Hemodynamic Disorders Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Hemodynamic Disorders. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Hemodynamic Disorders Indian Medical PG Question 1: Which of the following conditions is primarily associated with stasis as a cause of thrombosis?
- A. Polycythemia
- B. Dehydration
- C. Sickle cell anemia
- D. Venous stasis (Correct Answer)
Hemodynamic Disorders Explanation: ***All of the above***
- Stasis can contribute to **thrombosis in various conditions**, including polycythemia, as it increases blood viscosity, and in sickle cell anemia due to impaired blood flow [2].
- **Venous circulation** is particularly affected by stasis, as it leads to venous thromboembolism, making it a critical factor in thrombosis [1].
*Polycythemia*
- While **polycythemia** leads to increased blood viscosity, stasis itself isn't the primary mechanism for thrombosis in this condition.
- Thrombosis in polycythemia is more due to *hyperviscosity* rather than stasis alone.
*Venous circulation*
- While stasis is indeed significant in **venous circulation**, it does not capture the full spectrum of thrombosis causes in the context of various conditions [1].
- Other factors such as **hypercoagulability** and **vascular injury** also contribute, making it not solely reliant on stasis [1].
*Sickle cell Anemia*
- Thrombosis in sickle cell anemia occurs mainly due to **occlusion** from sickled cells, rather than stasis leading to thrombus formation [2].
- While stasis can occur, it is not the principal cause of thrombosis in this disease [2].
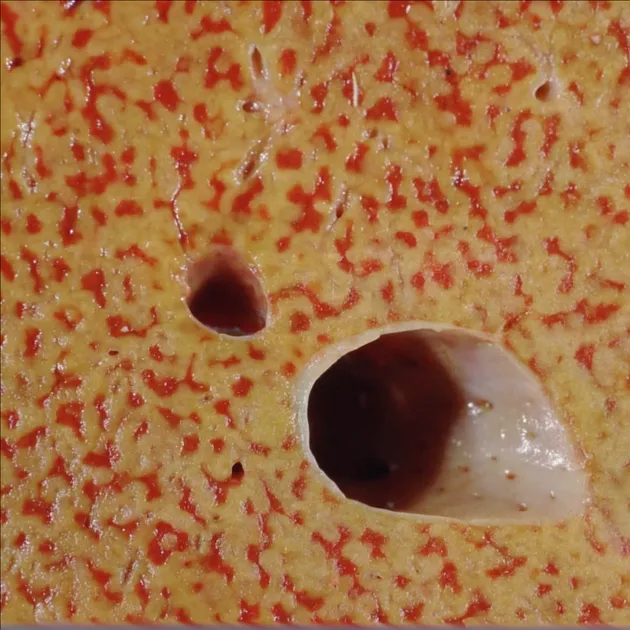
Hemodynamic Disorders Indian Medical PG Question 2: White infarcts are seen in which of the following?
- A. Heart
- B. Kidney
- C. All of the options
- D. Spleen (Correct Answer)
Hemodynamic Disorders Explanation: ***Spleen***
- The spleen is the **classic example** of an organ that develops **white (anemic) infarcts** [1]
- White infarcts occur in **solid organs with end-arterial blood supply** and limited collateral circulation [1]
- Splenic infarcts appear as **pale, wedge-shaped areas** of coagulative necrosis [1], [2]
- Typically caused by **embolic events** (e.g., infective endocarditis, atrial fibrillation, hypercoagulable states) [3], [4]
- The dense parenchyma prevents blood extravasation, resulting in pale appearance [1]
*Kidney*
- While the kidney also develops white infarcts due to its end-arterial circulation, the **spleen** is the more classic textbook example [1]
- Renal infarcts similarly present as pale, wedge-shaped areas but are less frequently emphasized in standard teaching [1], [2]
*Heart*
- Myocardial infarctions **initially present as RED (hemorrhagic) infarcts**, not white infarcts
- This occurs due to reperfusion through anastomotic channels and hemorrhage into necrotic tissue [1]
- The heart only develops pale appearance **after several days** when blood is resorbed
- Therefore, heart is **not** a typical site for white infarcts
*All of the options*
- Incorrect because the heart characteristically develops **red infarcts**, not white infarcts
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Hemodynamic Disorders, Thromboembolic Disease, and Shock, p. 140.
