Otologic Trauma Indian Medical PG Practice Questions and MCQs
Practice Indian Medical PG questions for Otologic Trauma. These multiple choice questions (MCQs) cover important concepts and help you prepare for your exams.
Otologic Trauma Indian Medical PG Question 1: Which of the following is false regarding cranial trauma?
- A. Depressed skull is associated with brain injury at the immediate area of impact
- B. Raccoon eyes seen in subgaleal hemorrhage (Correct Answer)
- C. Carotid-cavernous fistula occur in base skull
- D. Post traumatic epilepsy seen in 15%
Otologic Trauma Explanation: ***Raccoon eyes seen in subgaleal hemorrhage***
- **Raccoon eyes** (periorbital ecchymosis) are typically seen with **anterior cranial fossa fractures**, not subgaleal hemorrhage.
- Subgaleal hemorrhage is a collection of blood between the galea aponeurotica and the periosteum, usually causing diffuse **scalp swelling**.
*Depressed skull is associated with brain injury at the immediate area of impact*
- A depressed skull fracture means a portion of the skull is pushed inward, directly impacting the underlying **brain tissue**.
- This can lead to localized **contusions**, **lacerations**, or **hematomas** at the site of impact.
*Carotid-cavernous fistula occur in base skull*
- **Carotid-cavernous fistulas** (CCF) commonly result from **traumatic rupture** of the internal carotid artery within the **cavernous sinus**.
- This type of injury is often associated with **severe skull base fractures**, particularly those involving the sphenoid bone.
*Post traumatic epilepsy seen in 15%*
- The incidence of **post-traumatic epilepsy** (PTE) after severe head injury ranges from 5% to 15%, making 15% a plausible, though upper-end, estimate.
- Risk factors for PTE include **depressed skull fractures**, **intracranial hematomas**, and **early seizures**.
Otologic Trauma Indian Medical PG Question 2: The preferred site of incision for myringotomy in ASOM (Acute Suppurative Otitis Media) to drain the middle ear is:
- A. Anteroinferior
- B. Posteroinferior (Correct Answer)
- C. Anterosuperior
- D. Posterosuperior
Otologic Trauma Explanation: ***Posteroinferior***
- The **posteroinferior quadrant** of the tympanic membrane is the preferred site for myringotomy in **acute suppurative otitis media (ASOM)** due to its relative avascularity and safety regarding middle ear structures.
- This location allows for adequate drainage of pus and prevents re-accumulation, without damaging essential structures like the **ossicular chain** or the **facial nerve**.
*Anteroinferior*
- This quadrant is generally avoided because it provides less effective drainage and carries a higher risk of injury to the **Eustachian tube orifice** or other anterior structures.
- The **handle of the malleus** runs posteriorly, and an incision here might be less effective for gravity-assisted drainage.
*Anterosuperior*
- The **anterosuperior quadrant** is not typically chosen due to its proximity to the **ossicular chain** attachments and potentially larger blood vessels, increasing the risk of bleeding and injury.
- Incisions in this region are often less effective for draining fluids that tend to collect in the more dependent parts of the middle ear.
*Posterosuperior*
- While somewhat accessible, the **posterosuperior quadrant** carries a higher risk of damaging the **incus** and **stapes**, as well as the **facial nerve** or **chorda tympani nerve**.
- Its elevated position also makes it less ideal for gravity-dependent drainage of purulent fluid from the middle ear.
Otologic Trauma Indian Medical PG Question 3: A patient presents with vertigo, tinnitus, and head tilt. He underwent myringoplasty for the safe type of chronic suppurative otitis media (CSOM) 6 months back. What is your diagnosis?
- A. Paget disease
- B. Labyrinthitis
- C. Vestibular schwannoma
- D. Perilymphatic fistula (Correct Answer)
Otologic Trauma Explanation: ***Perilymphatic fistula***
- The combination of **vertigo**, **tinnitus**, and **head tilt** occurring after a **myringoplasty**, even for a safe type of CSOM, suggests a perilymphatic fistula.
