Occupational Lung Diseases Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Occupational Lung Diseases. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Occupational Lung Diseases Indian Medical PG Question 1: Which of the following is false regarding respirable dust:
- A. May lead to pneumoconiosis
- B. Silicosis is the most common dust disease
- C. Smaller than 5 microns is respirable
- D. Soluble dust remains in the lungs for a long time (Correct Answer)
Occupational Lung Diseases Explanation: ***Soluble dust remains in the lungs for a long time***
- This statement is false because soluble dusts are **rapidly cleared** from the lungs through dissolution and absorption into the bloodstream or through mucociliary clearance.
- Their solubility means they do not persist in the lung tissue long enough to cause significant chronic fibrotic changes.
*May lead to pneumoconiosis*
- **Inhalable dusts**, particularly those that are insoluble and durable, can accumulate in the lungs and lead to various forms of **pneumoconiosis**, which are interstitial lung diseases.
- Examples include **silicosis**, **asbestosis**, and **coal workers' pneumoconiosis**.
*Silicosis is the most common dust disease*
- **Silicosis** is indeed one of the **most prevalent occupational lung diseases** globally due to widespread exposure to **crystalline silica** in various industries.
- It is a chronic, progressive pneumoconiosis caused by the inhalation of respirable silica dust.
*Smaller than 5 microns is repairable*
- Dust particles **smaller than 5-10 microns** (often referred to as respirable dust) are capable of reaching the **alveolar region** of the lungs.
- Particles of this size are the most problematic because they can evade the upper respiratory tract's defense mechanisms and deposit deep within the lungs, leading to long-term health effects.
Occupational Lung Diseases Indian Medical PG Question 2: Which of the following organisms plays an important role in the pathogenesis of "malt worker's lung"?
- A. Aspergillus clavatus (Correct Answer)
- B. Pseudomonas
- C. Micropolyspora faeni
- D. Aspergillus fumigatus
Occupational Lung Diseases Explanation: ***Aspergillus clavatus***
- **Aspergillus clavatus** is the specific causative agent of **malt worker's lung**, a form of hypersensitivity pneumonitis (extrinsic allergic alveolitis)
- It thrives in the **moist, warm conditions of germinating barley**, where malt workers are exposed to its spores during the malting process
- This occupational exposure leads to an immunologic reaction in the lungs
*Aspergillus fumigatus*
- While *Aspergillus fumigatus* is a common cause of various aspergillosis syndromes (e.g., allergic bronchopulmonary aspergillosis, invasive aspergillosis), it is **not** typically associated with malt worker's lung
- It is more broadly distributed in organic matter but not specifically linked to the malt industry in this context
*Pseudomonas*
- *Pseudomonas* species are **gram-negative bacteria**, often associated with nosocomial infections, cystic fibrosis, or chronic lung infections
- They are **not fungi** and do not play a role in this specific allergic lung disease or hypersensitivity pneumonitis
*Micropolyspora faeni*
- *Micropolyspora faeni* (now reclassified as *Saccharopolyspora rectivirgula*) is the causative agent of **farmer's lung**, another type of hypersensitivity pneumonitis
- It is found in **moldy hay**, not in malted barley, and therefore does not cause malt worker's lung
Occupational Lung Diseases Indian Medical PG Question 3: Which of the following is a common use of asbestos in construction?
- A. Painting
- B. Bakery
- C. Cement production (Correct Answer)
- D. Cotton industry
Occupational Lung Diseases Explanation: ***Cement production***
- **Asbestos fibers** were commonly added to cement products, such as **asbestos-cement sheets** and pipes, to enhance their **strength** and durability.
- Its **heat-resistant** and **insulating properties** also made it ideal for fireproofing and reinforcing cement structures.
*Painting*
- Asbestos was rarely used in paints; common additives for texture or strength in paint typically did not include asbestos.
- The primary function of paint is decorative and protective, for which asbestos did not offer significant functional advantages.
*Bakery*
- Asbestos has no logical or historical use in the bakery industry, which involves food preparation and requires materials that are safe for consumption and food contact.
- Any inclusion of asbestos in this context would be highly toxic and severely regulated.
*Cotton industry*
- The cotton industry primarily deals with textile production from natural fibers and does not typically incorporate asbestos.
- While asbestos was used in some textiles for fire resistance (e.g., firefighters' gear), it was not a common additive in the general cotton industry.
