Ocular Pathology Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Ocular Pathology. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Ocular Pathology Indian Medical PG Question 1: A 45-year-old diabetic presents with sudden painless vision loss. Cotton wool spots and dot hemorrhages seen. HbA1c is 9.2. Most likely diagnosis?
- A. Hypertensive retinopathy
- B. CRAO
- C. Diabetic retinopathy (Correct Answer)
- D. CRVO
Ocular Pathology Explanation: ***Diabetic retinopathy***
- The presence of **cotton wool spots** and **dot hemorrhages** in a diabetic patient with poor glycemic control (HbA1c 9.2) are classic signs of **diabetic retinopathy**.
- **Painless vision loss** is a common presentation, especially with macular edema or proliferative disease.
*Hypertensive retinopathy*
- While cotton wool spots can be seen, **dot hemorrhages are less characteristic** than flame-shaped hemorrhages.
- The primary driver here is **diabetes** and poor glycemic control, not necessarily hypertension as the main cause.
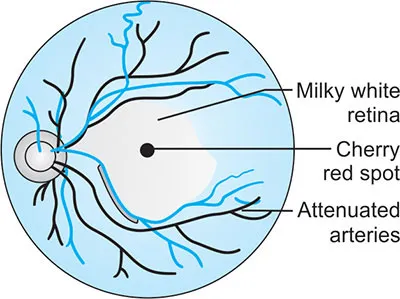
*CRAO*
- **Central retinal artery occlusion** typically presents with **sudden, profound, painless monocular vision loss**.
- Funduscopic examination would reveal a **cherry-red spot** and **pale retina**, not cotton wool spots and dot hemorrhages.
*CRVO*
- **Central retinal vein occlusion** is characterized by **extensive retinal hemorrhages** (often described as "blood and thunder" appearance), tortuous veins, and optic disc edema.
- While it can cause painless vision loss and some hemorrhages, the specific combination of **cotton wool spots and dot hemorrhages** in a diabetic context points more strongly to diabetic retinopathy.
Ocular Pathology Indian Medical PG Question 2: In primary open-angle glaucoma (POAG), which of the following findings is NOT typically seen?
- A. Bayoneting sign (arteriovenous crossing changes)
- B. Peripapillary atrophy
- C. Horizontal cupping of the optic disc
- D. Macular edema (Correct Answer)
Ocular Pathology Explanation: ***Macular edema***
- **Macular edema** is characterized by fluid accumulation in the fovea or retina, causing blurry vision and metamorphopsia.
- While it can occur in conditions like **diabetic retinopathy** or **uveitis**, it is **not a typical finding in POAG**, which primarily affects the optic nerve.
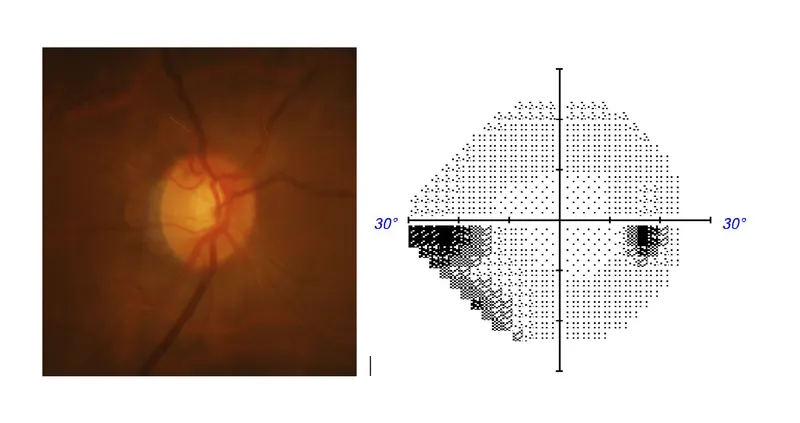
*Horizontal cupping of the optic disc*
- **Horizontal cupping** (or vertical elongation of the optic cup) is a common sign of **glaucomatous damage**, reflecting the loss of retinal ganglion cells.