[2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. (Basic Pathology) introduces the student to key general principles of pathology, both as a medical science and as a clinical activity with a vital role in patient care. Part 2 (Disease Mechanisms) provides fundamental knowledge about the cellular and molecular processes involved in diseases, providing the rationale for their treatment. Part 3 (Systematic Pathology) deals in detail with specific diseases, with emphasis on the clinically important aspects., pp. 148-149.
[3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Hemodynamic Disorders, Thromboembolic Disease, and Shock, pp. 136-137.
[4] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. (Basic Pathology) introduces the student to key general principles of pathology, both as a medical science and as a clinical activity with a vital role in patient care. Part 2 (Disease Mechanisms) provides fundamental knowledge about the cellular and molecular processes involved in diseases, providing the rationale for their treatment. Part 3 (Systematic Pathology) deals in detail with specific diseases, with emphasis on the clinically important aspects., pp. 145-146.
Hemodynamic Disorders Indian Medical PG Question 3: Which type of necrosis is characterized by deposition of immune complexes and fibrin in the walls of blood vessels?
- A. Liquefactive necrosis
- B. Coagulative necrosis
- C. Caseous necrosis
- D. Fibrinoid necrosis (Correct Answer)
Hemodynamic Disorders Explanation: ***Fibrinoid necrosis***
- This type of necrosis is classically associated with **immune-mediated vascular damage**, where antigen-antibody complexes are deposited in arterial walls [2].
- The microscopic appearance is characterized by bright pink, amorphous material composed of **fibrin and immune complexes**, giving a fibrin-like staining pattern [1].
*Liquefactive necrosis*
- Characterized by the **dissolution of dead cells into a viscous liquid mass**, often seen in bacterial infections or brain infarcts.
- The necrotic tissue is replaced by inflammatory cells and fluid, rather than immune complex deposits.
*Coagulative necrosis*
- Occurs due to **ischemia**, leading to protein denaturation and preservation of cell outlines for a period.
- It does not involve the deposition of immune complexes or fibrin in vessel walls.
*Caseous necrosis*
- A form of coagulative necrosis associated with **tuberculosis**, characterized by a friable, "cheese-like" appearance.
- It primarily involves granulomatous inflammation and macrophage accumulation, not immune complex deposition in blood vessels.
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of Infancy and Childhood, pp. 514-518.
[2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Diseases of the Immune System, pp. 214-242.
Hemodynamic Disorders Indian Medical PG Question 4: What is the primary cause of edema in nephritic syndrome?
- A. Decreased plasma protein concentration
- B. Reduced plasma osmotic pressure
- C. Increased plasma protein concentration
- D. Sodium and water retention (Correct Answer)
Hemodynamic Disorders Explanation: ***Sodium and water retention***
- In nephritic syndrome, **sodium and water retention** occurs due to kidney inflammation, leading to fluid overload [1].
- This results in increased **blood volume**, causing edema as a key clinical feature [1].
*Increased in plasma protein concentration*
- Nephritic syndrome typically leads to **decreased**, not increased, plasma protein levels due to proteinuria.
- Higher plasma protein levels would not contribute to edema; in fact, they would do the opposite by promoting osmotic balance.
*Reduced plasma osmotic pressure*
- While reduced osmotic pressure contributes to edema, in nephritic syndrome, the main factor is sodium and water retention [1].
- This oes not accurately describe the underlying cause in nephritic syndrome.
*Decreased in plasma protein concentration*
- Although nephritic syndrome may involve decreased protein concentration, edema is primarily due to **fluid retention** [1].
- Directly stating decreased plasma proteins oversimplifies the dynamic fluid balance that is disrupted in nephritic syndrome.
Hemodynamic Disorders Indian Medical PG Question 5: Which of the following is not typically seen in Disseminated Intravascular Coagulation (DIC)?
- A. Thrombocytopenia
- B. PT elevation
- C. Fibrinogen decreased
- D. Normal aPTT (Correct Answer)
Hemodynamic Disorders Explanation: ***Normal APTT***
- In Disseminated Intravascular Coagulation (**DIC**), **APTT** is typically **prolonged** due to consumption of clotting factors [1].
- The presence of normal APTT indicates that coagulation pathways are not significantly affected, which is contrary to what is seen in DIC.
*Fibrinogen decreased*
- **Decreased fibrinogen levels** are common in DIC, reflecting its consumption during the coagulation process [1].