- Myringoplasty can occasionally involve trauma to the **oval or round window**, leading to a direct communication between the inner ear (perilymph) and the middle ear, causing these symptoms.
*Paget disease*
- This is a **bone remodeling disorder** that primarily affects the skull, pelvis, and long bones, leading to bone pain and deformities.
- While it can cause hearing loss (due to otosclerosis) and a sense of imbalance, it does not typically present with the acute onset of **vertigo** and **tinnitus** following ear surgery.
*Labyrinthitis*
- **Labyrinthitis** is an inflammation of the inner ear, typically caused by a viral infection, leading to sudden, severe **vertigo**, **nausea**, and often **hearing loss** or **tinnitus**.
- While the symptoms of vertigo and tinnitus are present, the history of recent myringoplasty makes a **structural compromise** like a perilymphatic fistula a more specific diagnosis than generalized inflammation.
*Vestibular schwannoma*
- Also known as an acoustic neuroma, this is a **benign tumor** on the eighth cranial nerve, causing **gradual unilateral hearing loss**, **tinnitus**, and **imbalance**, but rarely sudden, intense vertigo unless very large.
- The presentation with a history of myringoplasty and acute symptoms makes a **spontaneous structural defect** more likely than a slowly growing tumor.
Otologic Trauma Indian Medical PG Question 4: A 35-year-old patient presents with hearing loss and discomfort in the right ear. Examination reveals keratin accumulation in the ear canal. What is the most likely diagnosis?
- A. Keratosis obturans (Correct Answer)
- B. Exostosis
- C. Cerumen
- D. Otitis externa
Otologic Trauma Explanation: ***Keratosis obturans***
- This condition is characterized by an **accumulation of desquamated keratin** and epithelial debris in the bony external auditory canal, leading to earache, conductive hearing loss, and sometimes widening of the ear canal.
- The patient's presentation of **hearing loss**, **discomfort in the right ear**, and **keratin accumulation** aligns directly with the description of keratosis obturans.
*Exostosis*
- Exostoses are **bony growths** in the ear canal, often associated with cold water exposure.
- While they can cause hearing loss and earwax impaction, they do not involve primary **keratin accumulation** as described.
*Cerumen*
- **Cerumen** is normal earwax, which is a mix of secretions and desquamated cells.
- While excessive cerumen can cause hearing loss, the description of **keratin accumulation** suggests a more organized, dense plug than typical cerumen impaction.
*Otitis externa*
- **Otitis externa** is an inflammation or infection of the ear canal, presenting with pain, redness, swelling, and discharge.
- While it can cause discomfort and sometimes lead to debris, the primary finding is **inflammation**, not specifically a large accumulation of keratin.
Otologic Trauma Indian Medical PG Question 5: The treatment of choice for atticoantral variety of chronic suppurative otitis media is:
- A. Mastoidectomy (Correct Answer)
- B. Medical management
- C. Underlay myringoplasty
- D. Insertion of ventilation tube
Otologic Trauma Explanation: **Correct: Mastoidectomy**
- The **atticoantral** variety of chronic suppurative otitis media (CSOM) is typically associated with **cholesteatoma**, which necessitates surgical eradication to prevent complications such as intracranial infection, facial nerve palsy, and labyrinthine destruction.
- **Mastoidectomy** is the treatment of choice to remove the cholesteatoma and achieve a safe, dry ear by clearing disease from the mastoid air cells and attic.
*Incorrect: Medical management*
- This approach is typically used for the **tubotympanic** (mucosal/safe) type of CSOM, which involves a central perforation without cholesteatoma.
- It is **ineffective in the presence of cholesteatoma**, as antibiotics cannot penetrate the keratinized debris matrix and do not eradicate the underlying pathology.
*Incorrect: Underlay myringoplasty*
- This procedure repairs a **tympanic membrane perforation** but does not address the underlying cholesteatoma or disease within the mastoid and attic.