- This morphological change suggests the progression of optic nerve atrophy.
*Bayoneting sign (arteriovenous crossing changes)*
- The **bayoneting sign**, where blood vessels appear to dip below the optic disc margin and then sharply bend, is a feature of **advanced glaucomatous cupping**.
- It indicates significant loss of optic nerve tissue and is often associated with deeply excavated optic discs.
*Peripapillary atrophy*
- **Peripapillary atrophy** (PPA) refers to areas of RPE and choroidal atrophy surrounding the optic disc, commonly seen in glaucoma.
- While its presence and extent may correlate with **glaucoma severity**, it is a recognized clinical feature of the disease.
Ocular Pathology Indian Medical PG Question 3: Recurrent anterior uveitis with increased intraocular tension is seen in which of the following conditions?
- A. Posner-Schlossman syndrome (Correct Answer)
- B. Foster-Kennedy syndrome
- C. Vogt-Koyanagi-Harada syndrome
- D. Fuchs heterochromic iridocyclitis
Ocular Pathology Explanation: ***Posner-Schlossman syndrome***
- Characterized by **recurrent, unilateral, non-granulomatous anterior uveitis** associated with markedly **elevated intraocular pressure (IOP)**.
- The condition is also known as **glaucomatocyclitic crisis**, highlighting the episodic inflammation and glaucoma.
- Key features include **acute attacks** lasting hours to weeks with **dramatic IOP elevation** (often >40 mmHg).
*Foster-Kennedy syndrome*
- This syndrome is defined by ipsilateral **optic atrophy**, contralateral **papilledema**, and often **anosmia**, typically due to a frontal lobe tumor.
- It does not involve anterior uveitis or primary elevated intraocular tension.
- This is a neuro-ophthalmologic syndrome, not an inflammatory ocular condition.
*Vogt-Koyanagi-Harada syndrome*
- An autoimmune disorder affecting pigmented tissues, leading to **bilateral granulomatous panuveitis**, often with hearing loss, vitiligo, poliosis, and neurological symptoms.
- While it involves uveitis, it is typically **bilateral and panuveitis**, not recurrent unilateral anterior uveitis.
- IOP may be elevated but not the defining feature with dramatic episodic rises.
*Fuchs heterochromic iridocyclitis*
- A chronic, **unilateral, low-grade anterior uveitis** with characteristic iris heterochromia.
- May have mild IOP elevation but **not recurrent episodic attacks** with marked pressure spikes.
- Inflammation is typically **quiet and chronic** rather than acute and recurrent.
Ocular Pathology Indian Medical PG Question 4: A 5 year old child who presented with proptosis of one of the eyes was found to have a desmin positive tumour. What is the probable diagnosis?
- A. Neuroblastoma
- B. Retinoblastoma
- C. Rhabdomyosarcoma (Correct Answer)
- D. Ewing's sarcoma
Ocular Pathology Explanation: ***Rhabdomyosarcoma***
- **Desmin positivity** is a characteristic immunohistochemical feature of **rhabdomyosarcoma**, as desmin is an intermediate filament found in muscle cells [1].
- In a 5-year-old child presenting with **proptosis**, rhabdomyosarcoma of the orbit is a highly probable diagnosis, as it is the most common primary malignant orbital tumor in childhood [3].
*Neuroblastoma*
- Neuroblastoma is typically a tumor of neural crest origin, with classic immunohistochemical markers being **neuron-specific enolase (NSE)** and **chromogranin**, not desmin [2].
- While it can manifest with orbital metastases leading to proptosis, the desmin positivity rules it out as the primary diagnosis [3].
*Retinoblastoma*
- Retinoblastoma is a malignant tumor of the retina, presenting with **leukocoria** (white pupillary reflex) and occasionally proptosis in advanced stages [4].
