Ischemic Optic Neuropathies Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Ischemic Optic Neuropathies. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Ischemic Optic Neuropathies Indian Medical PG Question 1: A case of injury to right brow due to a fall from scooter presents with sudden loss of vision in the right eye. The pupil shows absent direct reflex but a normal consensual pupillary reflex is present. The fundus is normal. The treatment of choice is:
- A. Pulse methyl Prednisolone 250 mg four times daily for three days
- B. Emergency optic canal decompression
- C. Oral Prednisolone 1.5 mg/kg body weight
- D. Intensive intravenous corticosteroids as prescribed for spinal injuries to be instituted within six hours (Correct Answer)
Ischemic Optic Neuropathies Explanation: ***Intensive intravenous corticosteroids as prescribed for spinal injuries to be instituted within six hours***
- The sudden **loss of vision** with a **traumatic brow injury** and **afferent pupillary defect** (absent direct reflex, normal consensual) suggests **traumatic optic neuropathy (TON)**.
- While the efficacy of corticosteroids is debated, high-dose intravenous corticosteroids, often following the **National Acute Spinal Cord Injury Study (NASCIS)** protocols (similar to spinal injury treatment), are a common initial treatment for TON, especially when administered within 6-8 hours of injury to reduce inflammation and edema around the optic nerve.
*Pulse methyl Prednisolone 250 mg four times daily for three days*
- This dosage regimen is a form of **pulse steroid therapy**, but the specific dose and frequency may not align with the standard high-dose IV corticosteroid protocols used for TON (e.g., typically 1g methylprednisolone daily).
- While corticosteroids are used, the precise protocol and optimal dosing for TON are critical and vary from this option.
*Emergency optic canal decompression*
- **Optic canal decompression surgery** is considered in cases of TON where there is direct compression of the optic nerve or a lack of response to corticosteroid therapy.
- It is not the initial treatment of choice for all TON cases and carries significant surgical risks; corticosteroid therapy is usually attempted first.
*Oral Prednisolone 1.5 mg/kg body weight*
- **Oral corticosteroids** are generally not sufficient for the acute, severe inflammation seen in traumatic optic neuropathy.
- **Intravenous administration** is preferred for its rapid and higher systemic bioavailability to achieve therapeutic levels at the optic nerve.
Ischemic Optic Neuropathies Indian Medical PG Question 2: Jaw tightness is typically seen in:
- A. Coarctation of aorta
- B. Giant cell arteritis (GCA) (Correct Answer)
- C. Polyarteritis nodosa (PAN)
- D. Granulomatosis with Polyangiitis (GPA)
Ischemic Optic Neuropathies Explanation: ***Giant cell arteritis (GCA)***
- **Jaw claudication** or tightness, difficulty chewing, and pain in the jaw are classic symptoms of GCA, resulting from **ischemia of the masticatory muscles**. [1]
- This condition is a **large vessel vasculitis** that frequently affects the **temporal arteries** and can lead to blindness if untreated. [1]
*Polyarteritis nodosa (PAN)*
- PAN is a **necrotizing vasculitis** that typically affects **medium-sized arteries**, often sparing the pulmonary circulation. [1]
- Common symptoms include **neuropathy**, abdominal pain, and skin lesions (e.g., livedo reticularis), but **jaw tightness is not a typical feature**.
*Coarctation of aorta*
- This is a **congenital narrowing of the aorta**, leading to symptoms like **upper extremity hypertension**, headache, and claudication in the lower extremities.
- **Jaw tightness is not a symptom** associated with coarctation of the aorta.
*Granulomatosis with Polyangiitis (GPA)*
- GPA is a **small-vessel vasculitis** characterized by **granulomatous inflammation** involving the upper and lower respiratory tracts, and glomerulonephritis.
- Symptoms often include **sinusitis**, lung nodules, and kidney disease, but **jaw claudication is not a characteristic presentation**.