Occupational Lung Diseases Indian Medical PG Question 4: NOT a cause of bacterial community acquired pneumonia:
- A. Streptococcus pneumoniae
- B. Mycoplasma pneumoniae
- C. Blastomyces (Correct Answer)
- D. Moraxella catarrhalis
Occupational Lung Diseases Explanation: ***Blastomyces***
- *Blastomyces*, a **dimorphic fungus**, causes **blastomycosis**, which is a **fungal infection**, not a bacterial infection.
- While it can cause community-acquired pneumonia with pulmonary symptoms, it is **NOT a bacterial pathogen** and therefore not a cause of **bacterial community-acquired pneumonia**.
- The question asks specifically about bacterial causes, making this the correct answer.
*Streptococcus pneumoniae*
- **_Streptococcus pneumoniae_** is the **most common bacterial cause** of **community-acquired pneumonia (CAP)**.
- Infection typically presents with **acute onset** of fever, chills, productive cough, and lobar consolidation on chest X-ray.
*Mycoplasma pneumoniae*
- **_Mycoplasma pneumoniae_** is a common cause of **atypical bacterial community-acquired pneumonia**, often referred to as "**walking pneumonia**".
- It typically causes milder symptoms, including a **persistent dry cough** and malaise, and is prevalent in younger adults and children.
*Moraxella catarrhalis*
- **_Moraxella catarrhalis_** is a **bacterial pathogen** that causes **community-acquired pneumonia**, especially in patients with **chronic obstructive pulmonary disease (COPD)**.
- It can also cause **bronchitis**, otitis media, and sinusitis.
Occupational Lung Diseases Indian Medical PG Question 5: Match the following: A) Caplan syndrome- 1) Found first in coal worker B) Asbestosis- 2) Upper lobe predominance C) Mesothelioma- 3) Involves lower lobe D) Sarcoidosis- 4) Pleural effusion is seen
- A. A-3, B-4, C-2, D-1
- B. A-1, B-4, C-3, D-2 (Correct Answer)
- C. A-4, B-2, C-3, D-1
- D. A-2, B-4, C-3, D-1
Occupational Lung Diseases Explanation: **A-1, B-4, C-3, D-2**
- **Caplan syndrome** was first described in **coal workers** with **rheumatoid arthritis** and progressive massive fibrosis.
- **Asbestosis** is often associated with **pleural effusion**, which can be benign or malignant.
- **Mesothelioma** typically involves the **lower lobes** of the lungs, specifically the pleura, and is strongly linked to asbestos exposure.
- **Sarcoidosis** is characterized by **non-caseating granulomas**, which have a predilection for the **upper lobes** of the lungs.
*A-3, B-4, C-2, D-1*
- This option incorrectly states that Caplan syndrome involves the lower lobe; **Caplan syndrome** is defined by the presence of large nodules in the lungs of coal workers with rheumatoid arthritis, and their specific lobar distribution is not a defining characteristic.
- This option incorrectly states that Mesothelioma has an upper lobe predominance; **Mesothelioma** is a pleural malignancy and typically involves the **lower lobes**, extending along the pleura.
*A-4, B-2, C-3, D-1*
- This option incorrectly associates Caplan syndrome with pleural effusion; **Caplan syndrome** manifests as rheumatoid nodules in the lungs, not primarily pleural effusion.
- This option incorrectly states that Asbestosis has an upper lobe predominance; **Asbestosis** predominantly affects the **lower lobes** of the lungs, causing interstitial fibrosis.
*A-2, B-4, C-3, D-1*
- This option incorrectly states that Caplan syndrome has an upper lobe predominance; the defining feature of **Caplan syndrome** is the combination of rheumatoid arthritis and pneumoconiosis, not specific lobar involvement.
- This option correctly identifies pleural effusion with asbestosis and lower lobe involvement with mesothelioma, but **Caplan syndrome** is not characterized by upper lobe predominance.