- It arises from neuroectodermal cells, and its characteristic markers include **synaptophysin** and **neuron-specific enolase (NSE)**, not desmin [4].
*Ewing's sarcoma*
- Ewing's sarcoma is a primary malignant small round blue cell tumor of bone and soft tissue, typically marked by expression of **CD99** and a characteristic **t(11;22) translocation**.
- While it can occur in the orbit, it is not desmin positive, making rhabdomyosarcoma a more likely diagnosis given the immunohistochemical findings.
**References:**
[1] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. Bones, Joints, and Soft Tissue Tumors, pp. 1224-1225.
[2] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. (Basic Pathology) introduces the student to key general principles of pathology, both as a medical science and as a clinical activity with a vital role in patient care. Part 2 (Disease Mechanisms) provides fundamental knowledge about the cellular and molecular processes involved in diseases, providing the rationale for their treatment. Part 3 (Systematic Pathology) deals in detail with specific diseases, with emphasis on the clinically important aspects., pp. 211-212.
[3] Kumar V, Abbas AK, et al.. Robbins and Cotran Pathologic Basis of Disease. 9th ed. The Central Nervous System, pp. 1323-1324.
[4] Cross SS. Underwood's Pathology: A Clinical Approach. 6th ed. Common Clinical Manifestations Of Central And Peripheral Nervous System Disease, pp. 737-738.
Ocular Pathology Indian Medical PG Question 5: MC site of basal cell carcinoma of eyelid:
- A. Medial canthus
- B. Lower eyelid (Correct Answer)
- C. Upper eyelid
- D. Outer canthus
Ocular Pathology Explanation: ***Lower eyelid***
- The **lower eyelid** is the most common site for basal cell carcinoma (BCC) of the eyelid, accounting for approximately **50-60%** of all eyelid BCCs.
- This high frequency is due to increased exposure to **UV radiation**, which is the primary risk factor for BCC development.
- BCC often presents as a **pearly nodule** with telangiectasias and central ulceration, frequently found on the lower lid margin.
*Medial canthus*
- The medial canthus is the **second most common site**, accounting for approximately **25-30%** of eyelid BCCs.
- Tumors in this area can be **more aggressive** and challenging to treat due to proximity to the lacrimal system and orbital structures.
- Medial canthal BCCs may require more extensive surgical reconstruction.
*Upper eyelid*
- The upper eyelid accounts for only **10-15%** of eyelid BCCs, making it significantly **less common** than the lower eyelid.
- This is due to **less direct sun exposure** compared to the lower lid, as the upper lid is often shaded by the brow.
*Outer canthus*
- The outer (lateral) canthus is the **least common site**, accounting for only about **5%** of eyelid BCCs.
- Tumors here may present with similar features but are much less frequently encountered than those on the lower lid or medial canthus.
Ocular Pathology Indian Medical PG Question 6: All are seen in non-proliferative diabetic retinopathy except which of the following?
- A. Microaneurysm
- B. Neovascularization (Correct Answer)
- C. Cotton wool spots
- D. Retinal hemorrhages
Ocular Pathology Explanation: ***Neovascularization***
- **Neovascularization** signifies the growth of new, fragile blood vessels and is a hallmark feature of **proliferative diabetic retinopathy**, not non-proliferative.
- These new vessels can bleed, leading to vitreous hemorrhage and tractional retinal detachment, which are severe complications.
*Microaneurysm*
- **Microaneurysms** are the earliest clinical sign of diabetic retinopathy, visible as small, red dots on funduscopic examination due to capillary outpouchings.
- They are characteristic findings in **non-proliferative diabetic retinopathy (NPDR)**.
*Cotton wool spots*
- **Cotton wool spots** are soft exudates resulting from microinfarcts in the retinal nerve fiber layer due to occluded precapillary arterioles.
- They are findings commonly seen in **non-proliferative diabetic retinopathy (NPDR)**.
