Sedative, Hypnotic, and Anxiolytic Use Disorders Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Sedative, Hypnotic, and Anxiolytic Use Disorders. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Sedative, Hypnotic, and Anxiolytic Use Disorders Indian Medical PG Question 1: Mechanism of action of d-tubocurarine is:
- A. Competitive, nondepolarizing block at the Nm cholinergic receptor (Correct Answer)
- B. Noncompetitive, depolarizing block at the Nm cholinergic receptor
- C. Non-competitive, nondepolarizing block at the Nm cholinergic receptor
- D. Competitive, depolarizing block at the Nm cholinergic receptor
Sedative, Hypnotic, and Anxiolytic Use Disorders Explanation: ***Competitive, nondepolarizing block at the Nm cholinergic receptor***
- **d-tubocurarine** acts as a **competitive antagonist** at the **nicotinic muscle (Nm) cholinergic receptors** on the motor endplate.
- It competes with **acetylcholine (ACh)** for binding sites, preventing ACh from activating the receptor and causing **muscle paralysis** without depolarization.
*Noncompetitive, depolarizing block at the Nm cholinergic receptor*
- This describes the mechanism of action of **depolarizing neuromuscular blockers** like **succinylcholine**, which first *depolarize* the motor endplate before causing paralysis.
- d-tubocurarine does not cause initial depolarization; it directly blocks the receptor.
*Non-competitive, nondepolarizing block at the Nm cholinergic receptor*
- While d-tubocurarine is **nondepolarizing**, it is a **competitive antagonist**, not a non-competitive one.
- A non-competitive block would involve binding to a different site on the receptor or an associated ion channel, altering receptor function indirectly.
*Competitive, depolarizing block at the Nm cholinergic receptor*
- This option incorrectly combines the concepts, as **depolarizing blockers** like succinylcholine act initially by **depolarizing** the endplate, whereas d-tubocurarine is purely a **nondepolarizing** agent.
- The "competitive" aspect would be true for the binding of ACh to its site on a depolarizing agent, but the effect of d-tubocurarine is simply to block, not depolarize.
Sedative, Hypnotic, and Anxiolytic Use Disorders Indian Medical PG Question 2: A 30-year-old male presents with a history of consuming an unknown substance. On examination, the patient has diaphoresis, headache, and features resembling acute coronary spasm. Which of the following clinical features is least likely to be present in this patient?
- A. Hypertension
- B. Tachycardia
- C. Hyperthermia
- D. Bradycardia (Correct Answer)
- E. Mydriasis
Sedative, Hypnotic, and Anxiolytic Use Disorders Explanation: ***Bradycardia***
- The presented symptoms of diaphoresis, headache, and coronary spasm are consistent with **stimulant intoxication** (e.g., cocaine, amphetamines).
- Stimulants typically cause **tachycardia** due to sympathetic overactivity, making bradycardia the least likely finding.
*Hypertension*
- **Stimulant intoxication** leads to increased sympathetic activity, causing **vasoconstriction** and elevated blood pressure.
- This is a common and expected finding in cases presenting with coronary spasm due to substance abuse.
*Tachycardia*
- **Sympathetic overstimulation** from an unknown substance, particularly stimulants, directly increases heart rate.
- This symptom closely aligns with the patient's presentation of diaphoresis and coronary spasm.
*Hyperthermia*
- Elevated body temperature is a frequent consequence of **stimulant overdose** due to increased metabolic activity and impaired thermoregulation.
- **Diaphoresis** (sweating) can be a compensatory mechanism for hyperthermia or a direct effect of sympathetic activation.
*Mydriasis*
- **Pupillary dilation** is a characteristic finding in sympathomimetic toxidrome caused by stimulant drugs.
- This occurs due to alpha-adrenergic stimulation of the radial muscle of the iris and is commonly seen with cocaine or amphetamine use.
Sedative, Hypnotic, and Anxiolytic Use Disorders Indian Medical PG Question 3: Which of the following is the platinum-based chemotherapeutic agent used as first-line treatment for ovarian carcinoma?