Ischemic Optic Neuropathies Indian Medical PG Question 3: Which of the following is the MOST common condition caused by hypernatremia?
- A. Altered mental status
- B. Brain hemorrhage
- C. Seizure (Correct Answer)
- D. Central pontine myelinosis
Ischemic Optic Neuropathies Explanation: ***Seizure***
- While not the *most* common initial symptom, **seizure** can be a severe manifestation of hypernatremia, particularly when the serum sodium levels rise rapidly or to very high concentrations leading to significant neuronal dehydration.
- **Rapid correction of severe hypernatremia** can also induce seizures if the brain cells swell too quickly.
*Altered mental status*
- **Altered mental status** such as lethargy, confusion, or irritability, is a very common and often an earlier symptom of hypernatremia due to neuronal dehydration and intracellular water shifts, but it generally precedes more severe neurological complications like seizures.[1]
- It is a broad term that encompasses a range of neurological dysfunctions, and while frequent, it is not as specific a severe endpoint as a seizure.
*Brain hemorrhage*
- **Brain hemorrhage** is a rare and severe complication of hypernatremia, primarily seen when extreme osmotic shifts cause significant brain shrinkage, leading to tension on bridging veins and potential rupture.
- This is not a common presentation and typically occurs only in very severe cases of hypernatremia or during overly rapid correction.
*Central pontine myelinosis*
- **Central pontine myelinolysis (CPM)** is a neurological disorder caused by too rapid correction of *chronic hyponatremia*, not hypernatremia.[1]
- It results from osmotic damage to myelin sheaths in the pons, leading to severe neurological deficits such as dysphagia, dysarthria, and even locked-in syndrome.[1]
Ischemic Optic Neuropathies Indian Medical PG Question 4: Sudden loss of vision without pain - Which of the following is NOT a cause?
- A. CRAO
- B. CSR
- C. Acute congestive glaucoma (Correct Answer)
- D. Vitreous Hemorrhage
Ischemic Optic Neuropathies Explanation: ***Acute congestive glaucoma***
- This condition is characterized by **sudden, severe eye pain** along with blurred vision, redness, and a fixed, mid-dilated pupil.
- The pain arises from abrupt elevation of **intraocular pressure**, which differentiates it from painless vision loss.
*CRAO*
- **Central Retinal Artery Occlusion** (CRAO) typically presents as **sudden, profound, painless monocular vision loss**.
- Funduscopic examination often reveals a **cherry-red spot** in the fovea with generalized retinal whitening.
*CSR*
- **Central Serous Retinopathy** (CSR) causes **sudden, painless blurred vision** or a scotoma, often described as a "watery" or "shimmering" effect.
- It involves leakage of fluid under the retina, typically in the macula.
*Vitreous Hemorrhage*
- Presents as **sudden, painless loss of vision** or a shower of floaters, often described as cobwebs or clouds.
- It results from bleeding into the **vitreous cavity**, which can obscure the retina.
Ischemic Optic Neuropathies Indian Medical PG Question 5: A 70-year-old woman is seen by her physician for evaluation of severe headaches. She noted these several weeks ago, and they have been getting worse. Although she has not had any visual aura but she has been intermittently losing vision in her left eye for the last few days. She denies new weakness or numbness, but she does reports jaw pain with eating. Her past medical history includes coronary artery disease requiring a bypass grafting 10 years prior, diabetes mellitus, hyperlipidaemia, and mild depression. Full review of symptoms is notable for night sweats and mild low back pain particularly prominent in the morning. Which of the following is the next most appropriate step?