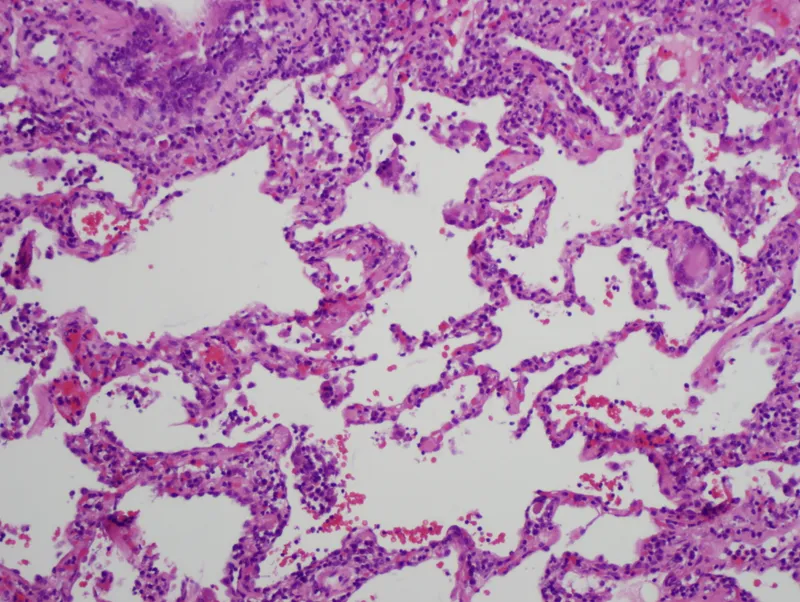
Occupational Lung Diseases Indian Medical PG Question 6: A 35-year-old woman with a long history of dyspnea, chronic cough, sputum production, and wheezing dies of respiratory failure following a bout of lobar pneumonia. She was not a smoker or an alcoholic. Which of the following underlying conditions is most likely associated with the pathologic changes shown in the lung autopsy?
- A. Antibodies against type 4 collagen (associated with Goodpasture syndrome)
- B. Cystic fibrosis (a genetic disorder affecting the lungs)
- C. Mutation in dynein arms (associated with primary ciliary dyskinesia)
- D. Alpha-1 antitrypsin deficiency (Correct Answer)
Occupational Lung Diseases Explanation: ***Alpha 1 antitrypsin deficiency***
- This condition leads to **accumulation of abnormal protein** in the liver and lungs, resulting in emphysema, which is consistent with chronic cough and dyspnea [1].
- Patients often develop **lung pathology** similar to what is seen in smokers, making it plausible given the patient's background [1].
*Mutation in dynein arms*
- This is associated with **primary ciliary dyskinesia**, which presents with recurrent respiratory infections but is not typical in non-smokers or in the context of **dyspnea with chronic cough**.
- Usually linked to **situs inversus** and **recurrent infections**, neither of which is highlighted here.
*Antibodies against type 4 collagen*
- This condition is related to **Goodpasture syndrome**, which typically results in **hemoptysis** and **renal failure**, rather than chronic cough and sputum production.
- The predominant involvement in this syndrome does not align with the clinical presentation of **chronic lung disease** noted in this patient.
*Cystic fibrosis*
- While it causes **chronic respiratory symptoms**, it is usually seen in younger patients and is associated with **pancreatic insufficiency** and **salty sweat**.
- The age of the patient and symptom progression does not fit well with a diagnosis of cystic fibrosis.
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lung, pp. 683-684.
Occupational Lung Diseases Indian Medical PG Question 7: A CT scan shows the 'crazy paving' pattern in both lungs. Which bronchoalveolar lavage finding would confirm pulmonary alveolar proteinosis?
- A. Milky fluid with PAS-positive material (Correct Answer)
- B. Hemosiderin-laden macrophages
- C. Eosinophilia >25%
- D. CD4/CD8 ratio >3.5
Occupational Lung Diseases Explanation: ***Milky fluid with PAS-positive material***
- A **milky, turbid bronchoalveolar lavage (BAL) fluid** is characteristic of **pulmonary alveolar proteinosis (PAP)** due to the accumulation of lipoproteinaceous material [1].
- **Periodic Acid-Schiff (PAS) staining** confirms the presence of this **glycoprotein-rich surfactant material**, which reacts positively [1].
*Hemosiderin-laden macrophages*
- These are indicative of **pulmonary hemorrhage**, not PAP.
- They are commonly seen in conditions like **Goodpasture syndrome** or **idiopathic pulmonary hemosiderosis**.
*Eosinophilia >25%*
- Significant **eosinophilia in BAL fluid** is a hallmark of **eosinophilic pneumonia**, a different interstitial lung disease.
- It suggests an **allergic or hypersensitivity reaction** in the lungs.
*CD4/CD8 ratio >3.5*
- An **elevated CD4/CD8 ratio** in BAL fluid is highly suggestive of **sarcoidosis**, a granulomatous inflammatory disease.
- This ratio reflects the **lymphocyte population** in the alveoli, not lipoproteinaceous accumulation.
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lung, pp. 703-705.
Occupational Lung Diseases Indian Medical PG Question 8: Ferruginous bodies are seen in:
- A. Silicosis
- B. Asbestosis (Correct Answer)
- C. Byssinosis
- D. Bagassosis
Occupational Lung Diseases Explanation: ***Asbestosis***
- Ferruginous bodies are specifically associated with **exposure to asbestos**, which leads to asbestosis [1].
