Adrenal Cortical Disorders Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Adrenal Cortical Disorders. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
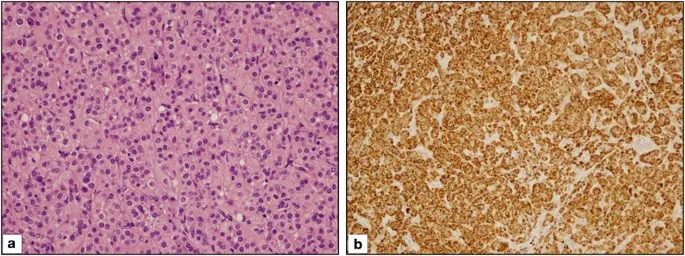
Adrenal Cortical Disorders Indian Medical PG Question 1: A patient presents with headaches, palpitations, hypertension, and urine VMA positivity. The biopsy findings are shown in the image. Which of the following statements is correct?
- A. Mostly malignant
- B. Mostly in children
- C. Mostly bilateral
- D. Associated with MEN 2A (Correct Answer)
Adrenal Cortical Disorders Explanation: ***Associated with MEN 2A***
- The clinical presentation (headaches, palpitations, hypertension) and positive **urine VMA (vanillylmandelic acid)** strongly suggest a **pheochromocytoma**.
- Pheochromocytomas are tumors of the adrenal medulla that secrete catecholamines and are frequently associated with **Multiple Endocrine Neoplasia Type 2A (MEN 2A)**, along with medullary thyroid carcinoma and primary hyperparathyroidism.
*Mostly malignant*
- Pheochromocytomas are generally benign, with approximately **10% being malignant** ("rule of 10s").
- Malignancy is difficult to predict based on histology alone and is usually defined by the presence of **metastases**.
*Mostly in children*
- While pheochromocytomas can occur at any age, they are **more common in adults**, typically between 30 and 50 years old.
- When they do occur in children, they are more often bilateral, extra-adrenal, or associated with genetic syndromes.
*Mostly bilateral*
- The majority of pheochromocytomas (approximately **90%**) are **unilateral**.
- Bilateral pheochromocytomas are often seen in genetic syndromes such as **MEN 2**, von Hippel-Lindau disease, and neurofibromatosis type 1.
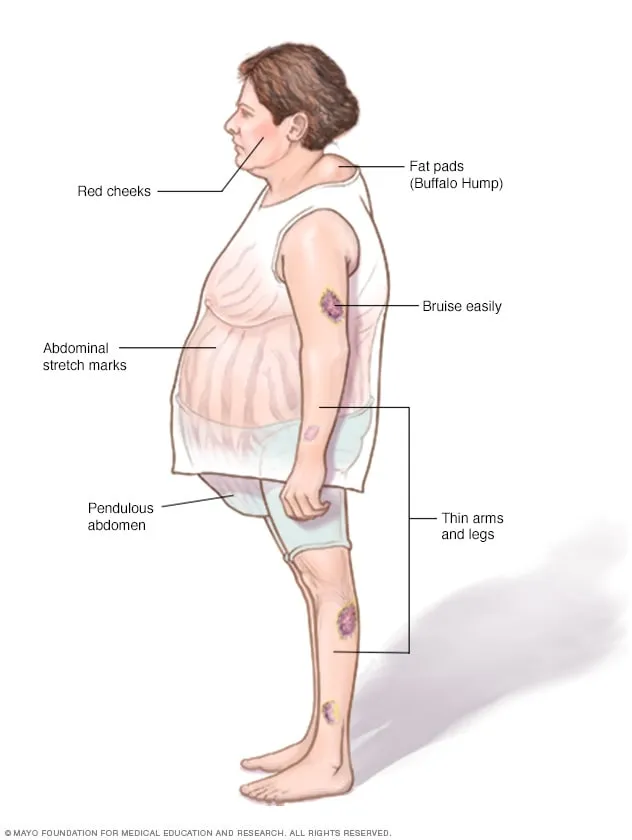
Adrenal Cortical Disorders Indian Medical PG Question 2: Which of the following best describes the hormonal profile in Cushing's disease?
