Muscular Dystrophies and Myopathies Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Muscular Dystrophies and Myopathies. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Muscular Dystrophies and Myopathies Indian Medical PG Question 1: What will be the likely cause of death in a 4-year-old boy who tires easily, exhibits weakness in the pelvic and shoulder girdles, and calf muscle enlargement, with elevated serum creatine kinase levels, and a biopsy showing marked variation in muscle fiber size and shape, muscle fiber necrosis, myophagocytosis, regenerating fibers, and fibrosis?
- A. Respiratory failure/complications (Correct Answer)
- B. Cerebrovascular complications
- C. Chronic kidney disease
- D. Pulmonary embolism
Muscular Dystrophies and Myopathies Explanation: ***Cardiomyopathy***
- In boys with **Duchenne muscular dystrophy (DMD)**, cardiomyopathy is a significant complication leading to **heart failure** and death.
- The muscle biopsy findings support **muscular dystrophy** [1], and the patient's symptoms indicate weakening of the heart muscle over time.
*End-stage renal disease*
- Typically results from **chronic kidney conditions**, which are not indicated by the case presented.
- The symptoms described, including **muscle weakness** and **fibrosis**, are not directly related to renal dysfunction.
*Cerebrovascular disease*
- Generally manifests as a sudden neurological deficit and is uncommon in **pediatric muscular conditions**.
- There is no indication of **neurological symptoms** in this patient's presentation.
*Pulmonary saddle embolism*
- This condition typically presents with sudden **shortness of breath** or **chest pain**, neither of which is mentioned here.
- The findings focus more on **muscle degeneration** rather than any acute pulmonary events.
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Peripheral Nerves and Skeletal Muscles, pp. 1244-1245.
Muscular Dystrophies and Myopathies Indian Medical PG Question 2: A 4-year-old boy is brought to the physician by his parents due to frequent falls, inability to jump, and easy fatigue. Physical examination reveals weakness in the pelvic and shoulder girdles, as well as enlargement of the child's calf muscles. The serum level of creatine kinase is elevated. A biopsy of calf muscle reveals marked variation in size and shape of muscle fibers, with foci of muscle fiber necrosis, myophagocytosis, regenerating fibers, and fibrosis. Molecular diagnostic assays performed on muscle biopsy from the patient would show alterations in the length of the primary transcript for which muscle-associated protein?
- A. Creatine kinase
- B. Desmin
- C. Dystrophin (Correct Answer)
- D. Glycogen phosphorylase
Muscular Dystrophies and Myopathies Explanation: ***Dystrophin***
- The clinical features, including muscle weakness, calf muscle hypertrophy, and elevated **creatine kinase**, indicate a muscular dystrophy, most characteristically associated with **dystrophin** deficiency [1].
- **Muscle biopsy results** showing variation in muscle fiber size and necrosis further support the diagnosis of **Duchenne muscular dystrophy**, where dystrophin mutations are commonly identified [1].
*Desmin*
- Although desmin is a muscle protein, it is primarily involved in **muscle fiber structure** and not directly associated with the symptoms or findings noted in this case.
- Conditions linked to desmin abnormalities usually involve **myofibrillar myopathies**, which present differently than the scenario described here.
*Glycogen phosphorylase*
- Glycogen phosphorylase is crucial in **glycogen metabolism**, and its deficiency typically leads to metabolic myopathies presenting with **exercise intolerance** rather than the distinct symptoms of muscle necrosis seen here.
- The muscle pathology observed (necrosis and regeneration) does not correlate with typical presentations seen in glycogen storage diseases.
*Creatine kinase*
- While creatine kinase levels are elevated in many muscle disorders, including dystrophies, it is not a structural protein and thus does not fit the question's focus on **primary transcript alterations** [2].
- Measuring creatine kinase assists in diagnosing muscle damage but does not indicate a molecular defect like **dystrophin**.
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Peripheral Nerves and Skeletal Muscles, pp. 1244-1245.
[2] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Peripheral Nerves and Skeletal Muscles, pp. 1245-1246.
Muscular Dystrophies and Myopathies Indian Medical PG Question 3: A 2-year- old boy presents with progressive clumsiness and difficulty walking. On physical examination, the child has
large calves. He has difficulty walking on his toes and has a waddling gait as shown. Which of the following is the most likely diagnosis?
