Spinal Cord Injuries Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Spinal Cord Injuries. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Spinal Cord Injuries Indian Medical PG Question 1: Anterior spinal artery is a branch of?
- A. Ascending spinal artery
- B. Vertebral artery (Correct Answer)
- C. Basilar artery
- D. Posterior spinal artery
Spinal Cord Injuries Explanation: ***Vertebral artery***
- The **anterior spinal artery** is formed by the union of two small branches, one from each **vertebral artery**, near their junction to form the basilar artery.
- It supplies the anterior two-thirds of the **spinal cord**, including the corticospinal tracts and the anterior horn.
*Ascending spinal artery*
- This is not a commonly recognized major named artery that directly gives rise to the anterior spinal artery.
- The arterial supply to the spinal cord is complex, involving main longitudinal arteries and segmental arteries.
*Basilar artery*
- The **basilar artery** is formed by the union of the two vertebral arteries and supplies the brainstem, cerebellum, and posterior cerebral hemispheres.
- While it is a continuation of the vertebral artery system, it does not directly give rise to the anterior spinal artery; rather, the vertebral arteries themselves give off the branches.
*Posterior spinal artery*
- The **posterior spinal arteries** typically arise directly from the vertebral arteries or from the posterior inferior cerebellar arteries (PICA).
- They run along the posterolateral sulci of the spinal cord and supply the posterior one-third of the cord, distinct from the anterior spinal artery's territory.
Spinal Cord Injuries Indian Medical PG Question 2: Type of sensation lost on same side of Brown Sequard syndrome?
- A. Loss of pain sensation
- B. Loss of touch sensation
- C. Loss of proprioception (Correct Answer)
- D. Loss of temperature sensation
Spinal Cord Injuries Explanation: ***Loss of proprioception***
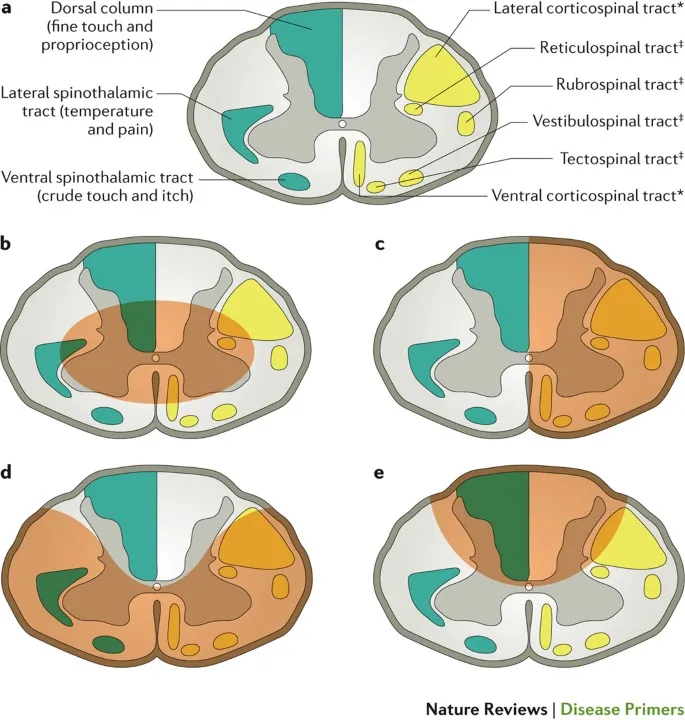
- In **Brown-Séquard syndrome**, the lesion on one side of the spinal cord interrupts the **dorsal columns** on the same side, which carry **proprioception** and vibration sense [1].
- This results in the loss of **fine touch and proprioception** ipsilateral to the lesion [1].
*Loss of pain sensation*
- **Pain and temperature sensations** are carried by the **spinothalamic tracts**, which cross in the spinal cord one or two levels above their entry [1].
- Therefore, a lesion in **Brown-Séquard syndrome** typically causes a loss of pain and temperature sensation **contralateral** to the lesion, starting a few segments below the injury [1].
*Loss of touch sensation*
- **Crude touch** (non-discriminative touch) is carried by the spinothalamic tract, crossing to the contralateral side.
- **Fine touch** (discriminative touch) is carried by the dorsal columns, which ascend ipsilaterally and cross in the medulla, leading to ipsilateral loss of fine touch in Brown-Séquard syndrome [1]. This option is too general, as fine touch is lost but crude touch involves a different pathway.
*Loss of temperature sensation*
- Similar to pain sensation, **temperature sensation** is carried by the **spinothalamic tracts** and crosses over in the spinal cord [1].