- A. Decreased ACTH and decreased cortisol levels
- B. Increased ACTH and decreased cortisol levels
- C. Increased catecholamines
- D. Increased ACTH and increased cortisol levels (Correct Answer)
Adrenal Cortical Disorders Explanation: ***Increased ACTH and increased cortisol levels***
- **Cushing's disease** is caused by an **ACTH-producing pituitary adenoma** [1], leading to excessive stimulation of the adrenal glands.
- This results in **elevated ACTH** secretion, which then drives the adrenal glands to produce **excessive cortisol** [3].
*Decreased ACTH and decreased cortisol levels*
- This profile typically indicates **adrenal insufficiency**, such as **Addison's disease**, where the adrenal glands fail to produce enough cortisol, and the pituitary tries to compensate (leading to high ACTH initially) or in central adrenal insufficiency where both ACTH and cortisol are low.
- It describes a state of **cortisol deficiency**, which is the opposite of the hypercortisolism seen in Cushing's disease.
*Increased ACTH and decreased cortisol levels*
- This scenario suggests **primary adrenal insufficiency** (Addison's disease), where the adrenal glands cannot produce sufficient cortisol despite high stimulation from the pituitary gland.
- The adrenal glands are unable to respond to the elevated ACTH by producing more cortisol.
*Increased catecholamines*
- **Elevated catecholamine levels** (epinephrine and norepinephrine) are characteristic of **pheochromocytoma** [2], a tumor of the adrenal medulla.
- This condition is distinct from Cushing's disease, which involves excessive cortisol production, not catecholamines.
Adrenal Cortical Disorders Indian Medical PG Question 3: A 26-year-old male presents to the outpatient department with a discrete thyroid swelling. On neck ultrasound, an isolated cystic swelling of the gland is seen. What is the risk of malignancy associated with this finding?
- A. 48%
- B. 12%
- C. 24%
- D. 3% (Correct Answer)
Adrenal Cortical Disorders Explanation: ***3%***
- **Purely cystic thyroid nodules** (as described in this case with "isolated cystic swelling") have a **very low risk of malignancy**, typically **2-3%** or less.
- According to **ATA guidelines** and **TIRADS classification**, purely cystic nodules are considered **low suspicion** lesions.
- The cystic nature suggests a **benign process** such as a degenerated adenoma, colloid cyst, or simple cyst.
- **Fine needle aspiration (FNA)** may still be considered if the nodule is >2 cm or has any suspicious solid components, but is often not required for purely cystic lesions.
*48%*
- This percentage is **significantly higher** than the actual malignancy risk for a purely cystic thyroid swelling.
- Such a **high risk** would typically be associated with **solid nodules** exhibiting highly suspicious ultrasound features such as:
- Microcalcifications
- Irregular or spiculated margins
- Taller-than-wide shape
- Marked hypoechogenicity
- Extrathyroidal extension
*24%*
- This percentage represents a **moderate to high risk** of malignancy, which is **not characteristic** of an isolated purely cystic thyroid swelling.
- A risk in this range might be seen with:
- **Mixed solid-cystic nodules** with predominantly solid components
- Solid nodules with **intermediate suspicious features** on ultrasound
*12%*
- While lower than 24% or 48%, 12% is still **considerably higher** than the generally accepted malignancy risk for purely cystic thyroid nodules.
- This risk level could be plausible for:
- **Predominantly cystic nodules** with some eccentric solid components
- Solid nodules with **mildly suspicious** features on ultrasound
Adrenal Cortical Disorders Indian Medical PG Question 4: Most common cause of Cushing's syndrome is what?
- A. Adrenal adenoma
- B. Adrenal carcinoma
- C. McCune Albright syndrome
- D. Pituitary adenoma (Correct Answer)
Adrenal Cortical Disorders Explanation: ***Pituitary adenoma***
- The **most common cause** of Cushing's syndrome, specifically **Cushing's disease**, is excess ACTH production from a pituitary adenoma [1].
- This leads to **overstimulation of the adrenal glands**, resulting in increased cortisol production [1].
*McCune Albright syndrome*
- It is a genetic disorder characterized by **fibrous dysplasia**, **café-au-lait spots**, and **endocrine problems**, not primarily Cushing's syndrome.
- Though hormone abnormalities may present, it is not the **most common** cause of Cushing's syndrome.