- A. Immediate initiation of glucocorticoid (Correct Answer)
- B. Aspirin 975 mg orally daily
- C. Measurement of erythrocyte sedimentation rate
- D. Referral for temporal artery biopsy
Ischemic Optic Neuropathies Explanation: ### Immediate initiation of glucocorticoids
- The patient's symptoms, including **severe headaches**, **transient vision loss (amaurosis fugax)**, **jaw claudication**, and **systemic symptoms** like night sweats in an elderly woman, are highly suggestive of **giant cell arteritis (GCA)**. [1]
- **Prompt initiation of high-dose glucocorticoids** is crucial to prevent irreversible vision loss, which is a devastating complication of GCA. [1]
*Aspirin 975 mg orally daily*
- While aspirin may be considered as an adjunct in treating GCA to reduce thrombotic complications, it is **not the primary or immediate treatment** for the disease itself.
- **High-dose aspirin** is typically not used for GCA and would not address the underlying inflammation causing ocular ischemia.
*Measurement of erythrocyte sedimentation rate*
- An **elevated ESR** is characteristic of GCA and can support the diagnosis. [1]
- However, performing this test first would **delay crucial treatment** for GCA, potentially leading to permanent vision loss. [1]
*Referral for temporal artery biopsy*
- A **temporal artery biopsy** is the gold standard for confirming the diagnosis of GCA but should **not delay the initiation of glucocorticoids**. [1]
- Treatment should begin immediately based on clinical suspicion, and the biopsy can be performed safely within **1-2 weeks of starting steroids** without significantly impacting diagnostic yield. [1]
Ischemic Optic Neuropathies Indian Medical PG Question 6: True about sympathetic ophthalmia?
- A. It is caused due to corneal injury
- B. It is bilateral non granulomatous uveitis
- C. Dalen Fuch's Nodules are seen (Correct Answer)
- D. Paton's Lines are seen
Ischemic Optic Neuropathies Explanation: ***Dalen Fuch's Nodules are seen***
- **Dalen-Fuchs nodules** are characteristic histological findings in sympathetic ophthalmia, consisting of epithelioid cells and lymphocytes between the retinal pigment epithelium and Bruch's membrane.
- Their presence is a key diagnostic indicator in the affected eye (sympathizing eye) and the exciting eye (initial injured eye).
*It is caused due to corneal injury*
- Sympathetic ophthalmia is typically triggered by **penetrating ocular trauma** or **intraocular surgery** involving the **uvea**, not merely corneal injury.
- The exposure of **uveal antigens** to the immune system after injury is the initiating event.
*It is bilateral non granulomatous uveitis*
- Sympathetic ophthalmia is a **bilateral, granulomatous panuveitis**, meaning it involves all layers of the uvea and is characterized by granuloma formation.
- The granulomatous nature with **epithelioid cells** and **giant cells** is a hallmark.
*Paton's Lines are seen*
- **Paton's lines** are radially oriented retinal folds seen around the optic disc, characteristic of **papilledema**.
- They are not associated with sympathetic ophthalmia, which primarily affects the uvea and retina due to an autoimmune response.
Ischemic Optic Neuropathies Indian Medical PG Question 7: Which drug does NOT cause optic neuropathy?