- It is used for **safe, dry perforations**, usually associated with the tubotympanic type of CSOM after the ear has been rendered inactive.
*Incorrect: Insertion of ventilation tube*
- Ventilation tubes (grommets) are primarily used for **recurrent acute otitis media** or **otitis media with effusion (glue ear)** to equalize middle ear pressure and facilitate drainage.
- They are **not indicated for CSOM**, especially the atticoantral type with cholesteatoma, as they do not resolve the chronic infection or remove the pathological tissue.
Otologic Trauma Indian Medical PG Question 6: What is the diagnosis shown in the following image?
- A. Hyperinsulinism
- B. Conductive hearing defect
- C. Perichondritis (Correct Answer)
- D. Mucopolysaccharidosis
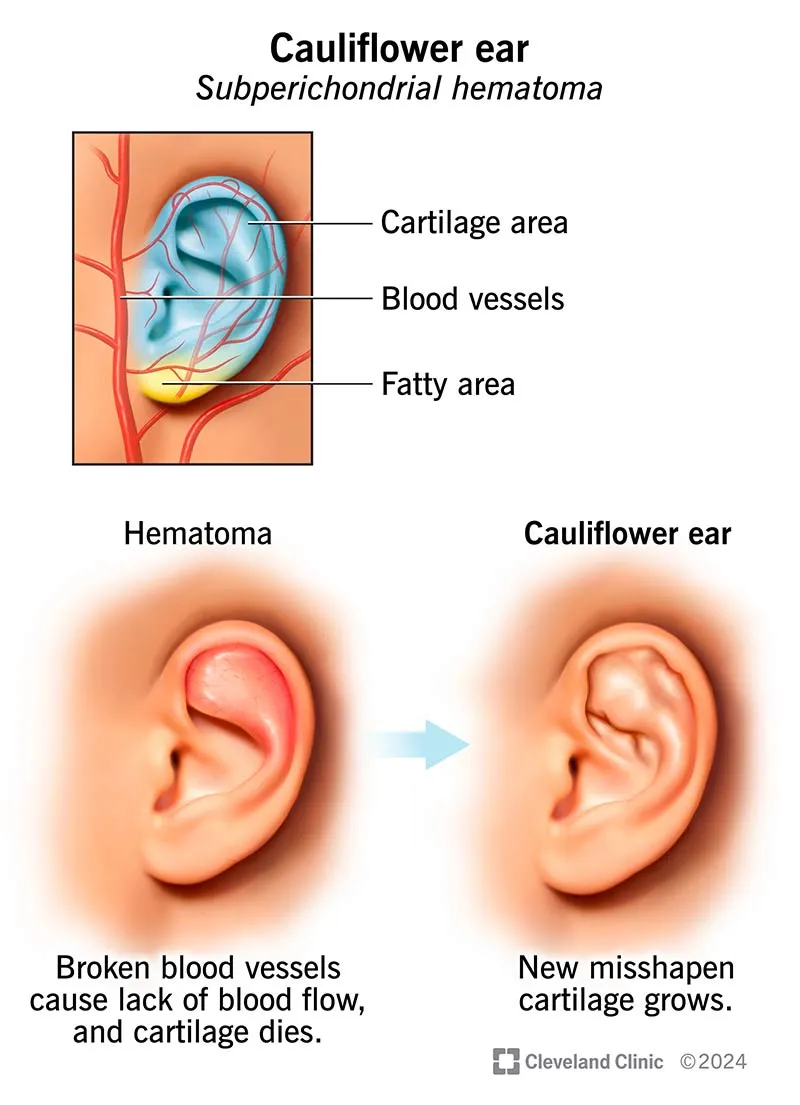
Otologic Trauma Explanation: ***Perichondritis***
- The image exhibits signs of **inflammation and swelling** of the external ear, consistent with **perichondritis**, an infection of the tissue surrounding the ear cartilage.
- This condition can lead to **redness**, **pain**, and fluid collection (abscess formation) that distorts the ear's normal architecture.