- A. Cyclophosphamide
- B. Methotrexate
- C. Cisplatin (Correct Answer)
- D. Dacarbazine
Sedative, Hypnotic, and Anxiolytic Use Disorders Explanation: ***Cisplatin***
- **Cisplatin** is a platinum-based chemotherapy drug that forms **DNA cross-links**, inhibiting DNA synthesis and leading to the death of rapidly dividing cells, making it highly effective against **ovarian carcinoma**.
- It is a cornerstone of chemotherapy regimens for ovarian cancer, often used in combination with other agents such as paclitaxel.
*Methotrexate*
- **Methotrexate** is an **antimetabolite** that inhibits dihydrofolate reductase, thereby interfering with DNA synthesis.
- While it is used in various cancers like leukemia, lymphoma, and some solid tumors (e.g., breast cancer, gestational trophoblastic disease), it is **not a primary recommended drug for ovarian carcinoma**.
*Cyclophosphamide*
- **Cyclophosphamide** is an **alkylating agent** that causes DNA damage, leading to cell death.
- It is used in many cancers, including lymphoma, breast cancer, and some leukemias, but it is **not a first-line or primary agent for ovarian carcinoma** in contemporary treatment guidelines.
*Dacarbazine*
- **Dacarbazine** is an **alkylating agent** primarily used in the treatment of **malignant melanoma** and Hodgkin lymphoma.
- It is **not indicated for the treatment of ovarian carcinoma**.
Sedative, Hypnotic, and Anxiolytic Use Disorders Indian Medical PG Question 4: After 72 hours of Cessation of alcohol, which of the following withdrawal symptoms can be seen in alcoholic patients?
- A. Seizures
- B. Hallucinations
- C. Tremors
- D. Delirium tremens (Correct Answer)
Sedative, Hypnotic, and Anxiolytic Use Disorders Explanation: **Delirium tremens**
- **Delirium tremens** typically manifests **48-96 hours** (2-4 days) after the last drink, making it a key symptom seen around the 72-hour mark.
- It involves **severe confusion**, disorientation, **hallucinations** (visual, auditory, tactile), agitation, and autonomic instability like **tachycardia**, hyperthermia, and hypertension, representing the most severe form of alcohol withdrawal.
*Seizures*
- **Alcohol withdrawal seizures** usually occur much earlier, within **6 to 48 hours** after cessation.
- While possible within the broader withdrawal timeline, they are more characteristic of the initial stages rather than the 72-hour peak of delirium tremens.
*Hallucinations*
- **Alcoholic hallucinosis** typically develops **12-24 hours** after cessation and can persist for days.
- While hallucinations are a component of delirium tremens, isolated hallucinosis usually presents earlier without the global cognitive impairment and autonomic instability of DTs.
*Tremors*
- **Tremors** are among the first signs of alcohol withdrawal, appearing as early as **6-12 hours** after the last drink.
- These early symptoms are usually self-limiting or managed with benzodiazepines and precede the more severe stages seen at 72 hours.
Sedative, Hypnotic, and Anxiolytic Use Disorders Indian Medical PG Question 5: Match the following drugs in Column A with their contraindications in Column B.
| Column A | Column B |
| :-- | :-- |
| 1. Morphine | 1. QT prolongation |
| 2. Amiodarone | 2. Thromboembolism |
| 3. Vigabatrin | 3. Pregnancy |
| 4. Estrogen preparations | 4. Head injury |
- A. A-1, B-3, C-2, D-4
- B. A-4, B-1, C-3, D-2 (Correct Answer)
- C. A-3, B-2, C-4, D-1
- D. A-2, B-4, C-1, D-3
Sedative, Hypnotic, and Anxiolytic Use Disorders Explanation: ***A-4, B-1, C-3, D-2***
- **Morphine** is contraindicated in **head injury** as it can increase intracranial pressure and mask neurological symptoms.
- **Amiodarone** is contraindicated in patients with **QT prolongation** due to its risk of inducing more severe arrhythmias like Torsades de Pointes.
- **Vigabatrin** is contraindicated during **pregnancy** due to its potential for teratogenicity and adverse effects on fetal development.
- **Estrogen preparations** are contraindicated in patients with a history of **thromboembolism** due to their increased risk of blood clot formation.