- A. Myotonic dystrophy
- B. Facioscapulo humeral dystrophy
- C. Becker muscular dystrophy
- D. Duchenne muscular dystrophy (Correct Answer)
- E. Limb-girdle muscular dystrophy
Muscular Dystrophies and Myopathies Explanation: ***Duchenne muscular dystrophy***
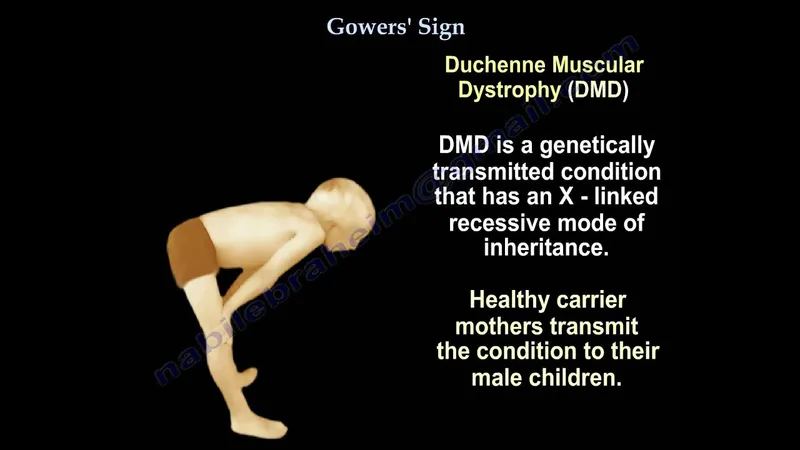
- This X-linked recessive disorder is characterized by **progressive muscle weakness** and **atrophy**, typically presenting in early childhood with symptoms like **clumsiness, difficulty walking, and a waddling gait**.
- **Pseudohypertrophy of the calves**, due to fat and connective tissue infiltration, and walking on toes are classic signs, along with a **Gowers' sign** (using hands to push off the floor to stand).
*Myotonic dystrophy*
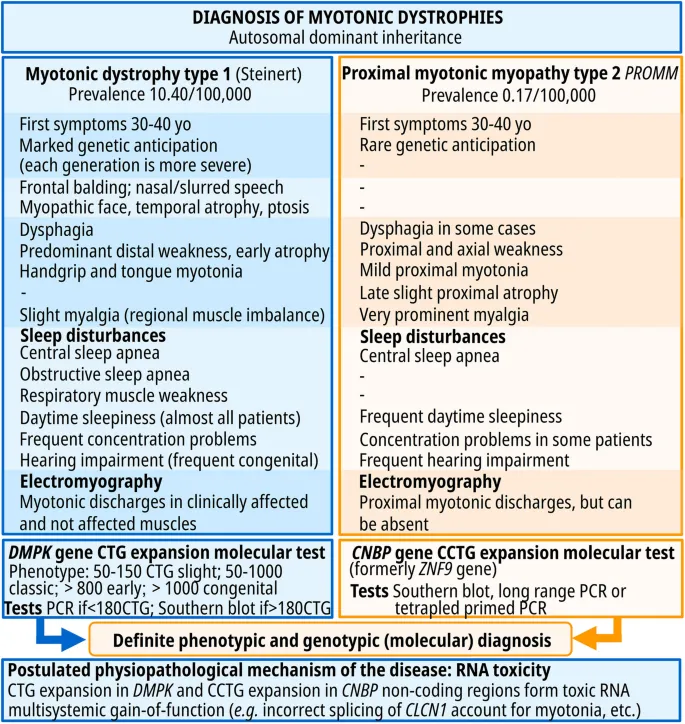
- This autosomal dominant disorder is frequently characterized by **myotonia** (delayed muscle relaxation), which is not described.
- Clinical features usually include **distal muscle weakness**, **facial weakness**, **cataracts**, and **cardiac conduction abnormalities**, and symptoms typically begin in adolescence or adulthood, though congenital forms exist with more severe weakness.
*Facioscapulohumeral dystrophy*
- This genetic disorder has a primary presentation involving weakness of the **facial muscles**, **shoulder girdle**, and **upper arm**, which is not the predominant symptom set.
- Onset is typically in adolescence or adulthood, with initial symptoms rarely affecting lower limb ambulation as severely in early childhood.
*Becker muscular dystrophy*
- While also an X-linked recessive disorder caused by a dystrophin gene mutation, **Becker muscular dystrophy** typically has a **later onset** and a **milder, slower progression** compared to Duchenne muscular dystrophy.
- Symptoms usually appear in adolescence or early adulthood, and patients often retain the ability to walk into adulthood, unlike the rapid progression seen in this 2-year-old.
