Spinal Stenosis Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Spinal Stenosis. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Spinal Stenosis Indian Medical PG Question 1: Which of the following medications is not associated with causing canalicular stenosis?
- A. Docetaxel
- B. Epinephrine
- C. Atropine (Correct Answer)
- D. 5-fluorouracil
Spinal Stenosis Explanation: ***Atropine***
- **Atropine** is an **anticholinergic drug** that primarily acts by blocking muscarinic acetylcholine receptors. It is not known to cause canalicular stenosis.
- Its effects include pupillary dilation (mydriasis), reduction of secretions, and increased heart rate, with **no direct association with lacrimal drainage system damage**.
*5-fluorouracil*
- **5-fluorouracil** (5-FU) is a chemotherapeutic agent known to cause **canalicular stenosis** as a significant ocular side effect, particularly when administered systemically or periocularly.
- The mechanism involves its cytotoxic effect on the **canalicular epithelium**, leading to inflammation and fibrosis.
*Docetaxel*
- **Docetaxel** is another chemotherapeutic agent that has been reported to cause **canalicular stenosis** and epiphora (excessive tearing).
- Its mechanism of action involves microtubule stabilization, which can lead to damage and inflammation of the **lacrimal drainage system**.
*Epinephrine*
- Topical **epinephrine** eye drops, particularly when used long-term for conditions like glaucoma, are associated with the risk of **canalicular stenosis**.
- Its metabolism can lead to the formation of **pigmentary deposits** (melanin-like) within the canaliculi, causing obstruction and inflammation.
Spinal Stenosis Indian Medical PG Question 2: A 45-year-old patient presents with chronic lower back pain. X-ray shows anterior displacement of a vertebral body. What is the likely diagnosis?
- A. Spondylosis
- B. Compression fracture
- C. Osteoporosis
- D. Spondylolisthesis (Correct Answer)
Spinal Stenosis Explanation: ***Spondylolisthesis***
- This condition involves the **anterior displacement** (slipping forward) of one vertebral body over the one below it, which perfectly matches the X-ray finding.
- It often causes **chronic lower back pain**, especially in active individuals or those with degenerative changes.
*Spondylosis*
- Refers to **degenerative changes** in the spine, including **osteophytes** and **disc space narrowing**, but typically does not involve anterior vertebral displacement.
- While it can cause chronic back pain, the specific X-ray finding points away from isolated spondylosis.
*Compression fracture*
- Involves a **collapse of the vertebral body**, usually due to trauma or osteoporosis, leading to a **decreased vertebral height**.
- It does not present as an anterior displacement of an entire vertebral body.
*Osteoporosis*
- This is a condition of **decreased bone density**, making bones fragile and prone to fractures (e.g., compression fractures), but it does not directly cause anterior vertebral displacement.
- While osteoporosis can be an underlying factor for some spinal conditions, it is not the direct diagnosis for the described X-ray finding.
Spinal Stenosis Indian Medical PG Question 3: What type of neurological signs would you expect from a lesion in the cauda equina?
- A. Normal reflexes
- B. Flaccid paralysis
- C. Muscle atrophy
- D. Lower motor neuron signs (Correct Answer)
Spinal Stenosis Explanation: ***Lower motor neuron signs***
- A lesion in the **cauda equina** affects the spinal nerve roots after they've left the spinal cord, which are part of the **peripheral nervous system**. [2]
- Therefore, it presents with classic features of **lower motor neuron (LMN) damage**, including muscle weakness, absent or reduced reflexes, and flaccid paralysis. [1]
*Normal reflexes*
- This would be an unexpected finding; **hyporeflexia or areflexia** are typical due to damage to the reflex arc within the LMN fibers. [1]
- **Normal reflexes** often suggest an intact LMN pathway, which is not the case with cauda equina compression.
*Flaccid paralysis*
- While **flaccid paralysis** is indeed a sign of lower motor neuron damage and occurs with cauda equina lesions, it is a specific symptom rather than the encompassing neurological category. [1]
- **Lower motor neuron signs** is a broader and more accurate description of the overall clinical picture.
*Muscle atrophy*
- **Muscle atrophy** is a chronic sign of lower motor neuron damage due to denervation, and while it will develop over time with a cauda equina lesion, it is usually not an initial acute finding. [1]
- The question asks for expected neurological signs, and a more immediate and overarching description is **Lower motor neuron signs**.