*A-1, B-3, C-2, D-4*
- This option incorrectly matches **Morphine** with QT prolongation and **Estrogen preparations** with head injury, which are not their primary contraindications.
- It also incorrectly links **Vigabatrin** with thromboembolism and **Amiodarone** with pregnancy.
*A-3, B-2, C-4, D-1*
- This choice incorrectly associates **Morphine** with pregnancy and **Vigabatrin** with head injury, which are not the most critical or direct contraindications.
- It also misaligns **Amiodarone** with thromboembolism and **Estrogen preparations** with QT prolongation.
*A-2, B-4, C-1, D-3*
- This option incorrectly matches **Morphine** with thromboembolism and **Amiodarone** with head injury, which are not their most significant contraindications.
- It also incorrectly links **Vigabatrin** with QT prolongation and **Estrogen preparations** with pregnancy.
Sedative, Hypnotic, and Anxiolytic Use Disorders Indian Medical PG Question 6: Which is NOT a common symptom of opioid withdrawal?
- A. Seizures (Correct Answer)
- B. Yawning
- C. Insomnia
- D. Diarrhea
Sedative, Hypnotic, and Anxiolytic Use Disorders Explanation: ***Seizures***
- Seizures are **not typical** of opioid withdrawal; they are more characteristic of withdrawal from substances like **alcohol** or **benzodiazepines**.
- Opioid withdrawal symptoms are primarily **autonomic** and **flu-like**, not neurological in the sense of causing seizures.
*Yawning*
- **Frequent yawning** is a common and early **autonomic symptom** of opioid withdrawal, indicating central nervous system overactivity.
- It is often accompanied by other signs of hyperarousal and discomfort.
*Insomnia*
- **Insomnia** (difficulty sleeping) is a very common and distressing symptom during opioid withdrawal due to heightened central nervous system activity and generalized discomfort.
- Patients often experience **restlessness** and an inability to achieve restful sleep.
*Diarrhea*
- **Diarrhea** is a prominent gastrointestinal symptom of opioid withdrawal, resulting from the cessation of opioid-induced slowing of gut motility.
- This symptom reflects the **autonomic hyperactivity** caused by opioid cessation.
Sedative, Hypnotic, and Anxiolytic Use Disorders Indian Medical PG Question 7: Shortest acting non benzodiazepine sedative is
- A. Zaleplon (Correct Answer)
- B. Eszopiclone
- C. Zopiclone
- D. Zolpidem
Sedative, Hypnotic, and Anxiolytic Use Disorders Explanation: ***Zaleplon***
- Has the shortest **half-life** (approximately 1 hour) among the non-benzodiazepine hypnotics, allowing for rapid elimination.
- This quick elimination makes it ideal for patients who have difficulty **falling asleep** but do not need prolonged sedation.
- Particularly useful for **middle-of-the-night** dosing due to its ultra-short duration.
*Eszopiclone*
- Has a half-life of about 6 hours, which is significantly longer than Zaleplon.
- It's the S-enantiomer of zopiclone and is used for both **sleep onset and maintenance**.
- Provides more sustained sleep throughout the night compared to Zaleplon.
*Zopiclone*
- Has a half-life of about 5-6 hours, which is considerably longer than Zaleplon.
- It's used for the short-term treatment of **insomnia** and helps both with sleep onset and maintenance.
- May cause a characteristic **bitter metallic taste** as a side effect.
*Zolpidem*
- Has a half-life of 2-3 hours, making it longer-acting than Zaleplon.
- It's commonly prescribed for problems with **sleep initiation** and occasionally for sleep maintenance.
- Available in extended-release formulations for prolonged action.
Sedative, Hypnotic, and Anxiolytic Use Disorders Indian Medical PG Question 8: A 45-year-old male with a history of chronic alcohol use is admitted to the hospital. He presents with anxiety, tremors, and agitation after his last drink 24 hours ago. Which of the following medications is most appropriate for controlling alcohol withdrawal symptoms?