- Typically spares the **lobule** (which lacks cartilage) and presents as an **acute inflammatory condition**.
*Hyperinsulinism*
- **Hyperinsulinism** is a metabolic disorder characterized by excessive insulin secretion and has no relationship to external ear pathology.
- This is not an appropriate option for an acute inflammatory ear condition shown in clinical images.
*Conductive hearing defect*
- A **conductive hearing defect** is a functional diagnosis, not a structural/pathological diagnosis visible on examination.
- It refers to problems in sound transmission through the **external or middle ear**, but is not itself visible as inflammation or swelling.
- The image shows an **acute inflammatory condition**, not a hearing disorder.
*Mucopolysaccharidosis*
- **Mucopolysaccharidoses** are lysosomal storage disorders that can cause progressive dysmorphic facial features, including ear structure changes.
- However, these present with **chronic, diffuse structural changes** rather than acute inflammation and swelling.
- The acute inflammatory presentation in the image is inconsistent with this genetic storage disorder.
Otologic Trauma Indian Medical PG Question 7: Which of the following statements about tubercular otitis media is false?
- A. Spreads through the eustachian tube
- B. Usually affects only one ear
- C. Causes painful ear discharge (Correct Answer)
- D. May cause multiple perforations
Otologic Trauma Explanation: ***Causes painful ear discharge***
- **Pain** is typically an **absent or minimal symptom** in tubercular otitis media, even with significant ear discharge.
- The discharge is usually **thin, watery, and non-purulent**, reflecting the indolent nature of the infection.
*Spreads through the eustachian tube*
- Tubercular otitis media can spread via the **eustachian tube** from the nasopharynx, especially in cases of active pulmonary or pharyngeal tuberculosis.
- This is a common route for infectious agents to reach the middle ear.
*Usually affects only one ear*
- Tubercular otitis media predominantly presents as a **unilateral infection**.
- While bilateral involvement can occur, it is less common than unilateral presentation.
*May cause multiple perforations*
- Tubercular otitis media is notorious for causing **multiple, small perforations** in the tympanic membrane.
- This feature, often described as a "sieve-like" drum, is a characteristic diagnostic clue for the condition.
Otologic Trauma Indian Medical PG Question 8: Best surgery to relieve intractable vertigo in a Meniere's disease patient with profound hearing loss is?
- A. Vestibular neurectomy
- B. Endolymphatic sac decompression
- C. Cochleosacculotomy
- D. Surgical Labyrinthectomy (Correct Answer)
Otologic Trauma Explanation: **Surgical Labyrinthectomy**
* **Labyrinthectomy** is the most effective surgical option for intractable vertigo in Meniere's disease when the affected ear also has **profound hearing loss**, as it completely ablates the vestibular function of the inner ear.
* Since the patient already has profound hearing loss, the loss of residual hearing from this procedure is not a significant concern, making it an ideal choice for **vertigo control**.
*Vestibular neurectomy*
* **Vestibular neurectomy** is a highly effective procedure for intractable vertigo, as it aims to selectively cut the vestibular nerve while preserving hearing.
* However, it is a more complex surgical approach compared to labyrinthectomy and is typically reserved for patients with **serviceable hearing** that they wish to preserve.
*Endolymphatic sac decompression*
* **Endolymphatic sac decompression** is a surgical procedure designed to improve the reabsorption of endolymph, thereby reducing the pressure and symptoms of Meniere's disease, including vertigo and hearing loss.
* While it may improve vertigo symptoms, it is less consistently effective than ablative procedures for intractable vertigo and its primary benefit is to **preserve hearing**, which is not a priority in a patient with profound hearing loss.
*Cochleosacculotomy*
* **Cochleosacculotomy** involves making a small opening in the labyrinth to drain endolymph, aiming to reduce endolymphatic hydrops and alleviate vertigo.
* Though it can help with vertigo, it carries a high risk of causing complete hearing loss in the operated ear and offers less reliable vertigo control compared to a labyrinthectomy, especially when profound hearing loss is already present.