- This depletion is linked to the increased clotting and is a hallmark of DIC, making this statement false in the context of the question.
*Thrombocytopenia*
- **Thrombocytopenia** occurs in DIC as platelets are consumed during the formation of microclots [1].
- A significant drop in platelet count is a key feature of DIC, therefore this statement does not align with the "except" clause.
*PT elevation*
- Prothrombin Time (**PT**) is usually **elevated** in DIC due to the consumption of clotting factors [1].
- This reflects the ongoing activation of the coagulation cascade, supporting the exclusion in the question context.
**References:**
[1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Blood And Bone Marrow Disease, pp. 625-626.
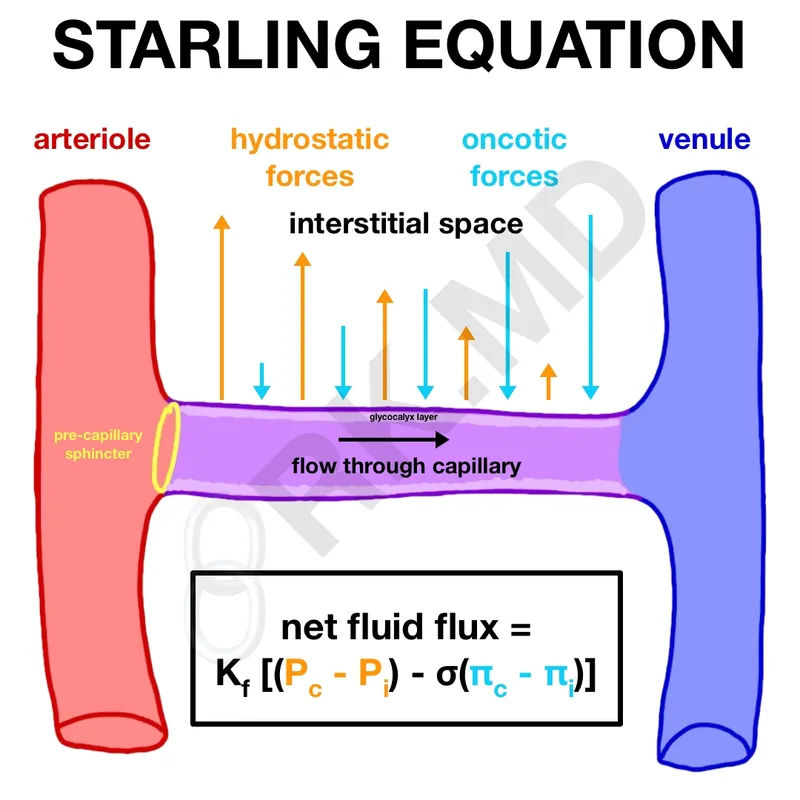
Hemodynamic Disorders Indian Medical PG Question 6: Which of the following factors most directly contributes to the development of edema in patients with nephrotic syndrome?
- A. Increased capillary permeability
- B. Hypertension
- C. Hypernatremia
- D. Hypoalbuminemia (Correct Answer)
Hemodynamic Disorders Explanation: Hypoalbuminemia
- Nephrotic syndrome is defined by significant proteinuria leading to a decrease in serum albumin levels [2].
- Albumin is the primary protein responsible for maintaining oncotic pressure within the capillaries, and its deficiency (<3 g/dL) leads to fluid shifts from the intravascular space to the interstitial space, causing edema [1], [2].
Increased capillary permeability
- While increased capillary permeability can cause edema, it is not the primary mechanism in nephrotic syndrome.
- In nephrotic syndrome, the problem is loss of protein from the capillaries, rather than the capillaries themselves becoming excessively leaky to fluid in general.
Hypertension
- Hypertension can exacerbate edema by raising hydrostatic pressure, but it is not the initial or primary cause of edema in nephrotic syndrome [1].
- Edema in nephrotic syndrome can occur even in normotensive patients due to severe hypoalbuminemia [2].
Hypernatremia
- Hypernatremia indicates high sodium levels in the blood, which would typically cause water to shift into the intravascular space, thus drawing fluid out of the interstitial space.
- In actuality, patients with nephrotic syndrome often experience some degree of sodium retention, which contributes to fluid overload, but it is not the most direct cause of fluid moving from the capillaries into the interstitial tissue [3].