*Adrenal carcinoma*
- While adrenal carcinoma can cause **Cushing's syndrome**, it is less common compared to the **pituitary adenoma** [1].
- This malignant tumor is rare and typically presents with more aggressive features and higher cortisol levels.
*Adrenal adenoma*
- Adrenal adenomas are benign tumors that can produce **excess cortisol**, but they are not the leading cause of Cushing's syndrome overall [1].
- They account for a smaller proportion of cases compared to **pituitary adenomas**.
Adrenal Cortical Disorders Indian Medical PG Question 5: In which of the following conditions would the cortisol level be highest?
- A. Normal person after receiving dexamethasone
- B. Normal person in the late evening
- C. Addison's disease
- D. Normal person in the early morning (Correct Answer)
Adrenal Cortical Disorders Explanation: ***Normal person in the early morning***
- Cortisol secretion follows a **circadian rhythm**, with levels naturally peaking in the early morning (typically between 6-8 AM) to prepare the body for the day's activities.
- This **diurnal variation** is a key physiological characteristic of cortisol, regulated by the **hypothalamic-pituitary-adrenal (HPA) axis**.
*Normal person after receiving dexamethasone*
- **Dexamethasone** is a potent synthetic glucocorticoid that **suppresses ACTH secretion** via negative feedback, leading to a significant **reduction in endogenous cortisol production**.
- This is the principle behind the **dexamethasone suppression test**, used to diagnose Cushing's syndrome (failure of suppression).
*Normal person in the late evening*
- Cortisol levels are typically at their **lowest point** in the late evening (around midnight to early morning hours) as part of the normal **circadian rhythm**.
- This nadir reflects the body's decreased need for metabolic and stress response hormones during rest.
*Addison's disease*
- **Addison's disease** is characterized by **primary adrenal insufficiency**, meaning the adrenal glands are unable to produce sufficient amounts of cortisol.
- Patients with Addison's disease have **chronically low cortisol levels** due to glandular damage, often accompanied by high ACTH levels.
Adrenal Cortical Disorders Indian Medical PG Question 6: In comparison to a normal healthy person, in the evening time, which of these will have an elevated ACTH as well as elevated Cortisol?
- A. Addison's disease
- B. Cushing's disease (Correct Answer)
- C. Transient state after exercise (evening time)
- D. Normal healthy person (evening time)
Adrenal Cortical Disorders Explanation: **_Cushing's disease_**
* In **Cushing's disease**, there is an **ACTH-producing pituitary adenoma** that leads to excessive ACTH secretion, which in turn stimulates the adrenal glands to produce high levels of cortisol.
* This results in **chronically elevated cortisol levels** throughout the day, including the evening, and an inappropriately elevated ACTH due to increased production from the pituitary.
*Addison's disease*
* **Addison's disease** is characterized by **primary adrenal insufficiency**, meaning the adrenal glands cannot produce sufficient cortisol despite adequate ACTH stimulation.
* While ACTH would be significantly **elevated** due to a lack of negative feedback from cortisol, the **cortisol levels would be low** or normal in response to the adrenal gland dysfunction.
*Transient state after exercise (evening time)*
* During and immediately after **intense exercise**, both ACTH and cortisol levels can transiently increase as part of the body's stress response.
* However, these elevations are typically **transient** and would not represent a sustained, pathologically elevated state in the evening in the same way as Cushing's disease, and levels would usually normalize relatively quickly.
*Normal healthy person (evening time)*
* In a normal healthy person, ACTH and cortisol levels exhibit a **diurnal rhythm**, with the highest levels in the morning and the lowest levels in the late evening/night.
* Therefore, in the evening, both **ACTH and cortisol levels would naturally be low** as part of the physiological circadian rhythm, not elevated.
Adrenal Cortical Disorders Indian Medical PG Question 7: Which of the following is seen in Conn's syndrome?
- A. Hypokalemia (Correct Answer)
- B. Metabolic alkalosis
- C. Hypertension
- D. Edema
Adrenal Cortical Disorders Explanation: ***Hypokalemia***
- In Conn's syndrome (primary hyperaldosteronism), excessive **aldosterone** secretion leads to increased renal reabsorption of sodium and excretion of **potassium** and hydrogen ions, resulting in hypokalemia.