*Limb-girdle muscular dystrophy*
- This heterogeneous group of disorders primarily affects **proximal muscles** of the pelvic and shoulder girdles.
- While it can present with proximal weakness, onset is typically **later in childhood or adolescence**, and **calf pseudohypertrophy** is less prominent than in Duchenne muscular dystrophy.
- The age of presentation (2 years) and classic features make Duchenne more likely.
Muscular Dystrophies and Myopathies Indian Medical PG Question 4: All are congenital myopathies except
- A. Polymyositis (Correct Answer)
- B. Central Core myopathy
- C. Centronuclear myopathy
- D. Nemaline myopathy
Muscular Dystrophies and Myopathies Explanation: ***Polymyositis***
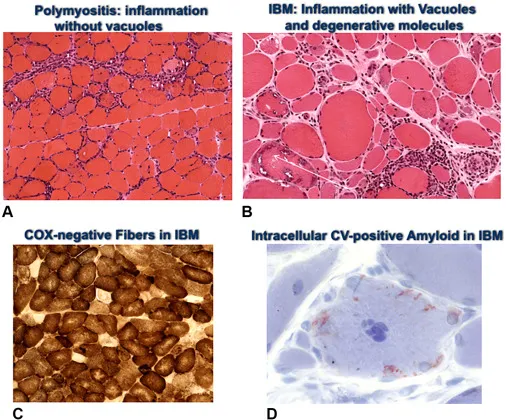
- This is an **acquired inflammatory myopathy** characterized by **autoimmune muscle inflammation** and weakness, typically presenting in adulthood [1].
- It is not a genetic or congenital condition but rather an **immune-mediated disorder** [1].
*Nemaline myopathy*
- This is a **congenital myopathy** characterized by the presence of **rod-like inclusions (nemaline bodies)** in muscle fibers.
- Symptoms often begin in infancy or childhood, including **muscle weakness** and **feeding difficulties**.
*Central Core myopathy*
- This is a **congenital myopathy** associated with mutations in the **RYR1 gene**, leading to abnormalities in muscle fibers characterized by **central cores**.
- It is often linked to **malignant hyperthermia susceptibility** and presents with early-onset **proximal muscle weakness**.
*Centronuclear myopathy*
- This is a **congenital myopathy** where muscle fibers have an **abnormal central placement of nuclei** that normally reside at the periphery.
- It typically presents at birth or in early childhood with **muscle weakness** and **hypotonia**.
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Peripheral Nerves and Skeletal Muscles, pp. 1240-1242.
Muscular Dystrophies and Myopathies Indian Medical PG Question 5: A 7 year old boy with progressive muscle weakness and walking difficulties presented with the following finding. What is the probable diagnosis?
- A. Emery-Dreifuss muscular dystrophy
- B. Duchenne muscular dystrophy (Correct Answer)
- C. Spinal muscular atrophy
- D. Myotonic dystrophy
- E. Becker muscular dystrophy
Muscular Dystrophies and Myopathies Explanation: ***Duchenne muscular dystrophy***
- The image illustrates the **Gower sign**, where the boy uses his hands to "walk up" his legs to stand from a seated position, indicating **proximal muscle weakness**, a classic feature of Duchenne muscular dystrophy (DMD).
- DMD is an X-linked recessive disorder characterized by rapid progressive muscle degeneration, typically presenting in early childhood (3-5 years) with muscle weakness, **waddling gait**, and frequent falls.
- The **age of presentation** (7 years) and **severity of weakness** requiring Gower's maneuver are most consistent with DMD rather than the milder Becker variant.
*Emery-Dreifuss muscular dystrophy*
- This dystrophy primarily affects **skeletal muscles** and the **cardiac muscle**, often presenting with joint contractures, particularly in the elbows, ankles, and neck, which are not explicitly shown or suggested as primary difficulties here.
- While it causes muscle weakness, the **pattern of weakness** and specific movements like the Gower sign are more characteristic of DMD in this age group.
*Spinal muscular atrophy*
- This condition involves the **loss of motor neurons** in the spinal cord, leading to widespread muscle weakness and atrophy, but it typically presents with **floppiness** (hypotonia) in infancy and absence of deep tendon reflexes.
- Patients with SMA would likely have significant difficulty achieving the positions seen in the Gower sign, and the muscle weakness is due to **nerve degeneration**, not directly to muscle pathology.
*Myotonic dystrophy*
- Myotonic dystrophy is characterized by **myotonia** (delayed muscle relaxation), distal muscle weakness, and often involves multiple organ systems.