Otologic Trauma Indian Medical PG Question 9: Which of the following is correct about ear speculum insertion?
- A. Pinna : upward, backward and laterally; Tragus: forward (Correct Answer)
- B. Pinna : downward, backward and laterally; Tragus: forward
- C. Pinna : upward, backward and medially; Tragus: forward
- D. Pinna : upward, forward and laterally ; Tragus: forward
Otologic Trauma Explanation: ***Pinna : upward, backward and laterally; Tragus: forward***
- To properly visualize the **tympanic membrane** and ear canal in adults, the **pinna** (auricle) should be gently pulled **upward, backward, and laterally**. This maneuver helps to straighten the **ear canal**.
- The **tragus** should be gently pushed **forward** to stabilize the ear and facilitate speculum insertion, minimizing discomfort [1].
*Pinna : downward, backward and laterally; Tragus: forward*
- Pulling the **pinna downward** is typically recommended for **children** to straighten their ear canal.
- Doing so in adults may not adequately straighten the **ear canal**, hindering visualization.
*Pinna : upward, backward and medially; Tragus: forward*
- While pulling the pinna **upward and backward** is correct, pulling it **medially** would likely obstruct the view or cause discomfort.
- The goal is to open the **ear canal** for better visualization [1].
*Pinna : upward, forward and laterally ; Tragus: forward*
- Pulling the pinna **forward** would likely curl the helix and obstruct the **external auditory canal**, making it difficult to insert the speculum.
- The correct direction is **backward** to align the cartilaginous and bony parts of the canal [1].
Otologic Trauma Indian Medical PG Question 10: The cough response elicited while cleaning the external ear canal is mediated by stimulation of which nerve?
- A. The V cranial nerve
- B. Innervation of the external ear canal by C1 and C2
- C. The X cranial nerve (Correct Answer)
- D. Branches of the VII cranial nerve
Otologic Trauma Explanation: This phenomenon is known as **Arnold’s Reflex** (or the Ear-Cough Reflex). It occurs due to the stimulation of the **Auricular branch of the Vagus Nerve (Arnold’s Nerve)**, which provides sensory innervation to the posterior and inferior walls of the external auditory canal (EAC).
### Why the Correct Answer is Right:
When the EAC is stimulated (e.g., during syringing or cleaning with a cotton bud), sensory impulses are carried via the Vagus nerve (CN X) to the nucleus tractus solitarius in the brainstem. This triggers the efferent limb of the cough reflex, leading to an involuntary cough. This is a classic example of a referred reflex where stimulation of a peripheral nerve causes a response in a visceral organ system.
### Why Other Options are Incorrect:
* **Option A (V cranial nerve):** The Auriculotemporal branch of the Mandibular nerve (V3) supplies the anterior and superior walls of the EAC. While it carries sensation, it does not mediate the cough reflex.
* **Option B (C1 and C2):** The Greater Auricular nerve (C2, C3) supplies the skin over the mastoid and the lateral/lower part of the auricle, not the deep canal associated with this reflex.
* **Option C (VII cranial nerve):** The Facial nerve provides minor sensory innervation to the concha and retroauricular area (often involved in Ramsay Hunt Syndrome), but it is not responsible for the cough reflex.
### High-Yield Clinical Pearls for NEET-PG:
* **Arnold’s Nerve:** A branch of the Vagus (CN X).
* **Vagal Reflexes in ENT:** Stimulation of the EAC can occasionally cause **bradycardia or fainting** (Vaso-vagal syncope) due to the same nerve.
* **Hitchelberger’s Sign:** Reduced sensation in the area supplied by the facial nerve in the EAC, seen in Acoustic Neuroma.
* **Nerve Supply of EAC (Summary):**
1. Anterior/Superior: V3 (Auriculotemporal).
2. Posterior/Inferior: X (Arnold’s).
3. Concha/Posterior wall: VII (Facial).
More Otologic Trauma Indian Medical PG questions available in the OnCourse app. Practice MCQs, flashcards, and get detailed explanations.