- A. Chloramphenicol
- B. Penicillin (Correct Answer)
- C. Ethambutol
- D. INH
Ischemic Optic Neuropathies Explanation: ***Penicillin***
- Penicillin is a widely used antibiotic that is **not associated with optic neuropathy**
- Its primary side effects are **allergic reactions and hypersensitivity**
- Visual disturbances or optic nerve damage are **not characteristic** of penicillin therapy
*Chloramphenicol*
- Known to cause **dose-dependent and duration-dependent optic neuropathy**, especially with prolonged use
- Can lead to visual impairment, including reduced visual acuity and color vision defects
- May be **irreversible** in some cases
*Ethambutol*
- **Most notorious** antitubercular drug for causing optic neuritis
- Causes **dose-dependent bilateral visual loss** and **red-green color blindness**
- Requires regular visual monitoring during therapy
- Potentially **irreversible** optic nerve damage
*INH (Isoniazid)*
- Can cause optic neuropathy, though **less frequently** than ethambutol
- Usually associated with **high doses** or prolonged therapy
- Risk increases in slow acetylators and those with nutritional deficiencies
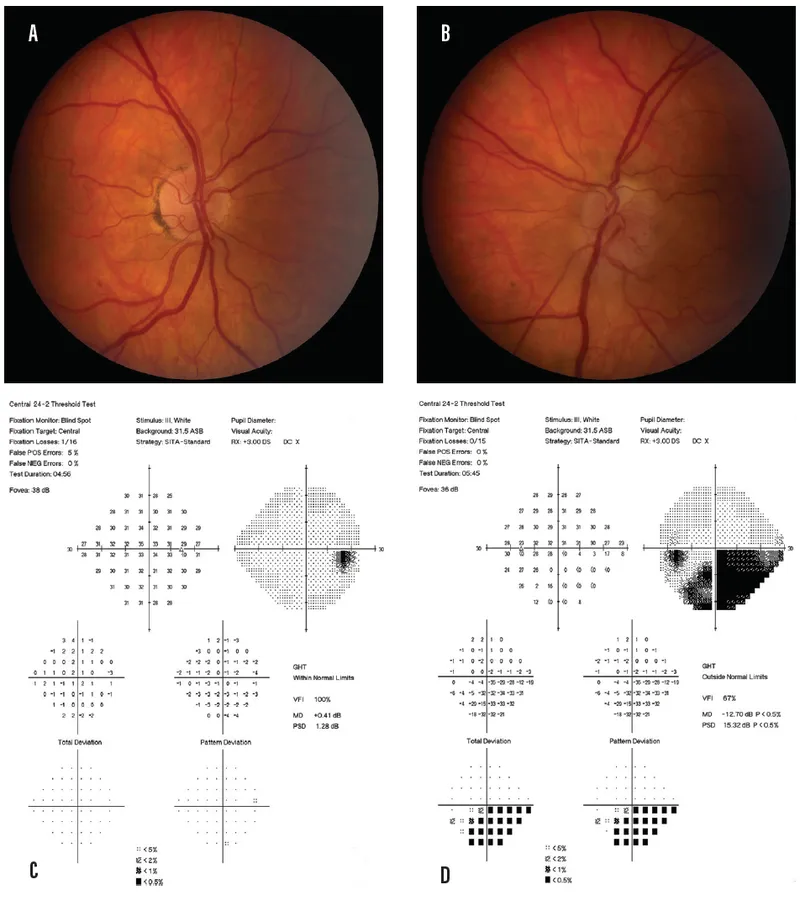
Ischemic Optic Neuropathies Indian Medical PG Question 8: Identify the visual field defect shown in the image.
- A. Binasal hemianopia
- B. Bitemporal hemianopia (Correct Answer)
- C. Homonymous hemianopia
- D. Altitudinal defect
Ischemic Optic Neuropathies Explanation: ***Bitemporal hemianopia***
- The image shows loss of vision in the **temporal (outer) halves of both visual fields**, which is characteristic of bitemporal hemianopia.
- This defect typically results from a lesion at the **optic chiasm**, compressing the crossing nasal retinal fibers, often due to a **pituitary tumor**.
*Binasal hemianopia*
- This condition involves visual loss in the **nasal (inner) halves of both visual fields**, which is the opposite of what is depicted.
- It is a rare defect that can be caused by lesions affecting the **uncrossed temporal retinal fibers** on both sides, such as from bilateral carotid artery aneurysms.
*Homonymous hemianopia*
- A homonymous hemianopia involves the **same half of the visual field in both eyes** (e.g., right visual field loss in both eyes), resulting from a lesion posterior to the optic chiasm.
- The image clearly shows different halves affected in each eye (temporal fields), not the same half.
*Altitudinal defect*
- An altitudinal defect involves the **loss of vision in the upper or lower half of the visual field** in one or both eyes, respecting the horizontal midline.