*Retinal hemorrhages*
- **Retinal hemorrhages** (dot-blot hemorrhages) occur when blood leaks from damaged capillaries in the retina.
- They are a common occurrence in **non-proliferative diabetic retinopathy (NPDR)**.
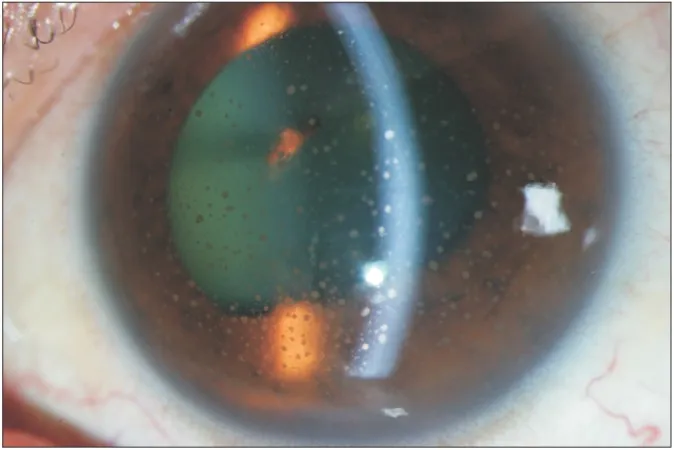
Ocular Pathology Indian Medical PG Question 7: A 76-year-old female presents with difficulty reading. Bilateral white opacifications consistent with cataract formation are observed. In which structure are these opacifications located?
- A. Aqueous humor
- B. Cornea
- C. Lens (Correct Answer)
- D. Optic nerve
Ocular Pathology Explanation: ***Lens***
- **Cataracts** are defined by the **clouding of the natural lens** of the eye, which causes blurred vision and difficulty with activities like reading.
- The condition is very common, especially among older adults, and affects the **bilateral vision** as described in the case.
*Aqueous humor*
- The **aqueous humor** is a clear fluid that fills the space between the cornea and the lens; it is not the structure that becomes opaque in cataracts.
- Problems with aqueous humor are typically associated with glaucoma (due to increased intraocular pressure) rather than cataract formation.
*Cornea*
- The **cornea** is the transparent outer layer of the eye that helps focus light, but it does not develop cataracts.
- Opacities in the cornea (e.g., from injuries or infections) would be described differently and produce different visual symptoms.
*Optic nerve*
- The **optic nerve** transmits visual information from the retina to the brain; it is a nerve, not a structure where light focuses or where cataracts develop.
- Damage to the optic nerve typically leads to vision loss or blind spots, not blurred vision from opacification.
Ocular Pathology Indian Medical PG Question 8: A patient with cataract presents with pain and redness of eye. On examination he had deep anterior chamber. What is the diagnosis?
- A. Acute phacolytic glaucoma (Correct Answer)
- B. Acute angle closure glaucoma
- C. Acute neovascular glaucoma
- D. Acute phacomorphic glaucoma
Ocular Pathology Explanation: ***Acute phacolytic glaucoma***
- This condition occurs when **lens proteins leak** from a mature or hypermature cataract into the aqueous humor, causing an inflammatory reaction and **trabecular meshwork obstruction**, leading to elevated intraocular pressure.
- The presence of a **deep anterior chamber** distinguishes it from phacomorphic glaucoma, which is characterized by a shallow anterior chamber due to lens intumescence.
*Acute angle closure glaucoma*
- This typically presents with a **shallow anterior chamber** as the iris bows forward, blocking the trabecular meshwork.
- While it causes pain and redness, the deep anterior chamber described in the patient makes this diagnosis unlikely.
*Acute neovascular glaucoma*
- This type of glaucoma results from the formation of **new blood vessels** on the iris and in the angle of the anterior chamber, often due to conditions like **diabetic retinopathy** or **retinal vein occlusion**.