- It usually presents later in childhood or adulthood with distinctive facial weakness, difficulty releasing grip, and is not typically associated with the classic presentation of **Gower sign** in a 7-year-old child.
*Becker muscular dystrophy*
- Becker muscular dystrophy is an **allelic variant** of DMD with mutations in the same dystrophin gene but producing a partially functional protein.
- It typically has a **later onset** (usually after age 10-12) and **slower progression** compared to DMD, making it less likely in a 7-year-old with significant weakness requiring Gower's maneuver.
- Patients with Becker can often maintain ambulation into their 20s or later, unlike DMD patients who typically lose ambulation by early teens.
Muscular Dystrophies and Myopathies Indian Medical PG Question 6: Muscle biopsy shows ragged red fibers on modified Gomori trichrome stain. Which enzyme defect is most likely?
- A. Complex IV
- B. Complex II
- C. Complex III
- D. Complex I (Correct Answer)
Muscular Dystrophies and Myopathies Explanation: ***Complex I***
- **Ragged red fibers** on modified Gomori trichrome stain are the pathological hallmark of **mitochondrial myopathies** [1]
- **Complex I (NADH-CoQ reductase) deficiency** is the **most common cause** of mitochondrial disease, accounting for approximately 30-40% of all cases
- Complex I deficiency is the **most frequent cause of ragged red fibers** in muscle biopsies
- Associated clinical features include progressive muscle weakness, exercise intolerance, lactic acidosis, and encephalomyopathy (Leigh syndrome) [1]
- The ragged red appearance results from subsarcolemmal accumulation of abnormal mitochondria attempting to compensate for defective oxidative phosphorylation
*Complex II*
- **Complex II (succinate dehydrogenase) deficiency** is a relatively rare cause of mitochondrial myopathy
- More commonly associated with hereditary paraganglioma-pheochromocytoma syndromes and certain cancers
- Can cause ragged red fibers but is much less common than Complex I deficiency
- The only complex entirely encoded by nuclear DNA (not mitochondrial DNA)
*Complex III*
- **Complex III (ubiquinol-cytochrome c reductase) deficiency** is a rare cause of mitochondrial disease
- Can present with myopathy and ragged red fibers, but accounts for only a small percentage of mitochondrial disorders
- Associated with exercise intolerance and multisystem involvement when present
*Complex IV*
- **Complex IV (cytochrome c oxidase, COX) deficiency** can cause mitochondrial myopathy with ragged red fibers [1]
- However, it is **less common than Complex I deficiency** as a cause of ragged red fibers
- COX-deficient fibers can be identified using specific COX histochemical staining [1]
- Associated with Leigh syndrome and other encephalomyopathies, but not the **most likely** cause when ragged red fibers are present
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Central Nervous System, pp. 1305-1306.
Muscular Dystrophies and Myopathies Indian Medical PG Question 7: Which is NOT a feature of polymyositis?
- A. Proximal muscle weakness
- B. Elevated serum creatine kinase (CK) levels
- C. Ocular muscle involvement (Correct Answer)
- D. Endomysial inflammation on muscle biopsy
Muscular Dystrophies and Myopathies Explanation: ***Ocular muscle involvement***
- **Polymyositis** primarily affects **proximal skeletal muscles**, sparing the **ocular** and facial muscles.
- Involvement of **ocular muscles** is more characteristic of other neuromuscular disorders, such as **myasthenia gravis**.
*Proximal muscle weakness*
- This is a hallmark symptom of **polymyositis**, manifesting as difficulty with activities like rising from a chair or lifting objects [1].
- The weakness is typically **symmetric** and progressive, affecting muscles of the **shoulders, hips, and neck** [1].
*Elevated serum creatine kinase (CK) levels*
- Elevated **CK levels** are a key laboratory finding in polymyositis, indicating **muscle damage** and inflammation.
- The degree of **CK elevation** often correlates with disease activity and muscle breakdown.
*Endomysial inflammation on muscle biopsy*
- A **muscle biopsy** is crucial for diagnosing polymyositis, revealing characteristic **inflammatory infiltrates** consisting mainly of **CD8+ T cells** surrounding and invading non-necrotic muscle fibers.
- This **endomysial inflammation** differentiates polymyositis from other myopathies.
Muscular Dystrophies and Myopathies Indian Medical PG Question 8: Perifascicular atrophy of muscle fibers is seen in?
- A. Myopathy due to corticosteroids
- B. Dermatomyositis (Correct Answer)
- C. Inclusion body myositis
- D. Nemaline myopathy
Muscular Dystrophies and Myopathies Explanation: ***Dermatomyositis***
- Characterized by **perifascicular atrophy** of muscle fibers, which is a distinct histological feature seen in dermatomyositis [1].