- This leads to a loss of temperature sensation **contralateral** to the lesion below the level of injury in **Brown-Séquard syndrome** [1].
Spinal Cord Injuries Indian Medical PG Question 3: Hypotension in acute spinal injury is due to:
- A. Loss of sympathetic tone (Correct Answer)
- B. Loss of parasympathetic tone
- C. Orthostatic hypotension
- D. Vasovagal attack
Spinal Cord Injuries Explanation: ***Loss of sympathetic tone***
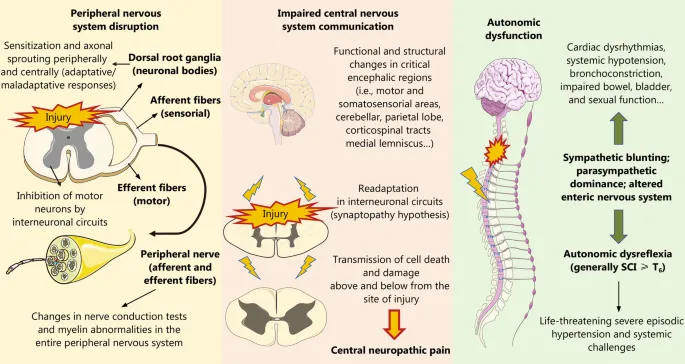
- **Acute spinal cord injury** above T6 can interrupt the sympathetic outflow from the central nervous system.
- This leads to unopposed **parasympathetic activity**, causing **vasodilation**, **bradycardia**, and resultant **hypotension**.
*Loss of parasympathetic tone*
- Loss of parasympathetic tone would typically result in **tachycardia** and potentially **hypertension**, as sympathetic activity would be unopposed.
- This is not the primary mechanism for hypotension observed in acute spinal injury.
*Orthostatic hypotension*
- While patients with spinal cord injury can experience orthostatic hypotension, the initial acute hypotension is due to the fundamental physiological disruption of **autonomic control**.
- **Orthostatic hypotension** specifically refers to a drop in blood pressure upon standing, which is a symptom that can persist, but not the direct cause of acute neurogenic shock.
*Vasovagal attack*
- A **vasovagal attack** is typically triggered by emotional stress or pain, leading to temporary reflex-mediated bradycardia and vasodilation.
- It is not the underlying cause of sustained hypotension in the setting of acute spinal cord injury.
Spinal Cord Injuries Indian Medical PG Question 4: All of the following are complications of epidural anaesthesia, EXCEPT:
- A. Urinary retention
- B. Total spinal analgesia
- C. Hypopnoea
- D. Hypertension (Correct Answer)
Spinal Cord Injuries Explanation: ***Hypertension***
- Epidural anesthesia commonly causes **vasodilation** and a subsequent drop in **blood pressure** (hypotension), not hypertension, due to sympathetic blockade.
- While hypertension can occur due to pain or anxiety during the procedure, it is not a direct physiological complication of the epidural anesthetic itself.
*Urinary retention*
- Epidural anesthesia can affect the nerves controlling the **bladder**, leading to temporary **urinary retention**.
- This is a common complication, often requiring catheterization until the epidural wears off.
*Total spinal analgesia*
- This occurs if the epidural needle inadvertently punctures the **dura** and a large dose of local anesthetic is injected into the **subarachnoid space**.
- It results in widespread **sensory and motor blockade**, potentially leading to respiratory arrest and hemodynamic collapse.
*Hypopnoea*
- High epidural blocks or accidental **intrathecal administration** can cause paralysis of **intercostal muscles** and the diaphragm.
- This can lead to **respiratory depression** (hypopnoea) or even apnea, necessitating ventilatory support.
Spinal Cord Injuries Indian Medical PG Question 5: Vasopressor of choice in hypotension produced during subarachnoid block is
- A. Ephedrine (Correct Answer)
- B. Mephentermine
- C. Epinephrine
- D. Dobutamine
Spinal Cord Injuries Explanation: ***Ephedrine***
- **Ephedrine** is a sympathomimetic with both direct (on adrenergic receptors) and indirect (releasing norepinephrine) effects, causing vasoconstriction and increased heart rate, making it suitable for treating **hypotension** during **subarachnoid block**.
- Its slower onset and longer duration of action compared to direct-acting vasopressors can be beneficial for sustained pressure support in this context.
*Mephentermine*
- While mephentermine is also an indirect-acting sympathomimetic used for hypotension, it has a **slower onset** and a more prolonged effect compared to ephedrine.
