposed oestrogen | Irregular heavy bleeding | Anovulatory progesterone <3 nmol/L |
| Fibroid distortion | Predictable HMB | MRI shows submucosal location |
| Tubal trophoblast invasion | Unilateral pain + bleeding | β-hCG plateau or slow rise |
| Tubal rupture | Haemodynamic collapse | Free fluid on USS, falling Hb |
2 — Pathophysiological Mechanisms: Why Bleeding Occurs
3 - Clinical Assessment: History, Examination, and Investigations
A 45-year-old presents with "flooding" periods lasting 9 days, passing clots, and requiring time off work. You quantify impact using a structured history, examine for structural causes, and order targeted investigations per NICE NG88 guidance. Meanwhile, a 26-year-old with positive pregnancy test and cramping requires urgent assessment for potential ectopic pregnancy , where clinical gestalt combined with serial β-hCG and transvaginal ultrasound determines management pathway.
History-Taking Priorities:
- AUB assessment:
- Quantify bleeding: Pictorial Blood Assessment Chart (PBAC >100 = HMB)
- Pattern: Regular/irregular, cycle length, intermenstrual/postcoital bleeding
- Impact: Anaemia symptoms (fatigue, palpitations), quality of life, fertility plans
- Risk factors: Obesity (anovulation), anticoagulation, PCOS, thyroid disease
- Ectopic pregnancy red flags:
- Triad: Amenorrhoea (6-8 weeks) + pelvic pain (unilateral) + vaginal bleeding
- Rupture indicators: Sudden severe pain, shoulder tip pain (diaphragmatic irritation), dizziness/syncope
Examination Findings:
- AUB: Abdominal masses (fibroids), bimanual examination (enlarged/tender uterus), speculum (exclude cervical pathology)
- Ectopic: Abdominal tenderness, cervical motion tenderness, adnexal mass (50%), peritonism if ruptured
Investigation Algorithm (NICE NG88 & NG126):
- AUB first-line:
- Full blood count: Hb <120 g/L indicates significant blood loss
- Ferritin: <15 μg/L confirms iron deficiency
- Coagulation screen if HMB since menarche or family history
- Pelvic USS: First-line imaging for structural causes
- Ectopic pregnancy pathway:
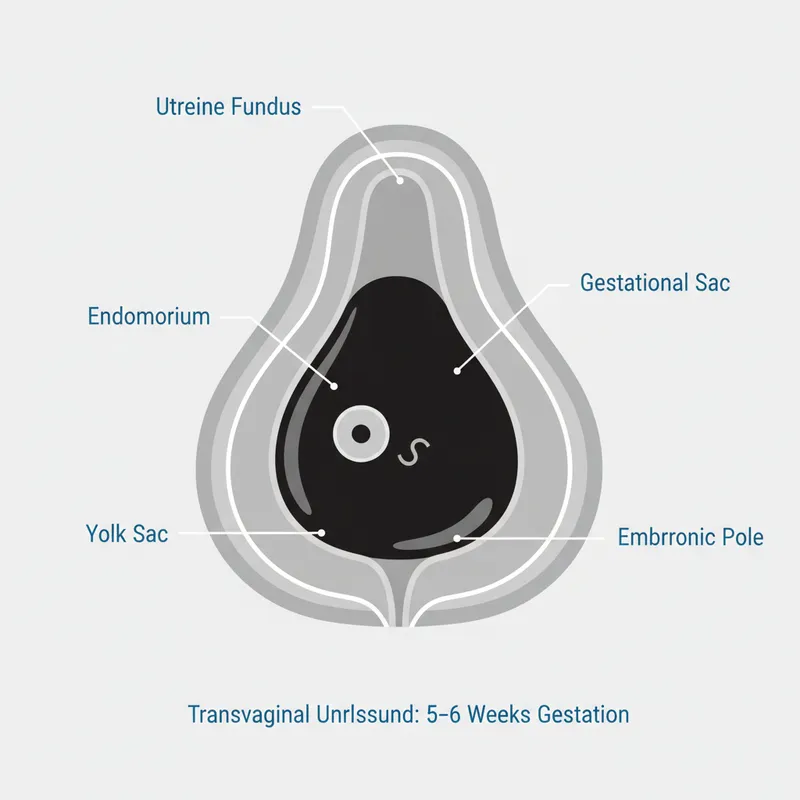
- Serum β-hCG: Discriminatory zone 1,500 IU/L (transvaginal USS should visualise intrauterine pregnancy)
- Transvaginal USS: Intrauterine gestational sac (confirms IUP), adnexal mass, free fluid
- Serial β-hCG (48h): Normal IUP rises >63%, ectopic typically <50% increase
| Investigation | Threshold | Sensitivity | Specificity |
|---|---|---|---|
| β-hCG rise >63% (48h) | Normal IUP | 99% | 93% |
| β-hCG plateau/fall | Failing pregnancy | 88% | 95% |
| USS gestational sac | β-hCG >1,500 IU/L | 90% | 100% |