- This persistent electrolyte imbalance can manifest clinically as muscle weakness, fatigue, and cardiac arrhythmias.
*Hypertension*
- While hypertension is a prominent feature of Conn's syndrome due to increased sodium reabsorption and water retention, it is a **symptom** or **consequence** of the condition, not the underlying biochemical derangement that defines the syndrome itself.
- The elevated aldosterone causes volume expansion and increased vascular tone, leading to systemic hypertension.
*Metabolic alkalosis*
- Metabolic alkalosis can occur in Conn's syndrome due to the renal excretion of **hydrogen ions** in exchange for sodium reabsorption.
- However, it is a **secondary effect** of the hyperaldosteronism and is not the primary defining biochemical abnormality like hypokalemia.
*Edema*
- Edema is generally **not a common or prominent** feature of Conn's syndrome despite the increased sodium reabsorption.
- The body's "escape phenomenon" often limits significant fluid retention and overt edema, preventing gross fluid overload.
Adrenal Cortical Disorders Indian Medical PG Question 8: Which of the following is a cause of Hirschsprung disease in a patient?
- A. Failure of involution of vitelline duct
- B. Failure of migration of neural crest cells (Correct Answer)
- C. Excessive peristalsis of the affected part of the gut
- D. Obstruction secondary to an infectious agent
Adrenal Cortical Disorders Explanation: ***Failure of migration of neural crest cells***
- Hirschsprung disease is characterized by the absence of **ganglion cells** (Auerbach and Meissner plexuses) in the distal colon [1].
- This aganglionosis results from the failure of **neural crest cells** to migrate completely from the esophagus to the anus during embryonic development [1].
*Failure of involution of vitelline duct*
- This condition is associated with **Meckel's diverticulum**, which is a remnant of the vitelline duct, not Hirschsprung disease.
- **Meckel's diverticulum** can cause symptoms like GI bleeding or obstruction, but it does not involve aganglionosis of the colon.
*Excessive peristalsis of the affected part of the gut*
- Hirschsprung disease is characterized by a **lack of peristalsis** in the aganglionic segment, leading to functional obstruction [1].
- The healthy, proximal colon may show increased peristalsis in an attempt to overcome the obstruction, but the affected segment itself is aperistaltic.
*Obstruction secondary to an infectious agent*
- Obstruction due to an infectious agent is typically related to **inflammatory processes** or strictures caused by infections (e.g., severe colitis).
- This mechanism of obstruction does not involve the **developmental anomaly** of missing ganglion cells, which is central to Hirschsprung disease.
**References:**
[1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. (Basic Pathology) introduces the student to key general principles of pathology, both as a medical science and as a clinical activity with a vital role in patient care. Part 2 (Disease Mechanisms) provides fundamental knowledge about the cellular and molecular processes involved in diseases, providing the rationale for their treatment. Part 3 (Systematic Pathology) deals in detail with specific diseases, with emphasis on the clinically important aspects., pp. 94-95.
Adrenal Cortical Disorders Indian Medical PG Question 9: Which of the following mechanisms is NOT responsible for complications in Diabetes Mellitus?
- A. Non-enzymatic glycosylation
- B. Protein Kinase C activation
- C. Disturbance in polyol pathway
- D. Chronic inflammation (Correct Answer)
Adrenal Cortical Disorders Explanation: The pathogenesis of diabetic complications is primarily driven by **hyperglycemia-induced metabolic disturbances** rather than primary chronic inflammation [1]. While diabetes is associated with a low-grade inflammatory state, the specific biochemical pathways leading to microvascular and macrovascular damage are well-defined.
### Why "Chronic Inflammation" is the Correct Answer
Chronic inflammation is a feature of many diseases, but it is **not** considered one of the four primary metabolic pathways (defined by Robbins Pathology) that directly cause diabetic complications. The damage in diabetes is biochemical and structural, resulting from the toxic effects of excess glucose on tissues that do not require insulin for glucose uptake (e.g., nerves, kidneys, blood vessels) [1].
### Explanation of Other Options (The 3 Main Mechanisms)
* **Non-enzymatic glycosylation (Option A):** Glucose binds to proteins (like collagen) without enzymes, forming **Advanced Glycation End-products (AGEs)**. AGEs cross-link proteins, trap LDL in vessel walls, and bind to RAGE (Receptors for AGEs) to release cytokines and pro-coagulant factors [1].