- Ephedrine is generally preferred due to its faster action in acute settings like **subarachnoid block-induced hypotension**, where rapid correction is often required.
*Epinephrine*
- **Epinephrine** is a potent vasopressor with significant alpha and beta-adrenergic effects, leading to strong vasoconstriction and cardiac stimulation.
- Its use might lead to **tachycardia** and arrhythmias, which are generally undesirable when milder agents like ephedrine can achieve the desired effect.
*Dobutamine*
- **Dobutamine** is primarily a beta-1 adrenergic agonist, meaning it mainly increases cardiac contractility and heart rate with minimal effect on systemic vascular resistance.
- It is not the agent of choice for hypotension due to **vasodilation** from subarachnoid block, as it does not sufficiently address the primary problem of decreased vascular tone.
Spinal Cord Injuries Indian Medical PG Question 6: A 25-year-old man is brought to the emergency department after sustaining a stab wound to the lower back. Examination shows right leg weakness in all muscle groups and loss of vibration and proprioception on the same side. There is loss of pain and temperature sensation but preserved motor strength in the left leg. He has no problems with bladder or bowel retention. Motor strength is preserved in the upper extremities.
His presentation is most consistent with which one of the following spinal cord syndromes?
- A. Anterior cord syndrome
- B. Cauda equina syndrome
- C. Central cord syndrome
- D. Hemisection of the cord (Correct Answer)
Spinal Cord Injuries Explanation: ***Hemisection of the cord***
- This syndrome, also known as **Brown-Séquard syndrome**, is characterized by ipsilateral motor paralysis and loss of proprioception/vibration below the lesion, and contralateral loss of pain and temperature sensation [1]. The patient's presentation perfectly matches these findings.
- The **stab wound** to the lower back suggests a highly localized injury, which is consistent with a hemisection rather than a more diffuse cord injury.
*Anterior cord syndrome*
- This syndrome typically results in **bilateral motor paralysis** below the lesion and bilateral loss of pain and temperature sensation.
- **Proprioception and vibration sensation are preserved** in anterior cord syndrome because the posterior columns are spared [1].
*Cauda equina syndrome*
- This syndrome involves injury to the **nerve roots below the spinal cord** and typically presents with bilateral leg weakness, **saddle anesthesia**, and bladder/bowel dysfunction.
- The patient in this case has unilateral motor and sensory deficits and no bladder/bowel issues, which is inconsistent with cauda equina syndrome.
*Central cord syndrome*
- This syndrome usually results in **greater motor weakness in the upper extremities** than in the lower extremities, along with a variable sensory loss [1].
- It often occurs after hyperextension injuries in older individuals with cervical spondylosis, and the patient's presentation of a stab wound and specific unilateral deficits does not fit this pattern.
Spinal Cord Injuries Indian Medical PG Question 7: A 50-year-old male with a history of chronic low back pain presents with new-onset bowel and bladder incontinence. What is the next best step in management?
- A. Conservative management with NSAIDs
- B. Bed rest
- C. Urgent MRI of the spine (Correct Answer)
- D. Physical therapy
Spinal Cord Injuries Explanation: ***Urgent MRI of the spine***
- The new onset of **bowel and bladder incontinence** in a patient with chronic low back pain is highly suggestive of **cauda equina syndrome**. This is a surgical emergency.
- An **urgent MRI** is crucial to confirm the diagnosis and identify the level of compression, guiding immediate surgical decompression to prevent permanent neurological deficits.
*Conservative management with NSAIDs*
- This approach is appropriate for routine, uncomplicated low back pain, but it is entirely inadequate for a **neurological emergency** like potential cauda equina syndrome.
- Delaying definitive diagnosis and treatment in such cases can lead to irreversible neurological damage, including chronic incontinence and paralysis.
*Bed rest*
- While bed rest might be recommended for acute exacerbations of certain types of back pain, it is not a primary treatment for neurologic emergencies and will not resolve the underlying compression causing **cauda equina syndrome**.
- Prolonged bed rest can also lead to complications like deconditioning and venous thromboembolism, and it would waste critical time for diagnosis and intervention.
*Physical therapy*
- Physical therapy is a cornerstone of management for chronic low back pain and for rehabilitation after an acute event once stability is achieved.
- However, in cases of suspected **cauda equina syndrome**, physical therapy is contraindicated as an initial step because it does not address the acute spinal cord or nerve root compression and may worsen the condition or delay necessary surgical intervention.
Spinal Cord Injuries Indian Medical PG Question 8: What is the most common movement force involved in fractures of the spine?