- Additionally associated with **skin manifestations** such as a heliotrope rash and Gottron's papules.
*Inclusion body myositis*
- Features **rimmed vacuoles** and **inflammatory infiltrate**, but does not show perifascicular atrophy as seen in dermatomyositis.
- Typically affects older adults and has a different clinical presentation compared to dermatomyositis.
*Nemaline myopathy*
- Characterized by **nemaline bodies** on muscle biopsy, not perifascicular atrophy, which is specific to dermatomyositis.
- Generally presents with **congenital muscle weakness**, distinctly different from the autoimmune nature of dermatomyositis.
*Steroid myopathy*
- Results from **chronic corticosteroid use**, leading to muscle weakness but does not feature perifascicular atrophy.
- Primarily affects **proximal muscles** and is linked to medication rather than a specific myopathy like dermatomyositis.
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Peripheral Nerves and Skeletal Muscles, pp. 1240-1241.
Muscular Dystrophies and Myopathies Indian Medical PG Question 9: Variation in size and shape of muscle fibers, combined with degenerative changes and intramysial fibrosis, is typical of
- A. Denervation of muscle with reinnervation
- B. Denervation atrophy
- C. Muscular dystrophy (Correct Answer)
- D. Mitochondrial myopathy
Muscular Dystrophies and Myopathies Explanation: ***Muscular dystrophy***
- The combination of **variation in muscle fiber size and shape**, **degenerative changes**, and **intramysial fibrosis** is a hallmark of muscular dystrophies [1].
- These conditions are characterized by progressive muscle weakness and degeneration, often with cycles of degeneration and attempted regeneration, leading to fibrosis [1].
*Denervation of muscle with reinnervation*
- This typically leads to **fiber type grouping** as reinnervated fibers take on the characteristics of the reinnervating nerve.
- While there may be some variation in fiber size, the prominent **degenerative changes** and **intramysial fibrosis** described are less characteristic of this process alone.
*Denervation atrophy*
- Primarily features widespread **atrophy of muscle fibers**, often angular in shape.
- It lacks the prominent combination of **fiber size variation** and **significant degenerative changes with fibrosis**.
*Mitochondrial myopathy*
- Characterized by the presence of **ragged red fibers** on Gomori trichrome stain and often **lipid accumulation** due to mitochondrial abnormalities.
- While there may be some fiber size variation, the description of widespread degenerative changes and intramysial fibrosis isn't the primary defining feature.
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Peripheral Nerves and Skeletal Muscles, pp. 1244-1245.
Muscular Dystrophies and Myopathies Indian Medical PG Question 10: A Thirty five year old female has proximal weakness of muscles, ptosis and easy fatigability. The most sensitive test to suggest the diagnosis is -
- A. CPK levels
- B. Single fiber EMG (Correct Answer)
- C. Muscle Biopsy
- D. Edrophonium test
Muscular Dystrophies and Myopathies Explanation: ***Single fiber EMG***
- This patient's symptoms (proximal muscle weakness, ptosis, and easy fatigability) are highly suggestive of **myasthenia gravis**.
- **Single fiber EMG (SFEMG)** is the **most sensitive electrophysiological test** for detecting impaired neuromuscular transmission in myasthenia gravis, even in cases with normal routine EMG [1].
*CPK levels*
- **Creatine phosphokinase (CPK)** levels are typically elevated in muscle diseases involving **muscle fiber damage**, such as inflammatory myopathies (e.g., polymyositis, dermatomyositis) or muscular dystrophies [1].
- In myasthenia gravis, CPK levels are usually **within normal limits** as it is a disorder of the neuromuscular junction, not muscle fiber integrity.
*Muscle Biopsy*
- Muscle biopsy is performed to identify **structural abnormalities** of muscle tissue, inflammation, or fiber type changes, often used in diagnosing myopathies.
- It is **not the primary diagnostic test** for myasthenia gravis, as there are no specific or consistent pathological changes evident upon muscle biopsy in this condition.
*Edrophonium test*
- The **Edrophonium (Tensilon) test** involves administering a short-acting acetylcholinesterase inhibitor, leading to a temporary improvement in muscle strength in myasthenia gravis.
- While it was historically used for diagnosis, it is **less sensitive** than SFEMG and can have false positives or negatives, thus it is not considered the **most sensitive test** overall.
More Muscular Dystrophies and Myopathies Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.