* **Protein Kinase C (PKC) activation (Option B):** Intracellular hyperglycemia increases Diacylglycerol (DAG), which activates PKC [1]. This leads to the production of **VEGF** (causing neovascularization in retinopathy) and **TGF-β** (causing basement membrane thickening).
* **Disturbance in Polyol Pathway (Option C):** In tissues like the lens or nerves, glucose is converted to **sorbitol** by aldose reductase. Sorbitol is osmotically active, leading to water influx, oxidative stress, and depleted glutathione, causing cataracts and peripheral neuropathy.
### NEET-PG High-Yield Pearls
* **The "Fourth" Mechanism:** Not listed here, but often tested, is the **Hexosamine pathway**, which leads to the production of fructose-6-phosphate and contributes to insulin resistance [1].
* **Common Denominator:** All these pathways are triggered by the production of **Reactive Oxygen Species (ROS)** in the mitochondria.
* **HbA1c:** This is a clinical example of non-enzymatic glycosylation used to monitor long-term glycemic control.
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1118-1121.
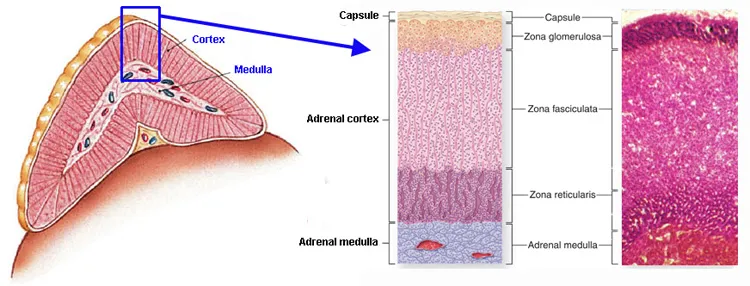
Adrenal Cortical Disorders Indian Medical PG Question 10: Pheochromocytoma are tumors of which structure?
- A. Adrenal cortex
- B. Adrenal medulla (Correct Answer)
- C. Pancreas
- D. Bone
Adrenal Cortical Disorders Explanation: **Explanation:**
**Pheochromocytoma** is a catecholamine-secreting tumor derived from the **chromaffin cells** [2] of the **adrenal medulla** [3]. These cells are embryologically derived from the **neural crest** and are responsible for synthesizing and secreting epinephrine and norepinephrine [3].
**Analysis of Options:**
* **Adrenal Cortex (Incorrect):** The cortex is derived from the mesoderm and produces steroid hormones (aldosterone, cortisol, and androgens) [3]. Tumors here include Conn’s syndrome or Cushing’s syndrome adenomas.
* **Pancreas (Incorrect):** While the pancreas has endocrine functions (Islets of Langerhans), its tumors (e.g., Insulinoma, Gastrinoma) are distinct from catecholamine-secreting pheochromocytomas.
* **Bone (Incorrect):** Bone is not a site for primary chromaffin cell tumors.
**High-Yield Clinical Pearls for NEET-PG:**
* **The Rule of 10s:** 10% are bilateral, 10% are malignant, 10% occur in children, and 10% are extra-adrenal (known as **Paragangliomas**, most commonly at the Organ of Zuckerkandl) [1].
* **Clinical Triad:** Episodic headache, sweating (diaphoresis), and palpitations/tachycardia, usually accompanied by hypertension [2].
* **Diagnosis:** Best initial screening test is **urinary/plasma metanephrines**.
* **Histology:** Characterized by the **"Zellballen" pattern** (nested clusters of cells surrounded by a vascular stroma) [1].
* **Genetic Associations:** Frequently associated with **MEN 2A and 2B**, von Hippel-Lindau (VHL) syndrome, and Neurofibromatosis type 1 (NF1).
* **Management:** Pre-operative blockade must follow the sequence: **Alpha-blockade first** (e.g., Phenoxybenzamine), followed by Beta-blockade to prevent a hypertensive crisis.
**References:**
[1] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Problems From Liver And Biliary System Disease, pp. 419-420.
[2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1137-1139.
[3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Endocrine System, pp. 1125-1126.
More Adrenal Cortical Disorders Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.