Hemodynamic Disorders Indian Medical PG Question 7: A liver biopsy shows 'nutmeg' pattern. Which additional finding would best support chronic passive congestion?
- A. Bridging fibrosis
- B. Sinusoidal dilatation (Correct Answer)
- C. Mallory bodies
- D. Ground glass hepatocytes
Hemodynamic Disorders Explanation: ***Sinusoidal dilatation***
- **Sinusoidal dilatation** is the **characteristic microscopic feature** of **chronic passive congestion** of the liver, directly responsible for the "nutmeg" appearance [1].
- This dilatation occurs due to increased venous pressure from right-sided heart failure, causing blood to back up into the **hepatic sinusoids**, particularly in **Zone 3 (centrilobular)** around the central veins [3].
- On gross examination, the alternating pattern of congested red-brown centrilobular areas and pale periportal areas creates the classic **nutmeg liver** appearance [1], [2].
*Bridging fibrosis*
- **Bridging fibrosis** is a feature of **advanced/late-stage chronic passive congestion**, sometimes called **cardiac cirrhosis** or **cardiac sclerosis** [3].
- While long-standing congestion can eventually lead to centrilobular necrosis and fibrosis, **sinusoidal dilatation** is the **primary and early finding** that best supports the diagnosis.
- Bridging fibrosis takes months to years to develop and represents chronic injury, not the acute/characteristic finding [3].
*Mallory bodies*
- **Mallory bodies** (Mallory-Denk bodies) are diagnostic hallmarks of **alcoholic hepatitis** or **non-alcoholic steatohepatitis (NASH)**.
- They represent aggregates of **intermediate filaments** (cytokeratin) within hepatocytes, unrelated to vascular congestion.
*Ground glass hepatocytes*
- **Ground-glass hepatocytes** are indicative of **chronic hepatitis B virus infection**, representing accumulated **hepatitis B surface antigen (HBsAg)** in the endoplasmic reticulum.
- This finding is completely unrelated to **vascular congestion** or the nutmeg liver pattern.
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Hemodynamic Disorders, Thromboembolic Disease, and Shock, p. 126.
[2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 401-402.
[3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Liver and Gallbladder, pp. 870-872.
Hemodynamic Disorders Indian Medical PG Question 8: A 50-year-old patient presents with dyspnea, edema, and an elevated JVP. Which condition is most likely?
- A. Right heart failure (Correct Answer)
- B. Left heart failure
- C. Pneumonia
- D. Asthma
Hemodynamic Disorders Explanation: ***Right heart failure***
- **Dyspnea**, **edema** (often peripheral), and an **elevated jugular venous pressure (JVP)** are classical signs of right heart failure due to systemic venous congestion [1].
- The inability of the right ventricle to pump blood efficiently leads to blood backing up in the systemic circulation [3].
*Left heart failure*
- While it can cause dyspnea, left heart failure primarily leads to **pulmonary congestion** (e.g., crackles, orthopnea) and is less directly associated with prominent peripheral edema and elevated JVP as initial prominent symptoms [2].
- An elevated JVP and significant peripheral edema in left heart failure typically indicate progression to **biventricular failure** [1].
*Pneumonia*
- Pneumonia typically presents with acute symptoms like **fever, cough with sputum, pleuritic chest pain**, and localized lung findings, rather than chronic dyspnea, edema, and elevated JVP.
- It’s an **infectious lung condition**, not primarily a circulatory disorder causing systemic congestion.
*Asthma*
- Asthma is a **reversible obstructive airway disease** characterized by episodic **wheezing, cough, and shortness of breath** due to bronchospasm [4].
- It does not typically cause edema or an elevated JVP.
Hemodynamic Disorders Indian Medical PG Question 9: Pulmonary embolism is most commonly caused by:
- A. Deep vein thrombosis (DVT) of the leg (Correct Answer)
- B. Fat embolism from pelvic fracture
- C. Cardiac emboli from heart disease
- D. Increased pulmonary pressure (a consequence of PE)
Hemodynamic Disorders Explanation: ***Deep vein thrombosis (DVT) of the leg***
- **Deep vein thrombosis (DVT)** in the leg is the most common source of emboli that travel to the lungs, leading to pulmonary embolism [1].
- The thrombus breaks off from the deep veins, typically in the **lower extremities**, and propagates through the venous system to the pulmonary arteries [1].