Spinal Stenosis Indian Medical PG Question 4: Anterolateral decompression is primarily indicated for
- A. Spinal tuberculosis (Pott's disease) (Correct Answer)
- B. Lumbar disc herniation
- C. Ankylosing spondylitis
- D. Spinal metastasis
Spinal Stenosis Explanation: ***Spinal tuberculosis (Pott's disease)***
- **Anterolateral decompression** is crucial for **Pott's disease** to remove infected bone and pus, relieve pressure on the spinal cord, and facilitate fusion.
- This approach allows direct access to the anterior spinal column, which is commonly affected by the destructive process of **tuberculosis**.
*Spinal metastasis*
- While spinal metastasis can cause compression, **anterolateral decompression** is less common as a primary approach; often, surgical treatment involves posterior decompression, stabilization, and adjuvant therapies like radiation.
- The goal is often **pain management** and neurological preservation in the context of advanced disease.
*Lumbar disc herniation*
- **Lumbar disc herniation** is typically addressed by posterior approaches like **microdiscectomy** or laminectomy, which directly access the posterior aspect of the disc.
- **Anterolateral decompression** is generally not indicated as the primary treatment for standard disc herniations.
*Ankylosing spondylitis*
- Surgical intervention in **ankylosing spondylitis** is usually reserved for severe kyphosis or spinal fractures, employing osteotomies and stabilization techniques, often through posterior approaches.
- **Anterolateral decompression** is not a standard procedure for the typical manifestations or complications of **ankylosing spondylitis**.
Spinal Stenosis Indian Medical PG Question 5: A patient complains to a physician of chronic pain and tingling of the buttocks. The pain is exacerbated when the buttocks are compressed by sitting on a toilet seat or chair for long periods. No lumbar pain is noted. Pain is elicited when the physician performs Freiberg's maneuver. Most likely diagnosis?
- A. Disk compression of the sciatic nerve
- B. Fibromyalgia
- C. Popliteus tendinitis
- D. Piriformis syndrome (Correct Answer)
Spinal Stenosis Explanation: ***Piriformis syndrome***
- The symptoms of **chronic pain and tingling in the buttocks**, exacerbated by sitting, and the positive finding on **Freiberg's maneuver** (passive internal rotation of the hip) are hallmark signs.
- This condition involves **entrapment or irritation of the sciatic nerve by the piriformis muscle**, which is located deep in the buttock.
*Disk compression of the sciatic nerve*
- While it can cause similar symptoms, the absence of **lumbar pain** makes a primary disc issue less likely.
- **Freiberg's maneuver** is specific to piriformis irritation, not typically for disk compression.
*Fibromyalgia*
- Fibromyalgia presents with **widespread musculoskeletal pain** and tenderness, not typically localized to the buttocks with specific positional exacerbation.
- It does not involve nerve entrapment or specific orthopedic maneuvers like Freiberg's maneuver.
*Popliteus tendinitis*
- Popliteus tendinitis causes pain in the **posterolateral aspect of the knee**, not the buttocks.
- It is typically associated with activities involving downhill running or pivoting of the knee.
Spinal Stenosis Indian Medical PG Question 6: Which of the following is NOT a contraindication for spinal anaesthesia?
- A. Raised intracranial tension
- B. Bleeding disorder
- C. Hypertension (Correct Answer)
- D. Infection at injection site
Spinal Stenosis Explanation: ***Hypertension***
- While **severe uncontrolled hypertension** may necessitate blood pressure stabilization before surgery, **mild to moderate hypertension** is not an absolute contraindication for spinal anesthesia.
- In fact, spinal anesthesia can sometimes be beneficial in hypertensive patients due to its **vasodilatory effects**, which may help lower blood pressure.
*Bleeding disorder*
- A **bleeding disorder** (e.g., thrombocytopenia, coagulopathy) is a **major contraindication** due to the high risk of **epidural or spinal hematoma** formation.
- A hematoma can lead to **spinal cord compression** and irreversible neurological damage.
*Raised intracranial tension*
- **Raised intracranial tension (ICT)** is a **strict contraindication** because the drop in cerebrospinal fluid (CSF) pressure during spinal anesthesia can worsen the pressure gradient across the foramen magnum.
- This can precipitate **herniation of the brainstem** and lead to catastrophic neurological injury or death.
*Infection at injection site*
- The presence of an **infection at the injection site** is an absolute contraindication as it poses a significant risk of introducing bacteria into the **subarachnoid space**.