| Endometrial thickness | >16mm (AUB) | 67% for pathology | 89% |
3 — Clinical Assessment: History, Examination, and Investigations
4 - Differential Diagnosis: Distinguishing Bleeding Causes
Separating benign from life-threatening bleeding requires systematic analysis. A 34-year-old with irregular bleeding and negative pregnancy test differs fundamentally from one with positive test and pain-the latter demands urgent ectopic exclusion . Similarly, distinguishing ovulatory HMB (regular cycles, structural causes) from anovulatory bleeding (irregular, endocrine dysfunction) guides targeted management for abnormal uterine bleeding .
Key Discriminators:
- Pregnancy status: β-hCG positive = ectopic/miscarriage/molar until proven otherwise
- Cycle regularity:
- Regular cycles (21-35 days) → structural causes (fibroids, polyps, adenomyosis)
- Irregular cycles → anovulation (PCOS, thyroid, hyperprolactinaemia)
- Age stratification:
- <20 years: Coagulopathy (13% of adolescent HMB)
- 30-40 years: Fibroids, adenomyosis
-
45 years: Endometrial cancer (2% of PMB)-requires urgent investigation
Common Diagnostic Pitfalls:
- Assuming negative urine pregnancy test excludes ectopic: False negatives occur with low β-hCG
- Missing coagulopathy: Ask about bruising, dental bleeding, family history
- Overlooking cervical pathology: Always visualise cervix with speculum
- Attributing all irregular bleeding to PCOS: Exclude endometrial hyperplasia/cancer
| Feature | Ectopic Pregnancy | Miscarriage | Ovulatory HMB | Anovulatory Bleeding |
|---|---|---|---|---|
| Cycle Pattern | Amenorrhoea then bleeding | Amenorrhoea then bleeding | Regular heavy cycles | Irregular unpredictable |
| Pain | Unilateral, severe | Midline cramping | Dysmenorrhoea | Minimal |
| β-hCG Pattern | Slow rise (<50% in 48h) | Falling | N/A | N/A |
| USS Findings | Adnexal mass, no IUP | Products in uterus | Structural pathology | Thickened endometrium |
| Urgency | EMERGENCY | Urgent | Routine | Routine |
4 — Differential Diagnosis: Distinguishing Bleeding Causes
5 - Evidence-Based Management: Medical, Surgical, and Conservative Options
NICE NG88 advocates a stepwise approach to abnormal uterine bleeding , prioritising medical management unless structural pathology mandates surgery. First-line treatment-levonorgestrel intrauterine system (LNG-IUS)-reduces menstrual blood loss by 94% at 12 months, superior to all oral therapies. For ectopic pregnancy , NICE NG126 stratifies management by haemodynamic stability, β-hCG level, and patient preference, balancing tubal preservation against treatment success.