- The visual field loss shown in the image is vertical, affecting the temporal halves, not the upper or lower halves.
Ischemic Optic Neuropathies Indian Medical PG Question 9: Early fundoscopic sign in papilloedema is
- A. Blurring of the disc margin (Correct Answer)
- B. Hyperemia of the disc
- C. Splinter hemorrhages
- D. Blurring of the peripapillary nerve fiber layer
Ischemic Optic Neuropathies Explanation: ***Blurring of the disc margin***
- The earliest fundoscopic sign of **papilledema** is the blurring of the superior and inferior optic disc margins, followed by nasal and then temporal margins.
- This blurring is due to the **axoplasmic stasis** and edema in the optic nerve head caused by increased intracranial pressure.
*Hyperemia of the disc*
- While disc **hyperemia** (redness) can occur in papilledema, it typically manifests after the initial blurring of the disc margins.
- It results from **venous engorgement** and capillary dilation within the swollen optic disc.
*Splinter hemorrhages*
- **Splinter hemorrhages** on or near the optic disc are a sign of more advanced or rapidly progressive papilledema, indicating capillary rupture.
- These are not usually the *earliest* sign but suggest severe **venous congestion**.
*Blurring of the peripapillary nerve fiber layer*
- While the **peripapillary nerve fiber layer** does become edematous and blurred in papilledema, the **disc margin blurring** is the *initial* and most characteristic sign identifying the onset of the condition.
- This occurs as part of the overall swelling but is often preceded by changes directly at the disc boundary.
Ischemic Optic Neuropathies Indian Medical PG Question 10: Which of the following investigations is not necessary for evaluating optic neuritis?
- A. MRI of the head and orbit
- B. Erythrocyte Sedimentation Rate (ESR)
- C. Ultrasonography B-scan (Correct Answer)
- D. Visual fields assessment
Ischemic Optic Neuropathies Explanation: **Explanation:**
Optic neuritis is an inflammatory condition of the optic nerve, most commonly associated with Multiple Sclerosis (MS). The diagnosis is primarily clinical, but investigations are focused on confirming the diagnosis, assessing the extent of damage, and determining the risk of systemic demyelination.
**Why B-scan is the correct answer:**
**Ultrasonography B-scan** is used to visualize the posterior segment of the eye when the media (cornea, lens, or vitreous) is opaque. It is useful for detecting retinal detachment, vitreous hemorrhage, or intraocular tumors. It has no diagnostic value in optic neuritis because the pathology is retrobulbar or involves the nerve fibers, which are better visualized via neuroimaging.
**Why the other options are necessary:**
* **MRI of the head and orbit (with Gadolinium):** This is the most important investigation. It confirms optic nerve inflammation (showing enhancement) and identifies white matter plaques in the brain, which are crucial for predicting the risk of developing Multiple Sclerosis.
* **Erythrocyte Sedimentation Rate (ESR):** While optic neuritis is usually idiopathic or demyelinating, ESR is checked to rule out inflammatory or systemic autoimmune mimics, such as Neuromyelitis Optica (NMO) or giant cell arteritis in older patients.
* **Visual fields assessment:** Automated perimetry (e.g., Humphrey Visual Field) is essential to document the type of defect. The most common finding is a **central or centrocecal scotoma**.
**Clinical Pearls for NEET-PG:**
* **Classic Triad:** Sudden unilateral vision loss, periocular pain (worsened by eye movement), and dyschromatopsia (impaired red-green color vision).
* **Marcus Gunn Pupil:** A Relative Afferent Pupillary Defect (RAPD) is a hallmark sign.
* **Pulfrich Phenomenon:** Objects moving in a straight line appear to move in curved paths due to delayed conduction in the affected nerve.
* **Uhthoff’s Phenomenon:** Temporary worsening of symptoms with increased body temperature (e.g., after a hot bath or exercise).
More Ischemic Optic Neuropathies Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.