*Increased pulmonary pressure (a consequence of PE)*
- **Increased pulmonary pressure** is a physiological consequence of a significant pulmonary embolism, as blood flow is obstructed, but it is not the cause of the embolism itself.
- This option describes a **downstream effect**, rather than the origin of the embolus.
*Fat embolism from pelvic fracture*
- **Fat embolisms** can occur after long bone fractures (especially pelvic or femur fractures) and surgeries, but they are a less common cause of PE compared to DVT.
- While they can lead to pulmonary symptoms, the mechanism involves **fat globules** entering the circulation, distinct from a thrombus.
*Cardiac emboli from heart disease*
- **Cardiac emboli** typically originate from the heart (e.g., from atrial fibrillation, mural thrombi after myocardial infarction, or valvular disease) and usually cause **systemic emboli** leading to strokes or limb ischemia.
- While rare, paradoxal emboli can occur via a patent foramen ovale but are not the leading cause of "pulmonary" embolism.
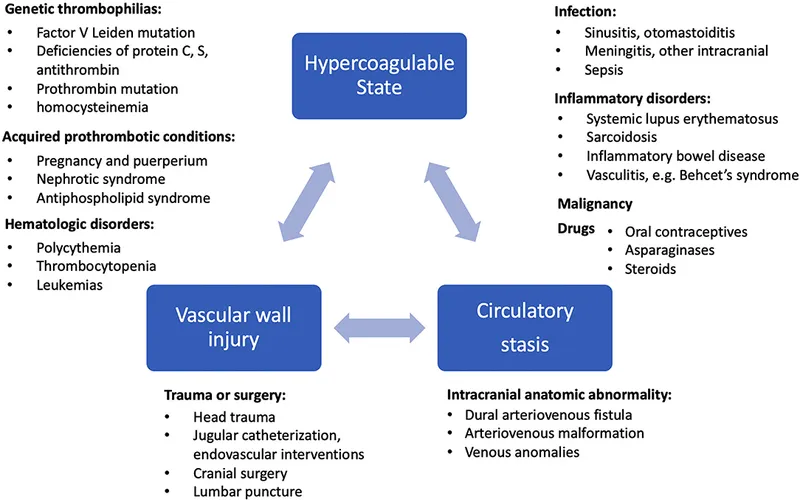
Hemodynamic Disorders Indian Medical PG Question 10: Virchow's triad includes all except:-
- A. Stasis of blood flow
- B. Endothelial injury
- C. Platelet thrombus (Correct Answer)
- D. Hypercoagulability
Hemodynamic Disorders Explanation: ***Platelet thrombus***
- Virchow's triad describes the three primary categories of factors that are thought to contribute to **thrombosis**, but it does not specifically include a formed **thrombus** itself. [1]
- While **platelet thrombus** formation is an outcome of an imbalance in these factors, it is not one of the predisposing conditions identified by Virchow's triad.
*Stasis of blood flow*
- **Stasis** refers to a reduction in the rate of blood flow, which allows clotting factors to accumulate and endothelial cells to become hypoxic, increasing the risk of **thrombosis**. [1]
- This is a well-established component of Virchow's triad, explaining why factors like immobility or venous insufficiency predispose to clot formation.
*Endothelial injury*
- **Endothelial injury** or dysfunction exposes the subendothelial collagen, leading to platelet adhesion and activation, and the initiation of the coagulation cascade. [1]
- It is a critical component of Virchow's triad, often seen in conditions like **atherosclerosis** or trauma, which directly promotes thrombus formation. [2]
*Hypercoagulability*
- **Hypercoagulability**, or thrombophilia, refers to an increased propensity for coagulation due to genetic or acquired abnormalities in clotting factors. [1]
- This imbalance in the coagulation system is a central part of Virchow's triad, leading to an exaggerated thrombotic response even in the absence of significant stasis or injury. [2]
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Hemodynamic Disorders, Thromboembolic Disease, and Shock, pp. 132-133.
[2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. (Basic Pathology) introduces the student to key general principles of pathology, both as a medical science and as a clinical activity with a vital role in patient care. Part 2 (Disease Mechanisms) provides fundamental knowledge about the cellular and molecular processes involved in diseases, providing the rationale for their treatment. Part 3 (Systematic Pathology) deals in detail with specific diseases, with emphasis on the clinically important aspects., pp. 142-143.
More Hemodynamic Disorders Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.