AUB Medical Management:
- First-line: LNG-IUS (Mirena®)
- Dose: 52mg levonorgestrel, releases 20μg/day
- Efficacy: 94% reduction in menstrual blood loss
- Contraindications: Current breast cancer, distorted uterine cavity
- Tranexamic acid: 1g TDS days 1-4 of menses (39% reduction)
- Mefenamic acid: 500mg TDS days 1-4 (20-25% reduction)
- Combined oral contraceptive: Regulates cycle, reduces flow (43% reduction)
AUB Surgical Options:
- Endometrial ablation: For completed childbearing, normal cavity
- Success: 80% satisfaction at 5 years
- 24% require further surgery
- Hysterectomy: Definitive treatment
- Laparoscopic preferred (shorter recovery, fewer complications)
- Mortality risk 0.38 per 1,000
Ectopic Pregnancy Management:
- Expectant management (selected cases):
- Criteria: β-hCG <1,000 IU/L, falling, minimal symptoms, reliable patient
- Success: 69% resolve without intervention
- Medical: Methotrexate
- Criteria: β-hCG <1,500 IU/L, unruptured, no fetal heartbeat, mass <35mm
- Dose: 50mg/m² IM single dose (or multi-dose protocol)
- Success: 88% (single dose), 93% (multi-dose)
- Monitoring: β-hCG days 4 and 7 (expect 15% drop); repeat if <15% fall
- Contraindications: Breastfeeding, immunodeficiency, renal/hepatic impairment
- Surgical: Laparoscopy
- Salpingectomy: Removes affected tube (preferred if damaged tube, recurrent ectopic)
- Salpingotomy: Preserves tube (if contralateral tube damaged, desire fertility)
- Emergency laparotomy: If haemodynamically unstable
| Treatment | Indication | Success Rate | Key Monitoring |
|---|---|---|---|
| LNG-IUS | First-line HMB | 94% reduction MBL | Review 3-6 months |
| Methotrexate | Ectopic β-hCG <1,500 | 88% single dose | β-hCG days 4, 7 |
| Salpingotomy | Ectopic + fertility desire | 93% success | 7% persistent trophoblast |
| Hysterectomy | Failed medical Rx | 100% cure | Surgical complications |
5 — Evidence-Based Management: Medical, Surgical, and Conservative Options
6 - Complex Scenarios: Special Populations and Advanced Cases
Real-world patients present nuanced challenges. A 38-year-old with HMB and concurrent anticoagulation for prosthetic heart valve requires coordinated cardiology input before considering surgical management . Similarly, a woman with recurrent ectopic pregnancy and single remaining tube faces difficult decisions balancing fertility preservation against treatment success . These scenarios demand synthesis of clinical evidence, patient values, and multidisciplinary expertise.
Challenging AUB Cases:
- Anticoagulation + HMB:
- Tranexamic acid safe with warfarin/DOACs (no thrombotic risk increase)
- LNG-IUS preferred (local effect, minimal systemic absorption)
- Avoid NSAIDs if on antiplatelet therapy
- Adolescent HMB:
- 13% have underlying coagulopathy-screen with PT, APTT, vWF antigen/activity
- Combined OCP first-line (regulates cycle, reduces flow)
- Avoid LNG-IUS (insertion difficult, poor tolerance)
- Perimenopausal bleeding:
- Exclude malignancy: Endometrial biopsy if >45 years with persistent IMB
- LNG-IUS prevents endometrial hyperplasia during HRT
- Failed medical management:
- Consider GnRH analogues (3-6 months pre-surgery to reduce fibroid size)
- Uterine artery embolisation: 85% satisfaction, preserves fertility potential
Complex Ectopic Scenarios:
- Pregnancy of unknown location (PUL):
- β-hCG <1,500, no USS findings
- Serial β-hCG protocol: 48h intervals until location confirmed or resolved
- 10-15% ultimately ectopic
- Caesarean scar ectopic:
- Rare (1:2,000) but increasing with rising CS rates
- High rupture risk-requires specialist management (methotrexate + local injection or surgery)
- Cornual/interstitial ectopic:
