Plate Osteosynthesis Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Plate Osteosynthesis. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Plate Osteosynthesis Indian Medical PG Question 1: Nonunion is most common in fracture of the:
- A. Talus
- B. Neck femur (Correct Answer)
- C. Scapula
- D. None of the options
Plate Osteosynthesis Explanation: ***Neck femur***
- Fractures of the **femoral neck** are highly prone to **nonunion** due to the precarious and often-disrupted blood supply to the femoral head, particularly the **retinacular arteries**.
- The high biomechanical stress and difficulty in achieving stable fixation in this region further contribute to the increased risk of nonunion.
*Talus*
- While talar fractures, especially those of the **talar neck**, can have a high incidence of complications like **avascular necrosis** due to limited blood supply, nonunion is less common than in femoral neck fractures.
- The talus has a complex vascular network that, while vulnerable, often allows for healing.
*Scapula*
- **Scapular fractures** are generally uncommon and, when they occur, typically heal well without surgical intervention.
- Due to the surrounding musculature and rich vascular supply, nonunion of the scapula is extremely rare.
*None of the options*
- This option is incorrect because **nonunion is indeed a significant problem** in specific fractures, particularly those of the femoral neck, making it a viable answer.
Plate Osteosynthesis Indian Medical PG Question 2: Open reduction (OR) is not required in which fracture?
- A. Fracture of the patella
- B. Fracture of the outer one-third of the radius (Correct Answer)
- C. Displaced fracture of the olecranon
- D. Fracture of the condyle of the humerus
Plate Osteosynthesis Explanation: ***Fracture of the outer one-third of the radius***
- Fractures of the **outer one-third of the radius** (distal radius fractures) often can be managed with **closed reduction and casting** if stable and adequately reduced.
- While some unstable distal radius fractures require OR, many stable patterns, especially those with minimal displacement or good alignment after closed manipulation, do not.
*Fracture of the patella*
- Many patellar fractures lead to significant **extensor mechanism disruption**, necessitating OR with **tension band wiring** or screw fixation to restore quadriceps function.
- Displaced patellar fractures, especially transverse ones, require surgical fixation to prevent extensor lag and **nonunion**.
*Displaced fracture of the olecranon*
- Displaced olecranon fractures disrupt the **triceps mechanism** and compromise elbow stability, almost always requiring **open reduction and internal fixation (ORIF)**, typically with tension band wiring.
- Without surgical repair, a displaced olecranon fracture can lead to significant loss of extension strength and **nonunion**.
*Fracture of the condyle of the humerus*
- Fractures of the humeral condyle, particularly in children, often require OR due to the risk of **avascular necrosis** (especially lateral condyle) and the need for **precise anatomical reduction** to prevent joint incongruity and cubitus varus/valgus deformities.
- Intra-articular and displaced condylar fractures almost invariably require surgical intervention to ensure harmonious joint function and prevent long-term complications like **stiffness and deformity**.
Plate Osteosynthesis Indian Medical PG Question 3: Which of the following is a contraindication for open reduction & internal fixation (ORIF)?
- A. Active infection
- B. Soft bones
- C. Soft tissue contractures around the fracture site
- D. All of the options (Correct Answer)
Plate Osteosynthesis Explanation: ***All of the options***
- **Active infection** at the surgical site is a significant contraindication for ORIF due to the high risk of **osteomyelitis** and implant failure.
- **Soft bones**, such as those found in patients with **osteoporosis**, may not adequately hold the internal fixation devices (screws, plates), leading to implant loosening or cutout.
- **Soft tissue contractures** around the fracture site can make surgical access difficult, compromise soft tissue coverage, and increase the risk of wound complications and poor functional outcomes.
*Active infection*
- While a direct contraindication, it's not the *only* one for ORIF.
- Performing ORIF in the presence of infection significantly increases the risk of **surgical site infection** and implant failure, potentially leading to chronic osteomyelitis.
*Soft bones*
- This is a significant challenge for ORIF, as the bone quality may not be sufficient to hold the hardware securely.