- This can lead to serious complications such as **meningitis** or a **spinal abscess**.
Spinal Stenosis Indian Medical PG Question 7: A lesion in the cauda equina will likely present with what type of signs?
- A. Lower motor signs (Correct Answer)
- B. Spastic paralysis
- C. Hyperreflexia
- D. Upper motor signs
Spinal Stenosis Explanation: Lower motor signs
- The **cauda equina** consists of nerve roots that have **exited the spinal cord** proper, making them part of the **peripheral nervous system**. [2]
- Damage to these peripheral nerves results in **lower motor neuron deficits** such as **flaccid paralysis**, **areflexia**, and **muscle atrophy**. [1]
*Spastic paralysis*
- **Spastic paralysis** is characteristic of **upper motor neuron lesions**, not lesions affecting the peripheral nerves of the cauda equina.
- This condition involves increased muscle tone and hyperreflexia due to the disinhibition of spinal reflexes.
*Hyperreflexia*
- **Hyperreflexia** is typically a sign of an **upper motor neuron lesion**, indicating damage to the neural pathways above the level of the spinal reflex arc. [2]
- Lesions of the cauda equina, being lower motor neuron lesions, usually present with **hyporeflexia** or **areflexia**.
*Upper motor signs*
- **Upper motor neuron signs** (e.g., spasticity, hyperreflexia, positive Babinski sign) arise from damage to the motor pathways within the **brain** or **spinal cord**.
- The cauda equina, comprising nerve roots **distal to the spinal cord termination** (conus medullaris), is part of the peripheral nervous system, and its lesions produce lower motor neuron signs. [1]
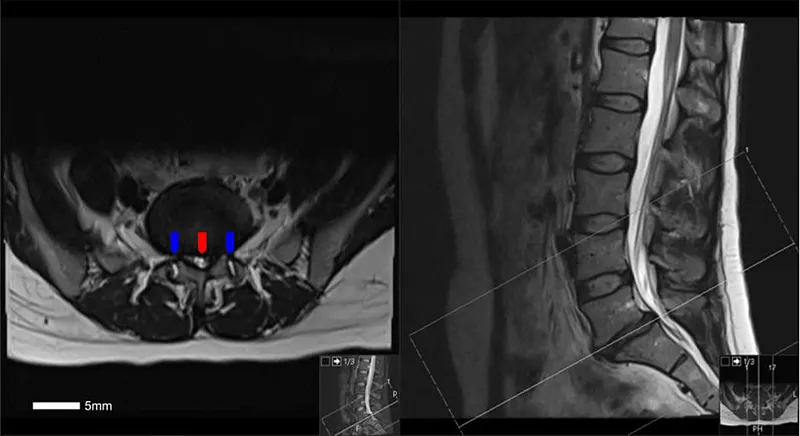
Spinal Stenosis Indian Medical PG Question 8: Investigation of choice for lumbar prolapsed disc -
- A. CT Scan
- B. Myelogram
- C. X-ray
- D. MRI (Correct Answer)
Spinal Stenosis Explanation: ***MRI***
- An **MRI** provides the best visualization of **soft tissues**, including the intervertebral discs, spinal cord, and nerve roots, making it the **gold standard** for diagnosing lumbar prolapsed disc.
- It can accurately show the **degree of disc herniation**, its impact on neural structures, and associated edema, which are crucial for treatment planning.
*CT Scan*
- While a **CT scan** provides good bony detail and can show disc herniation, its ability to visualize soft tissues is inferior to MRI for this specific condition.
- It involves **ionizing radiation** and may miss subtle nerve root compression or spinal cord abnormalities apparent on MRI.
*Myelogram*
- A **myelogram** involves injecting contrast dye into the spinal canal and then performing X-rays or CT scans to outline the spinal cord and nerve roots.
- Though effective in showing **nerve compression**, it is an **invasive procedure** with potential complications and has largely been replaced by MRI as a first-line diagnostic investigation.
*X-ray*
- **X-rays** primarily visualize **bony structures** and are useful for detecting fractures, spinal alignment issues, or severe degenerative changes.
- They **cannot directly visualize intervertebral discs** or nerve compression, making them unsuitable for diagnosing a prolapsed disc.
Spinal Stenosis Indian Medical PG Question 9: A previously healthy 45-yr-old labourer suddenly develops acute lower back pain with right-leg pain & weakness of dorsiflexion of the right great toe. Which of the following is true -
- A. Immediate treatment should include analgesics, muscle relaxants, and back strengthening exercises.