- A. Extension
- B. Flexion
- C. Lateral Rotation
- D. Compression (Correct Answer)
Spinal Cord Injuries Explanation: ***Compression***
- **Axial compression** due to falls from a height or direct impact is the most frequent mechanism leading to vertebral body fractures, such as **compression fractures**.
- These forces typically crush the vertebral body, often without significant displacement of bone fragments.
*Flexion*
- While often present in spinal fractures, pure **flexion forces** alone are less common than compression as the primary force.
- Flexion forces are most frequently involved in **wedge fractures** and **flexion-distraction injuries**, where they are often combined with compression or distraction.
*Extension*
- **Extension injuries** are relatively rare and usually occur in specific scenarios like being struck in the chin or in elderly patients with **ankylosing spondylitis**.
- These forces can lead to fractures of the posterior elements or **hyperextension injuries** of the anterior spinal column.
*Lateral Rotation*
- **Rotational forces**, especially when combined with flexion or extension, can cause unstable fracture patterns like **fracture-dislocations**.
- However, isolated **lateral rotation** as the primary injury mechanism is much less common than axial compression.
Spinal Cord Injuries Indian Medical PG Question 9: In typical hanging, knot is placed at:
- A. Chin
- B. Right side of mandible
- C. Occiput (Correct Answer)
- D. Left side of mandible
Spinal Cord Injuries Explanation: ***Occiput***
- In **typical hanging** (complete suspension of the body), the knot is usually placed at the **occipital region** (nape of the neck/back of the head).
- This positioning results in an **oblique ligature mark** that is higher posteriorly and **typical of suicidal hanging**.
- Death occurs primarily due to **compression of neck vessels** (carotid arteries and jugular veins), leading to **cerebral anoxia**, and **vagal nerve stimulation** causing cardiac arrest.
- The **occiput position** distinguishes typical hanging from atypical variants.
*Chin*
- If the knot is placed at the chin (anterior position), this is **not characteristic of typical hanging**.
- This position would cause primarily **airway compression** but is uncommon in practice.
- Anterior positioning is rarely seen in complete suspension cases.
*Right side of mandible*
- Placing the knot on the **lateral side** of the mandible (right or left) is characteristic of **atypical hanging**.
- This results in an **oblique ligature mark** higher on the side of the knot.
- In atypical hanging, the body may be **partially suspended** or in various positions (sitting, kneeling, lying).
- Death occurs through similar mechanisms but may be slower due to incomplete vascular compression.
*Left side of mandible*
- Similar to placement on the right side, a knot on the left side of the mandible indicates **atypical hanging**.
- The **lateral position** of the knot (either side) is the key distinguishing feature from typical hanging where the knot is posterior.
- Atypical hanging is still fatal through neck vessel compression and vagal stimulation, though the presentation differs from typical cases.
Spinal Cord Injuries Indian Medical PG Question 10: A 40-year-old male sustains spinal injury after an accident. His lower limb power is greater than that of upper limb and sacral sensations are present. Type of spinal cord lesion is:
- A. Complete spinal cord injury.
- B. Central cord syndrome (Correct Answer)
- C. Posterior cord syndrome
- D. Anterior cord syndrome
Spinal Cord Injuries Explanation: ***Central cord syndrome***
- This syndrome is characterized by **greater motor weakness** in the **upper extremities** than in the lower extremities, along with varying degrees of sensory loss. **Sacral sparing** (preserved perineal sensation and voluntary anal contraction) is also a classic feature.
- It often results from **hyperextension injuries** of the cervical spine, leading to damage predominantly in the central gray matter and surrounding white matter.
*Complete spinal cord injury*
- This involves a total loss of **motor and sensory function** below the level of the injury, including the sacral segments.
- The presence of **sacral sensations** in the patient rules out a complete spinal cord injury.
*Posterior cord syndrome*
- This syndrome affects the **dorsal columns**, resulting in a loss of **proprioception**, **vibration sense**, and **fine touch** below the level of injury.
- Motor function and pain/temperature sensation are typically preserved, which does not match the described motor weakness.
*Anterior cord syndrome*
- This involves damage to the **anterior two-thirds of the spinal cord**, leading to a loss of **motor function** (corticospinal tracts) and **pain and temperature sensation** (spinothalamic tracts) below the injury.
- However, **proprioception** and **vibration sense** (dorsal columns) are typically preserved, and sacral sparing of sensation is not a characteristic feature, nor is greater lower limb power. [1]
More Spinal Cord Injuries Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.