- It increases the risk of **implant failure** and non-union, but again, it's not the sole contraindication listed.
*Soft tissue contractures around the fracture site*
- Severe contractures can **impede surgical exposure**, make anatomical reduction difficult, and compromise the vascularity of the tissues.
- This can lead to increased rates of **wound complications** and poor healing, but it is one of several contraindications.
Plate Osteosynthesis Indian Medical PG Question 4: First-line treatment for non-displaced scaphoid fracture
- A. Compression Plating
- B. Compression Screws
- C. Conservative (Correct Answer)
- D. Traction
Plate Osteosynthesis Explanation: ***Conservative***
- Non-displaced scaphoid fractures are typically managed conservatively with **cast immobilization** due to the bone's precarious blood supply.
- This approach aims for sufficient **healing without operative risks**, with a long casting period (often 6-12 weeks) to ensure union.
*Compression Plating*
- **Compression plating** is generally reserved for **complex or displaced scaphoid fractures** that require more robust fixation.
- It is an **invasive surgical option** that carries risks beyond what is typically necessary for a non-displaced fracture.
*Compression Screws*
- **Compression screws** (e.g., Herbert screw) are used for **surgical fixation** of scaphoid fractures, particularly displaced or unstable types.
- This method is more invasive than conservative management and involves risks like **avascular necrosis** or **non-union** if not properly performed.
*Traction*
- **Traction** is rarely used as a primary treatment for scaphoid fractures; its application is more common in **dislocations** or **certain complex fractures** to maintain alignment.
- Applying traction to a scaphoid fracture could potentially exacerbate instability rather than promote union.
Plate Osteosynthesis Indian Medical PG Question 5: Minimally invasive Percutaneous plate osteosynthesis (MIPPO technique) is of use in:
- A. Fracture with metaphyseal comminution (Correct Answer)
- B. Segmental fracture
- C. Spiral fracture
- D. Oblique fracture
Plate Osteosynthesis Explanation: ***Fracture with metaphyseal comminution***
- The **MIPPO technique** is particularly useful for achieving stability in fractures with **metaphyseal comminution** by bridging the comminuted zone with a plate applied percutaneously.
- This approach minimizes soft tissue dissection, preserving **periosteal blood supply**, which is crucial for healing in these complex fractures.
*Segmental fracture*
- While MIPPO can be used, **segmental fractures** often require more direct reduction and stabilization of both fracture segments, which might be challenging with a purely percutaneous approach alone.
- The primary concern in segmental fractures is often maintaining length and alignment across two distinct fracture lines.
*Spiral fracture*
- **Spiral fractures** are typically inherently stable after reduction and are often amenable to intramedullary nailing or less invasive plate fixation, as the fracture pattern allows for good interfragmentary compression.
- The main advantage of MIPPO (minimizing soft tissue stripping around comminution) is less critical in these stable, non-comminuted patterns.
*Oblique fracture*
- Similar to spiral fractures, **oblique fractures** are often amenable to primary screw fixation or conventional plating techniques due to their stable nature after reduction and good contact between fracture fragments.
- The specific advantages of MIPPO for comminuted fractures are less relevant for simple oblique patterns.
Plate Osteosynthesis Indian Medical PG Question 6: In hand injury, the first structure to be repaired should be?
- A. Skin
- B. Muscle
- C. Nerve
- D. Bone (Correct Answer)
Plate Osteosynthesis Explanation: ***Bone***
- In hand injury, **skeletal stability** is paramount and is typically the first structure to be addressed to provide a stable foundation.
- Repairing bone first allows for proper alignment and length restoration, which is crucial for the subsequent repair of soft tissues like tendons, nerves, and vessels.
*Skin*
- While skin closure is the final step in wound management, it should only be performed after deeper structures like bone, tendons, and nerves have been repaired.
- Repairing the skin first would prevent access to underlying damaged structures and could lead to functional impairment.
*Muscle*
- Muscle repair is important for restoring function but should follow bone stabilization to ensure proper length and tension.
- Unstable bone fragments can impede effective muscle repair and healing.