- A. Lorazepam (Correct Answer)
- B. Fomepizole
- C. Disulfiram
- D. Buspirone
- E. Naltrexone
Sedative, Hypnotic, and Anxiolytic Use Disorders Explanation: ***Lorazepam***
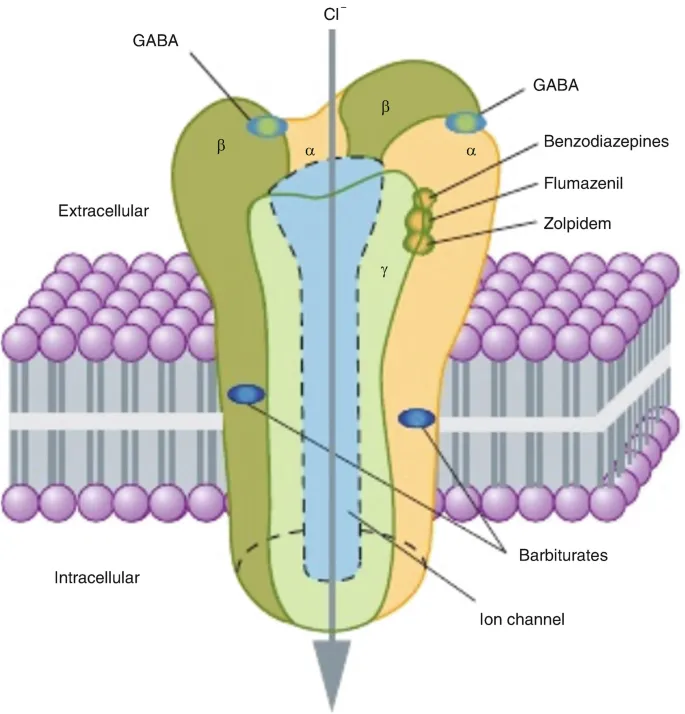
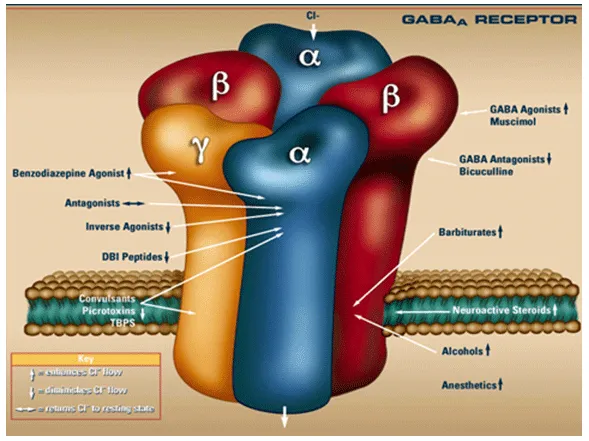
- **Lorazepam**, a **benzodiazepine**, is the first-line treatment for alcohol withdrawal symptoms due to its ability to enhance **GABAergic activity**, which is deficient during withdrawal.
- Its **intermediate half-life** and **lack of active metabolites** make it suitable for patients with liver impairment, common in chronic alcohol users.
*Fomepizole*
- **Fomepizole** is an antidote used to treat poisoning from **methanol** or **ethylene glycol**, not alcohol withdrawal.
- It works by inhibiting **alcohol dehydrogenase**, an enzyme involved in the metabolism of these toxic alcohols.
*Disulfiram*
- **Disulfiram** is an **aldehyde dehydrogenase inhibitor** used to deter alcohol consumption in recovering alcoholics by causing unpleasant reactions if alcohol is consumed.
- It is **not used to treat acute alcohol withdrawal symptoms** and can be dangerous if given during withdrawal due to potential interactions.
*Buspirone*
- **Buspirone** is an **anxiolytic** that acts as a **serotonin receptor agonist** and is used for generalized anxiety disorder.
- It is **ineffective for acute alcohol withdrawal** due to its slow onset of action and lack of anticonvulsant properties.
*Naltrexone*
- **Naltrexone** is an **opioid receptor antagonist** used for relapse prevention and reducing alcohol craving in patients with alcohol use disorder.
- It is **not effective for acute alcohol withdrawal symptoms** and does not prevent seizures or delirium tremens, which are life-threatening complications of withdrawal.