- These bodies are seen as **siderophilic structures** resembling a "dumbbell" shape under the microscope, which are indicative of this condition [1].
*Bagassosis*
- Caused by exposure to **bagasse dust**, primarily from sugarcane, leading to allergic alveolitis rather than ferruginous bodies [1].
- Histopathology typically shows **lymphocytic infiltration** and non-caseating granulomas, not ferruginous bodies.
*Byssinosis*
- This is associated with inhalation of **cotton dust** and primarily results in **bronchoconstriction** and respiratory symptoms rather than ferruginous bodies.
- Characterized by a **respiratory illness** that worsens at the beginning of the work week, missing the key features of asbestosis.
*Silicosis*
- Resulting from exposure to **silica dust**, this condition leads to macules and nodules in the lungs instead of ferruginous bodies [1].
- The hallmark findings are **hyaline nodules** on imaging and not the abnormal iron-containing structures seen in asbestosis.
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lung, pp. 695, 698-699.
Occupational Lung Diseases Indian Medical PG Question 9: Small deposits of neuroendocrine cell hyperplasia in scarred lungs are known as:
- A. Teratoma
- B. Tumorlet (Correct Answer)
- C. Carcinoid
- D. Hamartoma
Occupational Lung Diseases Explanation: ***Tumorlet***
- Small deposits of **neuroendocrine cell hyperplasia** in scarred lungs are specifically referred to as tumorlets, which can be associated with various lung diseases.
- Tumorlets are typically benign, comprising **small clusters of neuroendocrine cells** that are usually found in pulmonary scars.
*Teratoma*
- Teratomas are **germ cell tumors** that typically contain tissue from all three embryonic layers and are not associated with neuroendocrine cell hyperplasia.
- They usually occur in **gonadal** sites or mediastinum and do not relate to scarring in lung tissue.
*Carcinoid*
- Carcinoids are **neuroendocrine tumors** but larger and more defined than tumorlets, often causing obstruction or symptoms.
- Unlike tumorlets, carcinoids present as **solitary masses**, typically found in the gastrointestinal tract or lungs but not as small deposits in scarred tissue.
*Hamartoma*
- Hamartomas are benign tumors made of **disorganized tissue** native to the organ in which they arise, but they do not involve neuroendocrine cells specifically [1].
- They are generally characterized as **well-circumscribed** nodules and do not correlate with neuroendocrine hyperplasia in scarred lungs [1].
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lung, pp. 727-728.
Occupational Lung Diseases Indian Medical PG Question 10: Hypersensitivity pneumonitis due to prolonged inhalation of dust is a characteristic feature of Maltworker's lung, which is caused by:
- A. Aspergillus clavatus (Correct Answer)
- B. Pseudomonas
- C. Micropolyspora faeni
- D. Aspergillus fumigatus
Occupational Lung Diseases Explanation: ***Aspergillus clavatus***
- **Maltworker's lung** is a specific type of hypersensitivity pneumonitis caused by repeated inhalation of dust from moldy barley, which often contains **Aspergillus clavatus**.
- This leads to an **immunological reaction** in the lungs, manifesting as granulomatous inflammation [4].
*Aspergillus fumigatus*
- While **Aspergillus fumigatus** is a common cause of lung infections, it is primarily associated with conditions like **allergic bronchopulmonary aspergillosis (ABPA)** and invasive aspergillosis, not specifically Maltworker's lung [1].
- ABPA involves type I and type III hypersensitivity reactions to *A. fumigatus* colonization in the airways, distinct from the hypersensitivity pneumonitis seen in Maltworker's lung [2].
*Pseudomonas*
- **Pseudomonas** species are gram-negative bacteria, primarily known for causing opportunistic infections, particularly in immunocompromised individuals or those with cystic fibrosis.
- They are not a fungal organism and are not associated with hypersensitivity pneumonitis like Maltworker's lung; rather, they cause acute and chronic bacterial pneumonia.
*Micropolyspora faeni*
- **Micropolyspora faeni** (now *Saccharopolyspora rectivirgula*) is the causative agent of **Farmer's lung**, another form of hypersensitivity pneumonitis [3].
- **Farmer's lung** is distinct from Maltworker's lung, occurring due to exposure to moldy hay rather than moldy barley [3].
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Infectious Diseases, pp. 396-397.
[2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Respiratory Tract Disease, pp. 329-330.
[3] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Respiratory Tract Disease, pp. 332-333.
[4] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Lung, pp. 701-702.
More Occupational Lung Diseases Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.


 Hilar 'egg-shell' calcification.
Hilar 'egg-shell' calcification.