*Nerve*
- Nerve repair is critical for restoring sensation and motor function and should be done with meticulous attention to detail.
- However, nerve repair typically follows bone stabilization and sometimes tendon repair, as a stable environment is necessary for successful nerve coaptation and healing.
Plate Osteosynthesis Indian Medical PG Question 7: Which of the following is the appropriate treatment for atrophic non-union?
- A. External fixation
- B. Application of cast
- C. Stabilization and bone grafting (Correct Answer)
- D. Internal fixation
Plate Osteosynthesis Explanation: ***Stabilization and bone grafting***
- Atrophic non-union is characterized by a **lack of biological activity** and an **absence of callus formation**, requiring both **biological stimulation** (bone graft) and **mechanical stability** (stabilization).
- Bone grafting provides **osteogenic cells**, **osteoconductive scaffold**, and **osteoinductive growth factors** to promote healing, while stabilization ensures the fracture fragments remain in apposition.
*External fixation*
- While providing stability, external fixation alone does not address the **biological deficiency** inherent in atrophic non-union.
- It's mainly used for **open fractures**, **comminuted fractures**, or when internal fixation is not feasible, often as a temporary measure.
*Application of cast*
- A cast provides some immobilization but is generally insufficient for non-union, especially atrophic types, due to its **limited stability** and inability to compress the fracture site effectively.
- It also does not contribute to the **biological stimulation** needed for healing in atrophic non-unions.
*Internal fixation*
- Internal fixation provides stability, but in atrophic non-union, the primary issue is a **lack of healing potential**, not just instability.
- Without a concomitant **bone graft**, internal fixation alone is unlikely to achieve union in atrophic non-unions.
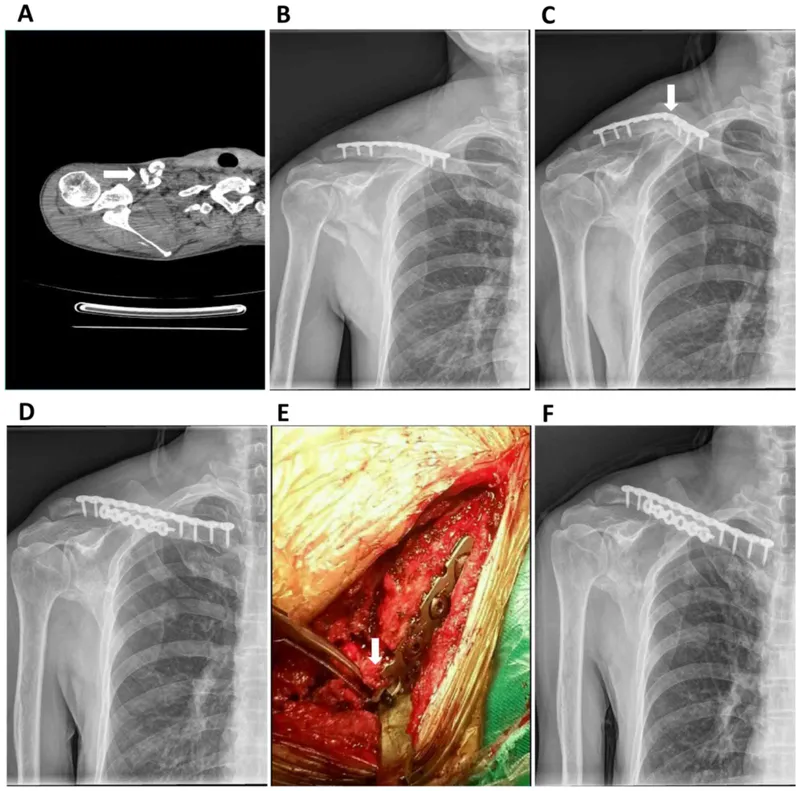
Plate Osteosynthesis Indian Medical PG Question 8: The X-ray shows plating done for a fracture. How does this fracture heal?