- There is no mention of such predisposing factors or visible neovascularization in the patient's presentation.
*Acute phacomorphic glaucoma*
- This condition is caused by the **intumescence (swelling) of a cataractous lens**, which pushes the iris forward, leading to a **shallow anterior chamber** and angle closure.
- The patient's presentation of a **deep anterior chamber** rules out phacomorphic glaucoma.
Ocular Pathology Indian Medical PG Question 9: Consider the following causes of visual loss :
1. Obstruction of the central retinal artery
2. Vitreous and retinal haemorrhage
3. Cataract
4. Retinal detachment Which of the above causes are associated with acute visual loss in a patient?
- A. 1, 3 and 4
- B. 1, 2 and 3
- C. 2, 3 and 4
- D. 1, 2 and 4 (Correct Answer)
Ocular Pathology Explanation: ***1, 2 and 4***
- **Obstruction of the central retinal artery**, **vitreous and retinal haemorrhage**, and **retinal detachment** all present as sudden, acute vision loss.
- **Central retinal artery occlusion** causes complete, sudden, painless monocular vision loss. **Vitreous hemorrhage** is acute, painless, and can present with floaters or red haze. **Retinal detachment** is acute, painless vision loss, often preceded by flashes and floaters, and can present as a "curtain" coming across the vision.
*1, 3 and 4*
- While **central retinal artery obstruction** and **retinal detachment** cause acute vision loss, **cataracts** typically cause gradual, progressive vision loss over months to years.
- Cataracts primarily affect lens clarity, leading to blurry vision, glare, and dull colors rather than an abrupt onset of blindness.
*1, 2 and 3*
- **Central retinal artery obstruction** and **vitreous/retinal hemorrhage** lead to acute vision loss, but **cataracts** are a cause of *chronic* and *gradual* vision impairment.
- The onset and progression of a **cataract** are distinctly different from the sudden nature of acute vision loss conditions.
*2, 3 and 4*
- **Vitreous and retinal haemorrhage** and **retinal detachment** are causes of acute vision loss, but a **cataract** is not.
- The defining characteristic of acute vision loss is its rapid onset, which does not align with the slow development of a cataract.
Ocular Pathology Indian Medical PG Question 10: What is the first-line treatment for acute angle closure glaucoma?
- A. Pilocarpine
- B. Beta blocker eyedrops
- C. IV mannitol
- D. Acetazolamide (Correct Answer)
Ocular Pathology Explanation: **Acetazolamide**
- **Acetazolamide** (oral or intravenous) is a carbonic anhydrase inhibitor that rapidly reduces intraocular pressure by decreasing aqueous humor production, making it the **first-line medical treatment** for acute angle-closure glaucoma.
- While other agents are used, acetazolamide provides the quickest and most significant initial reduction in **intraocular pressure (IOP)**, which is crucial in preventing permanent vision loss.
*IV mannitol*
- **Intravenous mannitol** is an osmotic diuretic used to draw fluid from the vitreous humor to lower **IOP** significantly, but it is typically reserved for cases where **acetazolamide** alone is insufficient or for very high **IOPs**.
- It is often considered a second-line or adjunctive agent rather than the initial first-line treatment.
*Pilocarpine*
- **Pilocarpine** is a miotic agent that constricts the pupil, which helps to pull the iris away from the trabecular meshwork and open the angle.
- However, it should only be administered *after* the **intraocular pressure** has been significantly lowered (e.g., with acetazolamide), as it can worsen angle closure in an inflamed eye with very high **IOP**.
*Beta blocker eyedrops*
- **Topical beta-blockers** (e.g., timolol) reduce **IOP** by decreasing aqueous humor production and are a common treatment for various types of glaucoma.
- While useful in acute angle-closure glaucoma, they act more slowly than **acetazolamide** and are typically used as an adjunct rather than the sole initial first-line treatment.
More Ocular Pathology Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.