- Implantation in uterine horn
- Later rupture (12-16 weeks), catastrophic haemorrhage
- Requires laparotomy (not laparoscopy)-mortality 2-2.5%
| Scenario | Key Consideration | Management Modification |
|---|---|---|
| Anticoagulation + HMB | Bleeding risk vs thrombosis | Tranexamic acid safe, avoid NSAIDs |
| Single tube + ectopic | Fertility preservation | Salpingotomy if feasible, counsel re: IVF |
| β-hCG >5,000 + ectopic | High rupture risk | Surgery preferred over methotrexate |
| Perimenopausal IMB | Malignancy risk | Mandatory endometrial sampling |
6 — Complex Scenarios: Special Populations and Advanced Cases
High Yield Summary
Key Take-Aways:
- HMB affects 25% of women; LNG-IUS is first-line medical management (94% reduction in menstrual blood loss)
- Ectopic pregnancy occurs in 1.1% of pregnancies; discriminatory β-hCG threshold is 1,500 IU/L for transvaginal USS
- PALM-COEIN classification systematically categorises AUB causes into structural and non-structural
- Methotrexate criteria for ectopic: β-hCG <1,500, unruptured, mass <35mm, no fetal heartbeat-88% success rate
- Serial β-hCG in normal IUP rises >63% in 48 hours; slower rise suggests ectopic or failing pregnancy
- Endometrial sampling mandatory for women >45 years with persistent intermenstrual bleeding (exclude cancer)
- Ruptured ectopic presents with triad: sudden severe pain, shoulder tip pain (diaphragmatic irritation), haemodynamic instability
Essential Gynaecology Numbers:
| Parameter | Threshold | Clinical Significance |
|---|---|---|
| β-hCG discriminatory zone | 1,500 IU/L | USS should show IUP if present |
| Normal IUP β-hCG rise | >63% in 48h | <50% suggests ectopic/failing |
| Methotrexate β-hCG limit | <1,500 IU/L | Higher levels = surgery preferred |
| LNG-IUS MBL reduction | 94% at 12 months | Superior to all oral therapies |
| Endometrial thickness (AUB) | >16mm abnormal | Warrants further investigation |
| Ectopic recurrence risk | 10-15% | After one previous ectopic |
Key Principles:
- Always exclude pregnancy in reproductive-age women with bleeding-urine test insufficient if symptoms suggest ectopic
- Structured history trumps investigations: PBAC score, impact on quality of life, and fertility plans guide AUB management
- Haemodynamic stability determines urgency: Unstable ectopic requires immediate laparotomy regardless of investigations
- Medical management first for AUB unless contraindications (distorted cavity, malignancy) or patient preference for surgery
- Serial monitoring essential in pregnancy of unknown location: 10-15% ultimately ectopic, requiring vigilant β-hCG tracking
Quick Reference:
| Condition | First Investigation | First-Line Management | Red Flag |
|---|---|---|---|
| HMB (regular cycles) | FBC, ferritin, pelvic USS | LNG-IUS 52mg | Postmenopausal bleeding |
| HMB (irregular cycles) | Add TSH, prolactin | Combined OCP or LNG-IUS | Age >45 + IMB (cancer risk) |
| Suspected ectopic | β-hCG + transvaginal USS | Depends on stability/β-hCG | Shoulder tip pain, syncope |
| Pregnancy unknown location | Serial β-hCG (48h) | Expectant if falling | β-hCG plateau or slow rise |
Continue reading on OnCourse
Sign up for free to access the full lesson, plus unlimited questions, flashcards, AI-powered notes, and more.
CONTINUE READING — FREEor get the app
Have doubts about this lesson?
Ask Rezzy, our AI tutor, to explain anything you didn't understand
Practice Questions: Gynaecology
Test your understanding with these related questions
A 43-year-old woman presents with fatigue, weight gain, and cold intolerance. TSH is 22 mU/L, free T4 is low. Anti-TPO antibodies are positive. She is trying to conceive. What is the TSH target?