- B. If the neurological signs resolve within 2 to 3 weeks but low back pain persists, the proper treatment would include fusion of the affected lumbar vertebra.
- C. The appearance of foot drop indicates early surgical intervention. (Correct Answer)
- D. If the neurological signs fail to resolve within 1 week, lumbar laminectomy and excision of any herniated nucleus pulposus should be done.
Spinal Stenosis Explanation: ***The appearance of foot drop indicates early surgical intervention.***
- The patient presents with **acute lower back pain**, **right-leg pain**, and **weakness of dorsiflexion of the right great toe**, which strongly suggests a herniated disc compressing the **L5 nerve root**.
- **Foot drop** (inability to dorsiflex the ankle/toes) is a significant neurological deficit indicating severe nerve compression, warranting **early surgical intervention** to prevent permanent damage.
*Immediate treatment should include analgesics, muscle relaxants, and back strengthening exercises.*
- While **analgesics** and **muscle relaxants** are appropriate for initial pain management, **back strengthening exercises** are usually initiated after the acute pain subsides and often under physical therapy guidance, not immediately in the acute phase of severe neurological deficit.
- The presence of **neurological deficits** (weakness/foot drop) indicates more than just simple back pain, suggesting a need for more aggressive management beyond conservative measures alone.
*If the neurological signs resolve within 2 to 3 weeks but low back pain persists, the proper treatment would include fusion of the affected lumbar vertebra.*
- **Lumbar fusion** is a major surgical procedure typically reserved for cases of **spinal instability**, severe intractable pain unresponsive to other treatments, or significant structural deformities.
- It is **not indicated** if neurological signs resolve, even if low back pain persists, as persistent back pain post-resolution of neurological symptoms can often be managed with less invasive methods, including physical therapy, injections, or less extensive surgeries.
*If the neurological signs fail to resolve within 1 week, lumbar laminectomy and excision of any herniated nucleus pulposus should be done.*
- While persistent or worsening neurological deficits within 1-2 weeks are a strong indication for surgery, a strict 1-week timeframe for all cases of non-resolving neurological signs is **not universally applied**, especially if the symptoms are not rapidly progressing or severe.
- The decision for surgery (e.g., **laminectomy** or **microdiscectomy**) depends on the severity of neurological deficits, progression of symptoms, and failure of conservative management, but typically, an acute foot drop indicating severe compression would warrant a more urgent consideration for surgery.
Spinal Stenosis Indian Medical PG Question 10: A 60-year-old woman with a history of chronic back pain presents with acute-onset sharp pain radiating down the right leg. She also reports numbness and tingling in the foot. What is the best next step in management?
- A. Bed rest
- B. MRI of the spine (Correct Answer)
- C. X-ray of the spine
- D. Physical therapy
Spinal Stenosis Explanation: ### MRI of the spine
- The patient's symptoms of acute-onset sharp pain radiating down the right leg with numbness and tingling strongly suggest **radiculopathy**, likely due to **nerve root compression** from a herniated disc, stenosis, or other pathology [1].
- An **MRI of the spine** is the **most sensitive and specific imaging modality** to visualize soft tissue structures like intervertebral discs, nerve roots, and the spinal cord, allowing for accurate diagnosis and guiding further management.
*Bed rest*
- While historically recommended, **prolonged bed rest** is generally discouraged for acute low back pain and radiculopathy as it can lead to deconditioning and delayed recovery [2].
- **Modified activity** and early mobilization are often preferred over strict bed rest, even for severe pain [2].
*X-ray of the spine*
- An **X-ray of the spine** can identify bony abnormalities like fractures, severe degenerative changes, or spondylolisthesis, but it **cannot visualize soft tissue structures** that are typically responsible for radicular symptoms, such as herniated discs or nerve root compression.
- Therefore, it is not the best initial imaging choice for pinpointing the cause of the patient's neurological symptoms.
*Physical therapy*
- **Physical therapy** is an important component of long-term management for back pain and radiculopathy, focusing on exercises, stretching, and education to improve function and reduce pain.
- However, in the setting of **acute, severe radicular symptoms** with numbness and tingling, it is crucial to first establish a definitive diagnosis through imaging to rule out more serious compression and guide appropriate therapeutic interventions.
More Spinal Stenosis Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.