- A. Primary healing (Correct Answer)
- B. Secondary healing
- C. Tertiary healing
- D. Distraction histiogenesis
Plate Osteosynthesis Explanation: **Primary healing**
- **Plating of a fracture** aims to achieve **absolute stability** at the fracture site, which facilitates primary bone healing.
- In primary healing, there is **direct bone formation** across the fracture gap without the formation of a significant callus.
*Secondary healing*
- Secondary healing involves the formation of a **callus** (fibrous tissue, cartilage, and immature bone) to bridge the fracture gap.
- This type of healing occurs in situations with **relative stability** and some micromotion at the fracture site, such as with casting or intramedullary nailing.
*Tertiary healing*
- **Tertiary healing** is not a recognized term in the context of fracture healing.
- Bone healing typically involves either primary or secondary mechanisms depending on the stability achieved.
*Distraction histiogenesis*
- **Distraction histiogenesis** is the process by which new bone is formed between bone surfaces that are gradually pulled apart using an external fixator (**distraction osteogenesis**).
- This is used in procedures like **limb lengthening** and is distinct from the direct healing of a fracture fixed with a plate.
Plate Osteosynthesis Indian Medical PG Question 9: Identify the implant shown in the image:
- A. Dynamic hip screw (Correct Answer)
- B. Cannulated hip screw
- C. Condylar hip screw
- D. Intramedullary nail
Plate Osteosynthesis Explanation: ***Dynamic hip screw***
- The image shows a **lag screw** inserted into the femoral neck and head, which slides within a **side plate** attached to the femoral shaft with cortical screws.
- This construct allows for controlled **dynamic collapse** and impaction at the fracture site, promoting healing and providing stable fixation for **extracapsular hip fractures**.
*Cannulated hip screw*
- Cannulated screws are typically used in a **parallel configuration** or as a single large screw for hip fractures, particularly **femoral neck fractures**.
- They do not feature a **side plate** that extends down the femoral shaft for additional fixation.
*Condylar hip screw*
- A condylar hip screw (DCS) is used for **distal femur fractures**, often extending into the **condyles**.
- It involves a different angulation and design compared to the proximal femoral implant seen, which is fixed to the femoral shaft.
*Intramedullary nail*
- An intramedullary nail is inserted into the **medullary canal** of the bone, running through its center.
- While some hip nails (e.g., trochanteric nails) have a cephalic screw component, they primarily stabilize the shaft from within, unlike the **extracortical side plate** seen here.
Plate Osteosynthesis Indian Medical PG Question 10: Locking compression plating is commonly indicated in which of the following fracture types?
- A. Periaicular fractures
- B. Transverse or oblique fractures of long bones (Correct Answer)
- C. Interochanteric fractures
- D. Fracture of long bones
Plate Osteosynthesis Explanation: ***Transverse or oblique fractures of long bones***
- **Locking compression plates (LCPs)** are particularly well-suited for **transverse or oblique fractures of long bones** because they provide angular stability, preventing screw pullout even in compromised bone.
- Their design allows for a **fixed-angle construct**, which helps maintain alignment and promotes biological healing by minimizing periosteal stripping.
*Periaicular fractures*
- While LCPs can be used in some **periarticular fractures**, their primary indication is not specifically these fractures, and their benefit is often related to the bone quality of the metaphysis rather than the articulation itself.
- These fractures often require careful contouring of plates to conform to the complex anatomy, and sometimes require different fixation strategies.
*Interochanteric fractures*
- **Intertrochanteric fractures** of the femur are typically treated with intramedullary nails (e.g., trochanteric entry nails) or dynamic hip screws, which are better suited for load-sharing in this weight-bearing region.
- Plates, especially LCPs, are generally not the first-line treatment for these fractures due to the high biomechanical forces and risk of cutout.
*Fracture of long bones*
- This option is too general; while LCPs are used for some **long bone fractures**, it is not indicated for all types. Many long bone fractures are better treated with intramedullary nailing or traditional non-locked plating.
- The specific fracture pattern (e.g., comminuted, transverse, oblique) and location within the long bone determine the most appropriate fixation method.
More Plate Osteosynthesis Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.