Sedative, Hypnotic, and Anxiolytic Use Disorders Indian Medical PG Question 9: Which anxiolytic acts through 5-HT1A receptor partial agonism without exhibiting significant anticonvulsant or muscle relaxant properties?
- A. Diazepam
- B. Zolpidem
- C. Phenobarbitone
- D. Buspirone (Correct Answer)
Sedative, Hypnotic, and Anxiolytic Use Disorders Explanation: ***Buspirone***
- **Buspirone** is a unique anxiolytic that primarily acts as a **partial agonist at 5-HT1A receptors**.
- Unlike benzodiazepines, it lacks significant **anticonvulsant**, **muscle relaxant**, or **sedative-hypnotic properties** and does not lead to physical dependence or withdrawal.
*Diazepam*
- **Diazepam** is a **benzodiazepine** that acts by enhancing the effect of **GABA** at GABA-A receptors, leading to significant anxiolytic, sedative, muscle relaxant, and anticonvulsant effects.
- It does not primarily act via **5-HT1A receptor partial agonism**.
*Zolpidem*
- **Zolpidem** is a **non-benzodiazepine hypnotic** that selectively binds to the **GABA-A receptor** subunit, primarily mediating sedative effects.
- While it's used for insomnia, it doesn't primarily act as a **5-HT1A partial agonist** and is not typically used for its anxiolytic properties in the same way as buspirone.
*Phenobarbitone*
- **Phenobarbitone** is a **barbiturate** that acts by prolonging the opening of **chloride channels** associated with GABA-A receptors, leading to strong sedative, hypnotic, and anticonvulsant effects.
- Its mechanism of action is distinct from **5-HT1A receptor partial agonism**, and it carries a high risk of dependence and overdose.
Sedative, Hypnotic, and Anxiolytic Use Disorders Indian Medical PG Question 10: A person presents to the outpatient department with tremors and visual hallucinations after a 2-day history of alcohol cessation. What is the diagnosis?
- A. Korsakoff’s psychosis
- B. Delirium tremens (Correct Answer)
- C. Wernicke encephalopathy
- D. Alcoholic hallucinosis
Sedative, Hypnotic, and Anxiolytic Use Disorders Explanation: ***Delirium tremens***
- Delirium tremens is a severe form of **alcohol withdrawal** characterized by **tremors**, disorientation, and **visual hallucinations**, typically appearing **48 to 96 hours** (2-4 days) after the last drink.
- This is a medical emergency with potential for **seizures**, **hyperthermia**, and **cardiovascular collapse** due to dysregulation of neurotransmitters (decreased **GABA** activity and increased **glutamate** activity).
- Autonomic hyperactivity (tachycardia, hypertension, diaphoresis) is a key feature distinguishing it from other alcohol-related conditions.
*Korsakoff's psychosis*
- This is a chronic **neuropsychiatric syndrome** typically occurring after an episode of **Wernicke encephalopathy**, characterized by severe **memory impairment** (anterograde and retrograde amnesia) and **confabulation**.
- It develops over weeks to months in the course of chronic alcoholism and is **not an acute withdrawal syndrome**, unlike the symptoms described in this 2-day presentation.
*Wernicke encephalopathy*
- This is an acute neurological condition caused by **thiamine (vitamin B1) deficiency**, commonly seen in chronic alcoholics, characterized by the classic triad of **ophthalmoplegia** (especially nystagmus), **ataxia**, and **confusion**.
- While it can precede Korsakoff's psychosis and involves confusion, it does not typically present with the prominent **tremors** and **visual hallucinations** characteristic of alcohol withdrawal, and the timing (2 days post-cessation) points more toward withdrawal rather than nutritional deficiency.
*Alcoholic hallucinosis*
- Alcoholic hallucinosis involves primarily **auditory hallucinations** (often threatening voices) that occur without significant clouding of consciousness, typically within **12-24 hours** of alcohol cessation.
- Unlike delirium tremens, it **lacks autonomic instability**, severe tremors, and global disorientation, and the hallucinations are predominantly auditory rather than visual.
More Sedative, Hypnotic, and Anxiolytic Use Disorders Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.